
In primary total knee arthroplasty for osteoarthritis, the subvastus approach enables faster early post-operative recovery, particularly quicker return of quadriceps function compared to the medial parapatellar approach, while achieving similar long-term outcomes. Preserving the extensor mechanism and pre-operative quadriceps strength play a crucial role in enhancing early rehabilitation and reducing hospital stay.
Dr. Ravindra Singh, Department of Orthopedics, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India. E-mail: mehta_85@zohomail.in
Abstract
Introduction: Knee osteoarthritis (OA) is a common cause of pain and disability in the elderly, for which total knee arthroplasty (TKA) is an effective treatment. The medial parapatellar approach is widely used but may impair patellar blood supply and delay quadriceps recovery. The subvastus (SV) approach has been introduced to preserve the extensor mechanism and potentially allow faster post-operative rehabilitation. This study compares the SV and medial parapatellar approaches in primary TKA, focusing on early recovery of quadriceps function.
Objective: This study aims to evaluate and compare the SV and medial parapatellar approaches for total knee replacement (TKR) in patients with OA at a tertiary care center, focusing on the time required for post-operative recovery of quadriceps function.
Materials and Methods: We conducted a retrospective review of medical records from 200 patients with OA who underwent TKR at a tertiary care hospital between January 2024 and December 2025. Patients were categorized into two groups: Group A underwent TKR using the SV approach, while Group B received TKR through the medial parapatellar approach. Pre-operative data, including quadriceps strength, body mass index, and baseline demographic characteristics, were collected from initial workup notes. Demographic data of all the patients were described in Table 1. Starting from the 1st post-operative day, the time to the first unassisted straight leg raise was recorded as the primary measure of quadriceps function. The collected data were then analyzed to assess post-operative quadriceps recovery.
Results: The SV approach was associated with faster recovery of quadriceps function compared to the medial parapatellar approach. Patients in their sixties experienced the most significant improvement. In addition, pre-operative quadriceps strength was found to play a key role in post-operative muscle recovery.
Conclusion: The SV approach in TKA promotes faster early recovery, including quicker quadriceps function, less pain, earlier range of motion, and shorter hospital stays compared to the medial parapatellar approach. Long-term functional outcomes are similar between the two techniques. Although technically more demanding, the SV approach is a safe and effective option that enhances early rehabilitation.
Keywords: Total knee arthroplasty, subvastus approach, medial parapatellar approach, quadriceps recovery, post-operative rehabilitation.
Knee osteoarthritis (OA) is a major public health concern and a primary cause of functional disability and reduced quality of life in the elderly [1]. OA of the hip or knee presents similarly in both men and women. Patients with advanced OA commonly experience persistent joint pain, difficulty in walking, and discomfort that worsens with weight-bearing activities. Radiographic findings often reveal joint space narrowing and osteophyte formation. Total knee arthroplasty (TKA) is an effective surgical intervention for managing severe degeneration of the knee joint [2]. Over the past 30 years, TKA has become increasingly common. The most frequently used approach for primary TKA involves an anterior midline skin incision combined with a medial parapatellar arthrotomy. In cases requiring patellar subluxation, part of the quadriceps tendon is included in the incision to gain joint access. However, incisions close to the patella can compromise its blood supply, potentially leading to anterior knee pain or even patellar fracture [3,4,5,6]. To address these issues, alternative surgical exposures have been developed to reduce patellofemoral complications and promote faster recovery of quadriceps function after surgery. Moreover, to avoid these defects, the subvastus (SV) approach and the mid-vastus approach have been introduced in TKA. In terms of subluxing the extensor mechanism laterally for knee exposure, the SV (“Southern”) technique varies from the medial parapatellar technique. The SV approach was described by Hofmann et al. in 1991 [7], and more and more surgeons have emphasized the potential benefit of this approach, as this approach keeps the extensor mechanism intact, damages less blood supply of the patella, which results in less pain in the early post-operative period, and achieves early rehabilitation [8,9]. Leave the extensor mechanism intact, according to proponents, results in faster restoration of quadriceps strength, retains greater vascularity in the patella, increases patient satisfaction while reducing post-operative pain, and. The exposure may be reduced compared to the medial parapatellar approach, especially in obese individuals and those who have had previous knee procedures. Factors, such as obesity, muscle bulk, and contractures around the knee, are also known to make the SV approach technically more difficult [10,11]. The goal of this study is to compare the SV technique to the usual medial parapatellar technique for total knee replacement (TKR) in patients with OA who present to a tertiary care center based on quadriceps function recovery in days.
