
Balloon kyphoplasty provides a safe and effective minimally invasive option for osteoporotic vertebral compression fractures, it resulting in significant and sustained improvement in pain, functional status, and radiological parameters with minimal complications.
Dr. M. Sabarinath, Department of Spine, MIOT Hospital, Chennai, Tamil Nadu, India. E-mail: sabarimbbs79@gmail.com
Abstract
Introduction: Vertebral compression fractures (VCFs) affect significant portions of the body. Balloon kyphoplasty (BKP) is a minimally invasive treatment that offers pain relief and restoration of vertebral body height. This study aimed to determine the functional and radiological outcomes of patients with osteoporotic vertebral fractures treated with BKP.
Materials and Methods: This prospective study included 40 patients from MIOT Hospital, Chennai, between March and December 2022. Patients with back injuries from trivial trauma were evaluated for osteoporotic VCFs using X-rays, classified according to the AO and DENNIS systems, and neurologically assessed. Pre- and post-operative (pre-op and post-operative) metrics, including the Visual Analog Scale (VAS) for back pain, Oswestry scores, anterior vertebral body height, and kyphotic angle, were documented.
Results: Most patients were female (82.5%), and 92.5% had no history of spinal surgery. Bone Mineral Density was 60% with a T-score of −2.5 and 40% with −3.5. According to Dennis’s classification, 57.5% of the patients had Type B fractures, with none having posterior compression or neurological deficits. The kyphotic angle varied by 45% at 10°. There was a significant increase in anterior vertebral body height from 24 ± 2.93 to 28 ± 2.48 (P = 0.005), decreased VAS scores (8.53 ± 0.68 pre-operative to 2.28 ± 0.91 at 6 months, P < 0.0001), and reduced Oswestry disability index (ODI) (27.98 ± 2.25 pre-operative to 12.80 ± 1.98 at 3 months, P < 0.0001). Beck’s index improved from 0.83 ± 0.05 pre-operative to 1.01 ± 0.11 post-op (P < 0.0001).
Conclusion: BKP improved pain, function, and radiological outcomes in osteoporotic vertebral fractures, with significant improvements in VAS, ODI, vertebral height, kyphotic angle, and Beck’s index, demonstrating safety and minimal complications.
Keywords: Beck index, visual analogue scale, balloon kyphoplasty, bone mineral density, osteoporotic vertebral fracture.
Vertebral compression fractures (VCFs) significantly affect healthcare, affecting 26% of women over 50 years of age and 40% over 80 years of age, with substantial quality of life and cost implications. Persistent back pain affects one-third to three-quarters of these individuals, often stemming from osteoporotic conditions such as kyphosis, kyphoscoliosis, or pseudoarthrosis. The severity of kyphosis correlates with reduced physical function, higher fracture risk, spinal cord compression, mental health problems, and impaired pulmonary function, potentially increasing the mortality rate [1]. VCFs, often due to osteoporosis, are prevalent in the elderly and cause significant pain and functional impairment. Diagnosis usually involves radiography, computed tomography, or magnetic resonance imaging. Conventional treatments include physical therapy, pain relief, and bed rest, whereas non-responders may require vertebroplasty. Family physicians can prevent these fractures by identifying high-risk individuals, addressing underlying factors, and promoting fall-prevention strategies [2]. Osteoporosis is a key risk factor for VCFs. Modifiable risks include smoking, alcohol consumption, low estrogen levels, early menopause, frailty, poor vision, lack of exercise, low body weight, and calcium and Vitamin D deficiency. Non-modifiable risk factors include advanced age, female sex, Caucasian race, dementia, fall tendency, fracture history, family fracture history, and past steroid or anticonvulsant use [3]. Dual-energy X-ray absorptiometry is the standard technique for measuring bone mineral density (BMD) and is the most accurate method for identifying osteoporosis risk. Osteopenia was defined as a T-score between −1 and −2.5, osteoporosis as a score below −2.5, and normal bone density as a score of −1 or higher [4]. Osteoporosis treatment for postmenopausal women involves 1500 mg calcium and 400 IU Vitamin D daily. Men with compression