This retrospective comparative study was conducted at Teerthanker Mahaveer Institute of Medical Sciences and Research Centre, where medical records of patients who underwent TKR between January 2024 and December 2025 were reviewed. Patients aged 40–80 years, of either gender, with a body mass index between 18.5 and 40 kg/m2 and diagnosed with OA requiring primary TKR were included in the study, while patients with ischemic heart disease and an ejection fraction of <30% or with incomplete records were excluded.
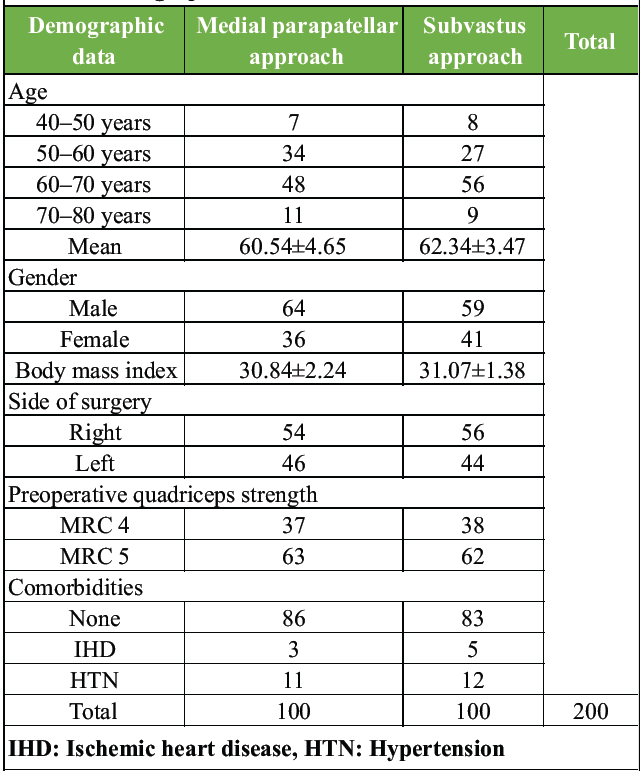
Table 1: Demographic data
After applying the eligibility criteria, a total of 200 patients were included and divided equally into two groups of 100 each based on the surgical approach used: Group A comprised patients who underwent the medial parapatellar approach, and Group B comprised patients who underwent the SV approach.
Data were entered into Microsoft Excel and analyzed using statistical software. Continuous variables were tested for normality using the Shapiro-Wilk test and expressed as mean ± standard deviation or median (interquartile range) as appropriate, while categorical variables were presented as frequencies and percentages. Group comparisons were performed using the independent t-test or Mann-Whitney U test for continuous variables and the chi-square or Fisher’s exact test for categorical variables. Multivariate linear and logistic regression analyses were conducted to adjust for confounders. A P < 0.05 was considered statistically significant. Data were anonymized, and institutional ethical approval was obtained before the study.
Surgical approaches
Group A: Medial parapatellar approach
The medial parapatellar approach is the conventional and most commonly used technique in TKA. It involves a midline skin incision and a medial arthrotomy extending into the quadriceps tendon to allow patellar eversion and wide exposure of the joint. This approach provides excellent visualization and is technically straightforward, making it suitable for most patients. However, it involves splitting the quadriceps tendon, which may lead to greater early post-operative pain and slightly delayed recovery of quadriceps function compared to muscle-sparing approaches.