fractures should be checked for serum testosterone levels to exclude hypogonadism, and elevated alkaline phosphatase levels could suggest osteomalacia. Alcohol consumption should be moderate, smoking discouraged, and weight-bearing exercise recommended daily [5]. The treatment of painful osteoporotic fractures encompasses minimally invasive methods, such as kyphoplasty, percutaneous vertebroplasty, internal bracing, and the Osseo-Fix spinal fracture reduction system. In addition, more invasive options, such as anterior and posterior decompression and stabilisation using screws, plates, cages, and rods, exist; however, securing osteoporotic bones can be challenging [6]. Kyphoplasty, a procedure involving balloon tamp insertion into a damaged vertebral body followed by bone cement filling, can restore 50–70% of post-operative (pre-op) height and improve segmental kyphosis by 6–10°, potentially preventing pulmonary and gastrointestinal complications. Short-term results have demonstrated good to moderate pain relief in 85–100% of patients [3,7]. Kyphoplasty, Food and Drug Administration – approved since 1998, restores spinal height and corrects kyphosis by inserting a balloon tamp into the vertebral body, followed by polymethylmethacrylate cement injection [8]. The first balloon kyphoplasty (BKP) procedure created space for high-viscosity cement through inflatable bone tamps, allowing precise control and low filling pressure. Unlike vertebroplasty, BKP stabilizes fractures, corrects deformities, and mitigates vertebral compression effects [9]. The balloon restores vertebral height and creates a cavity for cement, reducing leakage. BKP usually involves a single-level bipedicular approach under imaging guidance, costing ~3,000 euros [10]. Evidence shows superior pain relief in early osteoporotic fractures compared to conservative care [11], and it is also used for hemangiomas and metastatic lesions, with outcomes influenced by fracture type, age, and positioning [12].
This study aimed to determine the functional and radiological outcomes of patients with osteoporotic vertebral fractures treated with BKP.
Materials and Methods
This prospective study included 40 patients from the Department of Orthopaedics, MIOT Hospital, Chennai, between March and December 2022. This study was approved by the Institutional Ethics Committee before initiation (IEC No. NBEMS/THESIS/2023/A-231072) dated on November 03, 2023, and informed consent was obtained from all patients.
Inclusion criteria
Patients aged >40 years with acute vertebral fracture, painful VCF refractory to conservative treatment, and fracture with >40% collapse of the vertebra were included.
Exclusion criteria
Patients with local/systemic infection, coagulation disorder, metastasis to the spine, fracture involving the posterior cortex of the vertebra/posterior ligamentous complex, vertebral fracture with neurological deficit/bowel and bladder involvement, old asymptomatic fracture, or allergy to bone cement were excluded from the study.
Patients who sustained back injuries following trivial trauma were considered. On presentation to the outpatient department, true anterior-posterior and true lateral radiographs of the injured spine were obtained to diagnose an osteoporotic VCF. Fractures were classified using the AO and DENNIS classifications. Neurological examination was performed to assess motor status, sensory status, and bowel and bladder involvement. The pre-operative Visual Analog Scale (VAS) score for backache, and Oswestry disability index (ODI) were recorded. The patients and attendees were informed about the surgical technique, post-operative (post-operative) complications, and post-operative protocols. The anterior vertebral body height was compared preoperatively and postoperatively, and the kyphotic angle was measured before and after the BKP procedure. Intraoperative and post-operative complications were also documented.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation, and categorical variables are presented as frequencies and percentages. Repeated measures analysis of variance, post hoc tests, and paired t-tests were used to analyze the data. Statistical significance was set at P < 0.05. The Statistical Package for the Social Sciences Software (v23) was used for statistical analysis.
Most patients with VCFs were aged 61–70 years 17 (42.5%) and predominantly female 33 (82.5%). Most fractures were caused by slip-and-fall incidents 35 (87.5%). In terms of occupation, 25 (62.5%) patients were sedentary workers and 15 (37.5%) were manual workers. Comorbidities such as diabetes mellitus 16 (40%) and hypertension 15 (37.5%) were frequently observed among the patients. The most common osteoporotic vertebral fracture was L1 17 (42.5%), followed by D12 13 (32.5%) (Table 1).
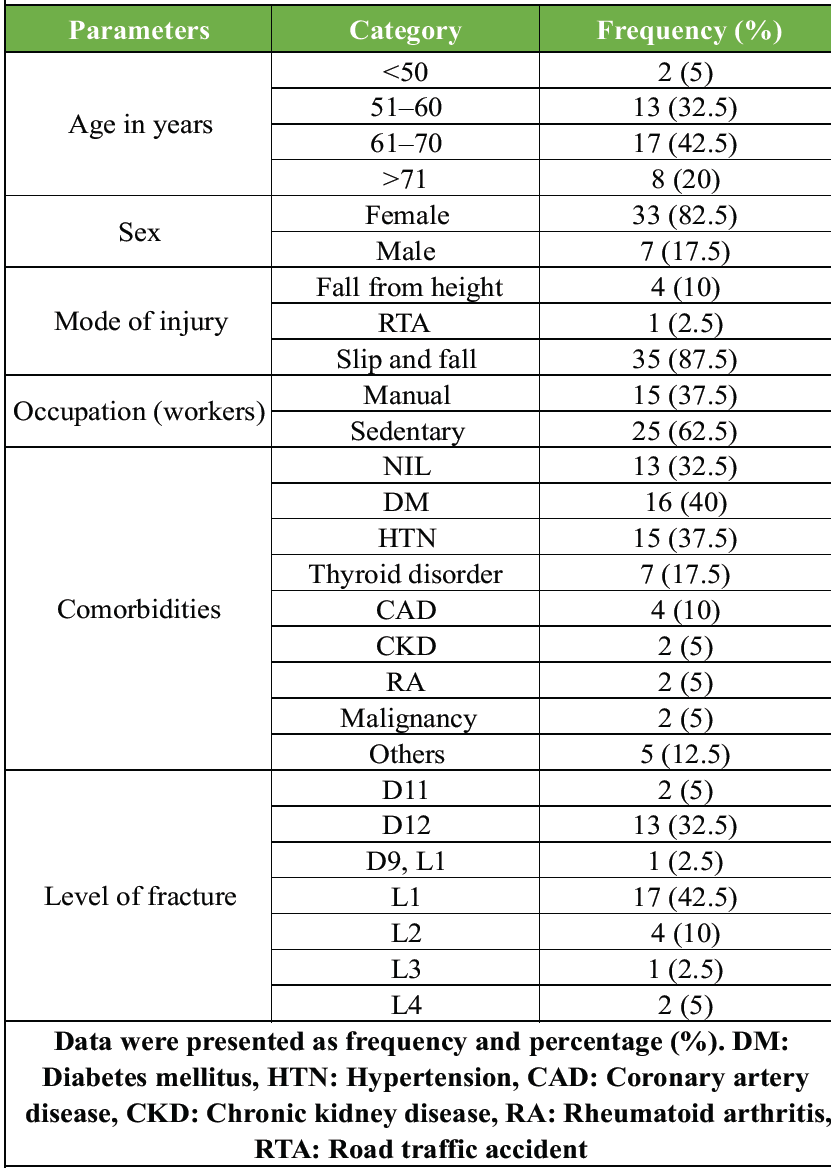
Table 1: Demographic characteristics of patients
Most patients 37 (92.5%) had no previous spinal surgery, and BMD scores indicated that 24 (60%) patients had a T-score of −2.5, and 16 (40%) had a T-score of −3.5. According to the Dennis classification, most fractures were Type B 23 (57.5%) fractures. The kyphotic angles varied, with 18 (45%) exhibiting a kyphotic angle of 10°. A 4 (10%) BKP was performed along with posterior stabilisation due to segmental instability of the spine. One (2.5%) patient had undergone kyphoplasty for osteoporotic VCFs. Single-level BKP was performed in 39 (97.5%) cases, and 1 (2.5%) patient. Extravertebral cement leakage occurred in two patients (5%), whereas the remaining 38 (95%) had no leakage. Intraoperative hypotension was also reported in 2 (5%), with 38 (95%). The kyphotic angle was reduced in most patients, with 29 (72.5%) achieving 6°, 6 (15%) achieving 7°, and 5 (12.5%) achieving 8° angles. None of the patients had posterior compression, neurological deficits, bowel involvement, or bladder involvement. General anaesthesia and an extravehicular approach were used for all procedures, and 36 (90%) patients did not require additional posterior stabilisation (Table 2).