Group B: SV approach
The SV (Southern) approach is a muscle-sparing technique used in TKA in which the surgeon accesses the knee joint by lifting the vastus medialis muscle without cutting the quadriceps tendon. The extensor mechanism remains intact, and the patella is displaced laterally without disrupting its blood supply. This approach aims to preserve quadriceps strength, reduce post-operative pain, and promote faster early rehabilitation. However, it can be technically more demanding, especially in obese patients or those with bulky musculature or severe deformity.
Skin incisions of both approach is shown in Fig. 1.
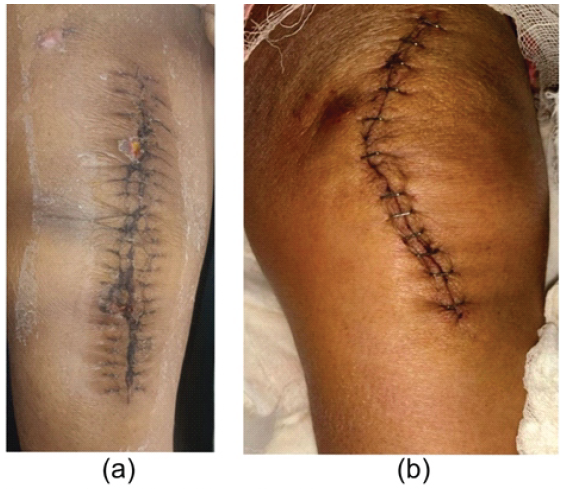
Figure 1: (a and b) The medial parapatellar approach and subvastus approach.
The outcome was assessed using a pre-specified protocol, including the duration of surgery, days to straight leg raise (SLR), post-operative pain scores, length of hospital stay, post-operative knee flexion, and post-operative knee functional outcome score.
Duration of surgery
The duration of surgery was almost the same for both groups, the medial parapatellar and SV groups.
Days to SLR
The data clearly show that patients in the SV approach had faster recovery of SLR, indicating that the surgery spared the quadriceps. Those in the SV approach recovered 0.47 days faster in SLR than patients in the medial parapatellar approach. The gender and side of TKR of the patients didn’t show any statistical significance on SLR in our analysis of the collected patient data. Mean days through both approaches are shown in Table 2.
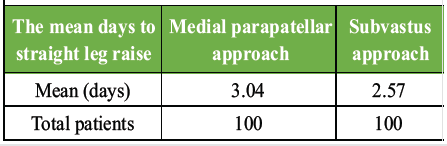
Table 2: The mean days to straight leg raise
Length of the hospital stay
In the SV approach group, patient days to SLR are less compared to the medial parapatellar approach, and ROM is achieved earlier in a satisfactory range in the subvastus group. Hence, the length of hospital stay is less in the SV group, and the post-operative infection ratio is less compared to the other group.
Post-operative knee flexion and extension
The 1st week of the post-operative period extension is more achieved, and it is less painful and more comfortable in the SV approach group as compared to the medial parapatellar approach. Knee flexion was assessed at different intervals after the operation. Accordingly, we compared the results for measurements available within 1 week and 6 weeks post-operatively. If more than one measurement was performed in the 1st week after the operation, the latest was considered for the analysis, and in the SV group, it is more than compared to the medial parapatellar approach.
Post-operative pain score
SV appeared to provide an early benefit to knee arthroplasty patients in the post-operative period, as seen by significantly reduced pain medication dosages utilized in the SV approach group during the first 48 h. SLR might be completed in substantially less time by the SV group. Patients who had the SV technique required 40% less post-operative pain medication than those who had the traditional medial parapatellar technique. Pain was also assessed at different intervals after the operation in each study. The visual analogue score is lower in the SV group (less painful) as compared to the other group (more painful).
Functional outcome score
Functional knee society score (KSS) in 200 patients at 6 and 12 weeks post-operatively. Results did not reach statistical significance.
Patients in the SV group achieved unassisted SLR significantly earlier than those in the medial parapatellar group. Early SLR is a reliable indicator of quadriceps recovery and reflects reduced surgical trauma to the extensor mechanism. Similar findings have been reported by Hofmann et al., who initially described the SV approach and highlighted its advantages in preserving quadriceps integrity and facilitating early rehabilitation [12]. Subsequent studies have also shown earlier return of quadriceps strength and improved early mobility with the SV approach [13,14,15].