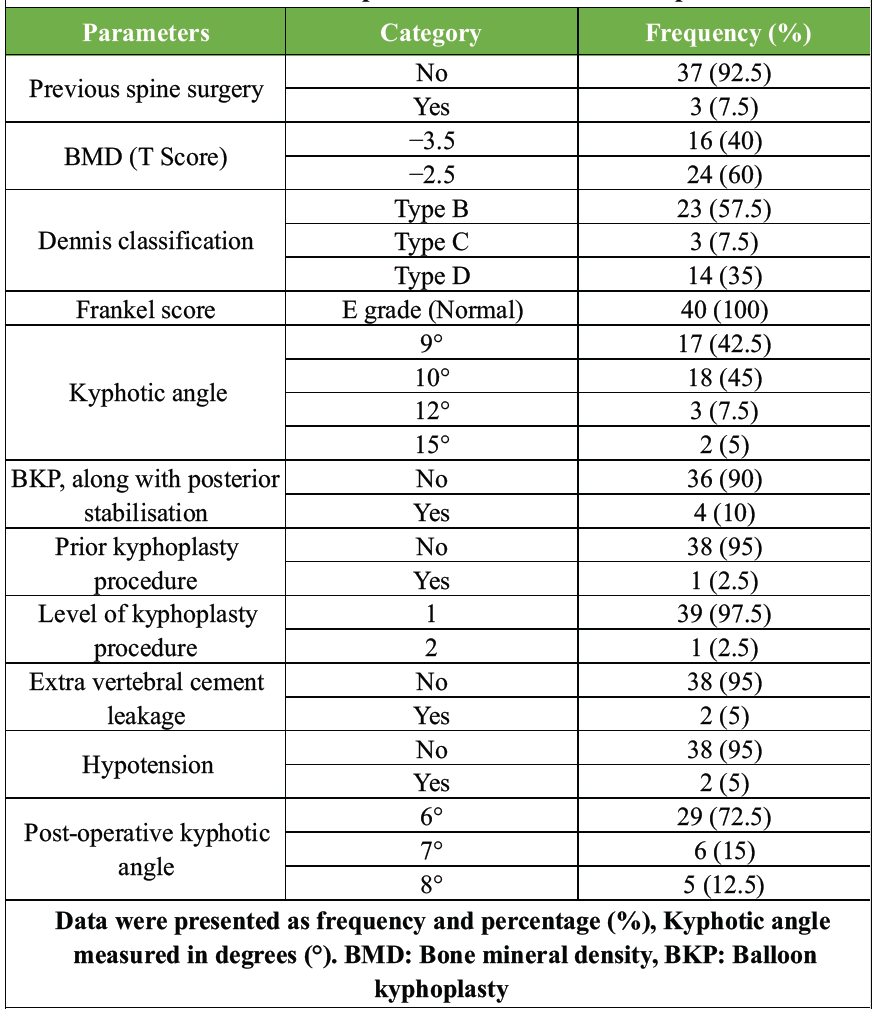
Table 2: Clinical and procedure characteristics of patients
The time interval between injury and procedure averaged 7.25 ± 14.76 weeks, and the duration of surgery was 47.25 ± 7.16 min. Significant improvements were observed in the anterior vertebral body height, which increased from 24 ± 2.93 preoperatively to 28 ± 2.48 postoperatively (P = 0.005). The VAS scores for pain showed a substantial decrease from 8.53 ± 0.68 preoperatively to 3.73 ± 0.85 immediately postoperatively, further decreasing to 2.28 ± 0.91 at 6 months (P < 0.0001). The ODI also improved significantly, reducing from 27.98 ± 2.25 pre-op to 12.80 ± 1.98 at 3 months (P < 0.0001). Beck’s index improved from 0.83 ± 0.05 preoperatively to 1.01 ± 0.11 postoperatively (P < 0.0001) (Table 3).
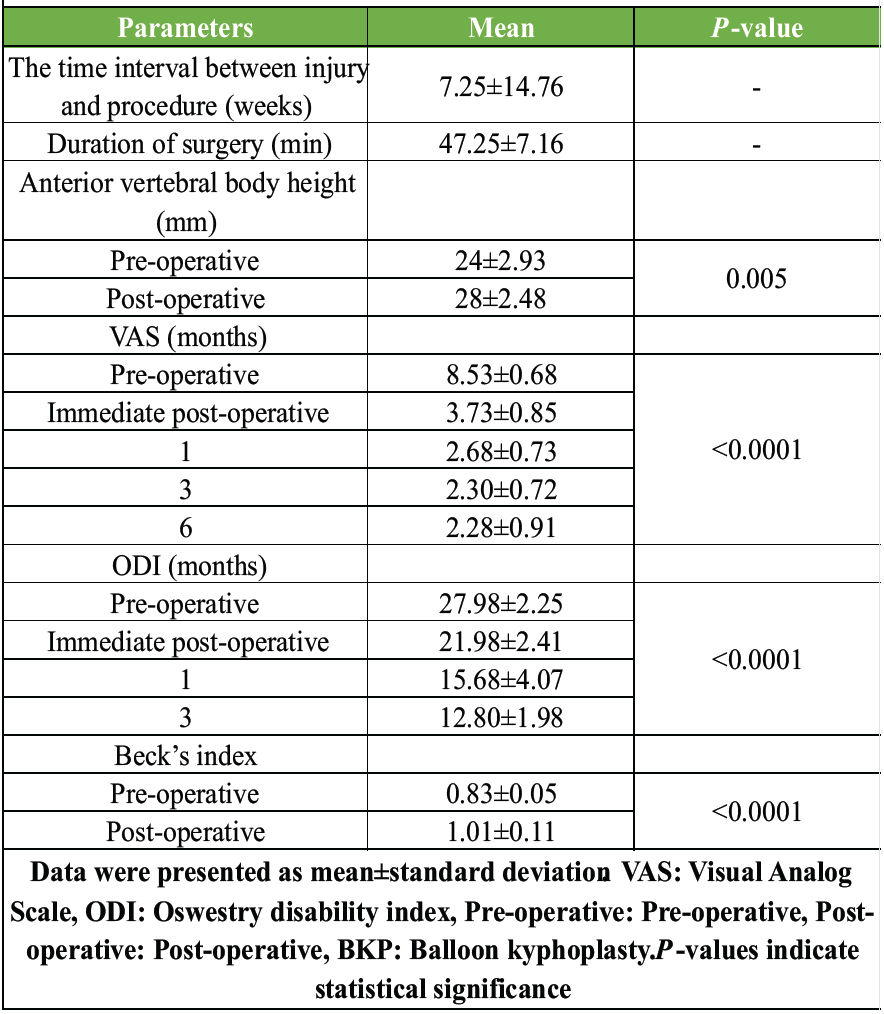
Table 3: Post-operative outcomes following BKP
In our study, most patients with VCFs were older adults, with a higher prevalence in females. The leading cause of injury was slip-and-fall, and many were sedentary workers. Diabetes mellitus and hypertension were the most common comorbidities, and fractures most frequently occurred at the thoracolumbar junction, particularly at L1 and D12. Similarly, Jose et al. reported a mean age of 63 ± 9 years, mostly between 50 and 60 years, with 70% females. Fractures are common at D12 (45%) and L1 (40%), followed by L3–L5 (5% each) [13]. Likewise, Ben Tekaya et al. studied 36 patients (mean age 65; range 41–74), including 26 females and 10 males, with 70% of fractures at the thoracolumbar junction [14]. Aligning with our findings, Ege and Akbas examined 8 patients (18 vertebrae) with a mean age of 62.5 years; 75% were female, with fractures at L3 (27%), L1 (22%), L2 (17%), L4 (17%), and L5 (17%) [15]. Overall, the findings from ours and other studies confirm that osteoporotic VCFs occur predominantly in older women, with the thoracolumbar junction, particularly L1 and D12, emerging as the most frequent fracture locations. In our study, the majority of patients had no history of prior spinal surgery, and BMD analysis confirmed osteoporosis. Most fractures were classified as Dennis Type B, with many showing mild kyphotic deformity. BKP was the primary procedure performed, usually at a single level, with only a few patients requiring additional posterior stabilisation. Complications such as cement leakage and intraoperative hypotension were rare. Postoperatively, kyphotic angle correction was commonly achieved, and no neurological deficits or bowel or bladder involvement were observed. Similarly, Deramond et al. studied 51 patients treated with BKP and reported a 4% incidence of cement leakage [16]. Similarly, Ege and Akbas noted wedge fractures as the most common (61%), followed by biconcave (33%) and crush (6%) fractures, with bone marrow edema observed in all cases. Cement leakage occurred in two patients, but without major neurological complications [15]. In line with these findings, Baz et al. observed low back pain as the main symptom, with a mean trauma-to-surgery interval of 1.1 months and a mean follow-up of 16 months. Cement leakage was observed