Reduced pain is likely attributable to minimal quadriceps disruption and preservation of patellar vascularity. Roysam and Oakley demonstrated significantly less post-operative pain and earlier functional recovery in patients treated with the SV approach compared to the medial parapatellar approach [16]. The length of hospital stay was shorter in the SV group, correlating with earlier quadriceps recovery, faster achievement of a satisfactory range of motion (ROM), and reduced pain levels. Early mobilization is critical in preventing post-operative complications and improving patient satisfaction. Several studies have reported similar reductions in hospital stay and earlier functional milestones in patients undergoing muscle-sparing approaches in TKA [17,18,19]. With respect to post-operative knee flexion and extension, patients in the SV group demonstrated better early extension and greater flexion during the 1st post-operative week and at 6 weeks. However, by 12 weeks, functional outcome scores, including the KSS, did not differ significantly between the two groups. This suggests that while the SV approach provides advantages in early recovery, long-term functional outcomes are comparable between the two techniques. These findings are consistent with previous studies reporting early benefits without significant long-term differences [20,21]. Although the SV approach offers several advantages, it is technically more demanding and may present challenges in obese patients, individuals with bulky quadriceps, or those with fixed deformities. In the present study, operative time was comparable between both approaches, indicating that with adequate surgical experience, the SV approach does not prolong surgery. This observation is consistent with earlier reports emphasizing the role of surgical expertise in achieving optimal outcomes with the SV technique [22,23].
The SV approach in TKA offers significant advantages in the early post-operative period, including faster recovery of quadriceps function, reduced pain, earlier achievement of ROM, and shorter hospital stays compared to the medial parapatellar approach. Despite these early benefits, long-term functional outcomes, as measured by the KSS, are comparable between the two approaches. The SV technique is technically more demanding, particularly in patients with obesity or bulky musculature, but with surgical experience, it does not increase operative time. Overall, the SV approach is a safe and effective alternative to the medial parapatellar approach, promoting quicker rehabilitation without compromising long-term outcomes.
• The subvastus approach allows earlier recovery of quadriceps function compared to the medial parapatellar approach
• Post-operative pain and analgesic requirement are lower with the subvastus approach, enabling early mobilization
• Hospital stay is shorter without increasing operative time when using the subvastus approach
• Preoperative quadriceps strength influences post-operative recovery
• Early outcomes favor subvastus, while short-term functional scores are comparable between both approaches.
References
- 1. Hootman JM, Sniezek JE, Helmick CG. Women and arthritis: Burden, impact and prevention programs. J Womens Health Gend Based Med 2002;11:407-16. [Google Scholar] [PubMed]
- 2. Ethgen O, Bruyere O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg 2004;86:963-74. [Google Scholar] [PubMed]
- 3. Boerger TO, Aglietti P, Mondanelli N, Sensi L. Minisubvastus versus medial parapatellar approach in total knee arthroplasty. Clin Orthop Relat Res 2005;440:82-7. [Google Scholar] [PubMed]
- 4. Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.0.1. London: The Cochrane Collaboration; 2009. [Google Scholar] [PubMed]
- 5. Kelly MA. Patellofemoral complications following total knee arthroplasty. Instr Course Lect 2001;50:403-7. [Google Scholar] [PubMed]