in five patients, but no neurological deficits occurred; both VAS and ODI improved significantly after treatment [17]. Likewise, Sun et al. reported a mean operative time of 28.5 ± 8.6 min per vertebra, with 81 vertebrae treated bilaterally and 61 vertebrae treated unilaterally. Cement leakage occurred in 12 vertebrae (8.45%), mainly into the paravertebral soft tissue and discs. However, all were asymptomatic, and no major complications were noted [18]. Overall, our findings, along with evidence from other studies, indicate that BKP is a safe and effective procedure for treating osteoporotic VCFs. Single-level procedures are the most common, complications such as cement leakage or hypotension are rare, and significant pain relief and functional improvement are consistently observed without major neurological deficits. In our study, the time interval between injury and procedure was generally short, and the surgery itself required relatively little operative time. Following the intervention, there was a marked improvement in vertebral body height restoration and the radiological parameters. Pain levels were significantly reduced, with sustained relief over time, and functional recovery showed considerable improvement. Overall, the procedure demonstrated both clinical and radiological benefits. Similarly, Jose et al. reported significant improvements with VAS decreasing from 7.55 ± 0.6 pre-op to 1.95 ± 1.5 at 1 year (P < 0.005) and ODI improving from 76.6 ± 6 to 21.5 ± 16 (P < 0.001). The kyphotic angle improved from 14.3° to 6.25° postoperatively, stabilizing at 7.5°, while the anterior vertebral height increased from 52.65 ± 1.2 to 74.7 ± 0.8, maintaining stability over a year [13]. Likewise, Ben Tekaya et al. showed post-operative VAS improvement from 5.28 pre-op to 2.92 immediately, further improving to 3.42 at the last follow-up (P < 0.001). The ODI at the final follow-up was 14, with 95% of patients reporting minimal to moderate disability. The kyphotic angle improved from 16.8° to 9.5° (P < 0.001), Beck’s index increased from 0.66 to 0.8 (P < 0.05), and kyphoplasty achieved greater angular correction than vertebroplasty (8.45° vs. 5.5°, P = 0.01) [14]. Ege and Akbas found vertebral body height gains of 3.15% anteriorly, 24.6% centrally, and 0.99% posteriorly (P = 0.001), with the kyphotic angle reduced from 6.67° to 5.73° (P = 0.001). The VAS score improved from 7.8 to 2.3 at one and 6 months, while the ODI reduced from 65.2 to 20.2 at 1 month and 18.8 at 6 months (70% reduction, P < 0.05) [15]. Similarly, Baz et al. reported VAS improvement from 8.6 (VP, KP) to 1.5 and 1.0 at 12 months (P = .001), and ODI from 47.3 (VP) and 45.1 (KP) to 11.5 and 9.8 (P = 0.001), respectively. No significant difference was noted between VP and KP, indicating that both were effective [17]. In comparison, Sun et al. observed sustained benefits with VAS decreasing from 8.3 ± 1.2 to 2.9 ± 0.7, remaining at 3.0 ± 1.2 at 2 years. The ODI improved from 76.4 ± 12.5 to 26.7 ± 5.6, and was sustained at 27.8 ± 8.3, while the SF-36 scores improved. Vertebral body heights were preserved without recollapse, although five new adjacent fractures (3.5%) occurred [18]. Overall, our study and others consistently demonstrate that BKP provides significant and sustained improvements in pain, function, and radiological outcomes. Vertebral height restoration, kyphotic angle correction, and functional recovery are reliably achieved with minimal complications, and the benefits are maintained over long-term follow-up.
Limitations
The study had a small sample size, single-center design, and a short follow-up period, limiting generalisability and long-term assessment. The lack of a control group and potential subjective bias in patient-reported outcomes are additional limitations of this study.
BKP significantly improved the functional and radiological outcomes in patients with osteoporotic VCFs. The procedure effectively reduced pain, with a marked decline in VAS scores, improved functional recovery through reduced ODI scores, and enhanced radiological parameters with restoration of vertebral height, correction of kyphotic angle, and improved Beck’s index. It was safe, with only minimal complications, such as cement leakage and intraoperative hypotension. Future studies with larger samples and longer follow-ups are needed to validate these findings and assess long-term outcomes.
BKP is a safe and effective minimally invasive treatment for osteoporotic VCFs. It provides significant pain relief, improves functional outcomes, and restores vertebral height and spinal alignment, with minimal complications. Early intervention can enhance the quality of life and reduce disability in affected patients.