- 6. Kelly MJ, Rumi MN, Kothari M, Parentis MA, Bailey KJ, Parrish WM, et al. Comparison of the vastus-splitting and median parapatellar approaches for primary total knee arthroplasty: A prospective, randomized study. J Bone Joint Surg Am 2006;88:715-20. [Google Scholar] [PubMed]
- 7. Hofmann AA, Plaster RL, Murdock LE. Subvastus (Southern) approach for primary total knee arthroplasty. Clin Orthop Relat Res. 1991;269:70-77. [Google Scholar] [PubMed]
- 8. Cila E, Guzel V, Ozalay M, Tan J, Simşek SA, Kanatli U, et al. Subvastus versus medial parapatellar approach in total knee arthroplasty. Arch Orthop Trauma Surg 2002;122:65-8. [Google Scholar] [PubMed]
- 9. Matsueda M, Gustilo RB. Subvastus and medial parapatellar approaches in total knee arthroplasty. Clin Orthop Relat Res 2000;371:161-8. [Google Scholar] [PubMed]
- 10. Cushner FD. The subvastus approach to the knee. J Knee Surg 2003;16:52-4. [Google Scholar] [PubMed]
- 11. Sporer SM. The minimally invasive subvastus approach for primary total knee arthroplasty. J Knee Surg 2006;19:58-62. [Google Scholar] [PubMed]
- 12. Hofmann AA, Plaster RL, Murdock LE. Subvastus (southern) approach for primary total knee arthroplasty. Clin Orthop Relat Res 1991;269:70-7. [Google Scholar] [PubMed]
- 13. Whiteside LA. Surgical technique for exposure of the knee using the subvastus approach. Clin Orthop Relat Res 1994;309:98-102. [Google Scholar] [PubMed]
- 14. Chang CB, Kim TK, Kang YG, Seong SC. Early quadriceps strength recovery after total knee arthroplasty using the subvastus approach. Clin Orthop Relat Res 2009;467:2832-8. [Google Scholar] [PubMed]
- 15. Engh GA, Parks NL. The subvastus approach for total knee arthroplasty. J Arthroplasty 1998;13:686-91. [Google Scholar] [PubMed]
- 16. Roysam GS, Oakley MJ. Subvastus approach for total knee arthroplasty: A prospective, randomized, and observer-blinded trial. J Arthroplasty 2001;16:454-7. [Google Scholar] [PubMed]
- 17. Varela-Egocheaga JR, Suárez-Suárez MA, Fernández-Villán M. Subvastus approach improves early recovery in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 2010;18:1034-40. [Google Scholar] [PubMed]
- 18. Meneghini RM, Pierson JL, Bagsby D, Ziemba-Davis M. Early recovery after total knee arthroplasty: Subvastus versus medial parapatellar approach. J Arthroplasty 2006;21 6 Suppl 2:43-8. [Google Scholar] [PubMed]
- 19. Peng X, Zhang X, Cheng T, Cheng M. Comparison of subvastus and medial parapatellar approaches in total knee arthroplasty: A meta-analysis. Knee Surg Sports Traumatol Arthrosc 2016;24:2565-72. [Google Scholar] [PubMed]
- 20. Dalury DF, Jiranek WA. The impact of surgical approach on early outcomes following total knee arthroplasty. Clin Orthop Relat Res 2008;466:2696-702. [Google Scholar] [PubMed]
- 21. Scuderi GR, Tenholder M, Capeci C. Surgical approaches in total knee arthroplasty. J Am Acad Orthop Surg 2006;14:20-8. [Google Scholar] [PubMed]
- 22. Engh GA, Holt BT, Parks NL. A midvastus muscle-splitting approach for total knee arthroplasty. J Arthroplasty 1997;12:322-31. [Google Scholar] [PubMed]
- 23. Dalury DF, Dennis DA. Extensile exposures in difficult total knee arthroplasty. J Am Acad Orthop Surg 2005;13:431-9. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study
June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty
June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty June 1, 2026 Short-term Clinical and Radiologic Outcomes, and Survivorship Following Primary Total Knee Arthroplasty Using a Novel High-Flexion System among Indian Patients
June 1, 2026 Short-term Clinical and Radiologic Outcomes, and Survivorship Following Primary Total Knee Arthroplasty Using a Novel High-Flexion System among Indian Patients June 1, 2026 The Prevalence of Complex Regional Pain Syndrome after Primary Total Knee Arthroplasty – A Longitudinal Study
June 1, 2026 The Prevalence of Complex Regional Pain Syndrome after Primary Total Knee Arthroplasty – A Longitudinal Study