References
- 1. Hsieh MK, Chen LH, Chen WJ. Current concepts of percutaneous balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: Evidence-based review. Biomed J 2013;36:154. [Google Scholar] [PubMed]
- 2. Old JL, Calvert M. Vertebral compression fractures in the elderly. Am Fam Physician 2004;69:111-6. [Google Scholar] [PubMed]
- 3. Alexandru D, So W. Evaluation and management of vertebral compression fractures. Perm J 2012;16:46-51. [Google Scholar] [PubMed]
- 4. Slemenda CW, Hui SL, Longcope C, Wellman H, Johnston CC Jr. Predictors of bone mass in perimenopausal women. A prospective study of clinical data using photon absorptiometry. Ann Intern Med 1990;112:96-101. [Google Scholar] [PubMed]
- 5. Kim DH, Vaccaro AR. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J 2006;6:479-87. [Google Scholar] [PubMed]
- 6. Bostrom MP, Lane JM. Future directions. Augmentation of osteoporotic vertebral bodies. Spine (Phila Pa 1976) 1997;22:38S-42. [Google Scholar] [PubMed]
- 7. Gaitanis IN, Hadjipavlou AG, Katonis PG, Tzermiadianos MN, Pasku DS, Patwardhan AG. Balloon kyphoplasty for the treatment of pathological vertebral compressive fractures. Eur Spine J 2005;14:250-60. [Google Scholar] [PubMed]
- 8. Denaro V, Longo UG, Maffulli N, Denaro L. Vertebroplasty and kyphoplasty. Clin Cases Miner Bone Metab 2009;6:125-30. [Google Scholar] [PubMed]
- 9. Garfin SR, Yuan HA, Reiley MA. New technologies in spine: Kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine (Phila Pa 1976) 2001;26:1511-5. [Google Scholar] [PubMed]
- 10. Armsen N, Boszczyk B. Vertebro-/kyphoplasty history, development, results. Eur J Trauma 2005;31:433-41. [Google Scholar] [PubMed]
- 11. Hulme PA, Krebs J, Ferguson SJ, Berlemann U. Vertebroplasty and kyphoplasty: A systematic review of 69 clinical studies. Spine (Phila Pa 1976) 2006;31:1983-2001. [Google Scholar] [PubMed]
- 12. Bergmann M, Oberkircher L, Bliemel C, Frangen TM, Ruchholtz S, Krüger A. Early clinical outcome and complications related to balloon kyphoplasty. Orthop Rev 2012;4:e25. [Google Scholar] [PubMed]
- 13. Jose RS, Moosa MS, Bava NK. Functional and radiological outcome of percutaneous balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures – a prospective study. J Orthop Dis Traumatol 2024;7:40-6. [Google Scholar] [PubMed]
- 14. Ben Tekaya A, Hannech E, Bellil M, Ben Salah M. AB1029 clinical and radiological outcomes after vertebroplasty and kyphoplasty for osteoporotic vertebral fractures. Ann Rheum Dis 2022;81:1637-8. [Google Scholar] [PubMed]
- 15. Ege F, Akbas M. Unilateral percutaneous kyphoplasty in patients with painful osteoporotic vertebral compression fractures; Single center experience. Bozok Tıp Derg 2023;13:111-7. [Google Scholar] [PubMed]
- 16. Deramond H, Saliou G, Aveillan M, Lehmann P, Vallée JN. Respective contributions of vertebroplasty and kyphoplasty to the management of osteoporotic vertebral fractures. Joint Bone Spine 2006;73:610-3. [Google Scholar] [PubMed]
- 17. Baz AB, Akalin S, Kiliçaslan ÖF, Tokatman B, Arik H, Duygun F. Efficiency of balloon kyphoplasty in the treatment of osteoporotic vertebral compression fractures. Kobe J Med Sci 2016;62:E49-54. [Google Scholar] [PubMed]
- 18. Sun ZY, Li XF, Zhao H, Lin J, Qian ZL, Zhang ZM, et al. Percutaneous balloon kyphoplasty in treatment of painful osteoporotic occult vertebral fracture: A retrospective study of 89 cases. Med Sci Monit 2017;23:1682-90. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty
June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density
June 1, 2026 Reliability of Singh’s Index and Calcaneal Index in Assessing Osteoporosis Compared with Quantitative Ultrasound Bone Mineral Density May 1, 2026 Optimizing Post-operative Pain Management in Knee Arthroscopy: A Double-Blinded Randomized Controlled Trial of Regional Anesthesia with and without Local Infiltration
May 1, 2026 Optimizing Post-operative Pain Management in Knee Arthroscopy: A Double-Blinded Randomized Controlled Trial of Regional Anesthesia with and without Local Infiltration May 1, 2026 ‘No Dressing’ Strategy for Post-operative Orthopedic Cases
May 1, 2026 ‘No Dressing’ Strategy for Post-operative Orthopedic Cases