
[box type=”bio”] What to Learn from this Article?[/box]
In case of chronic knee pain MRI should be sought out so that possibility of mucoid degeneration of ACL can be ruled out. Arthoscopic debridement is safe and effective procedure to treat it.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 87-89 | Raghvendra Choubey, Amit Jain. DOI: 10.13107/jocr.2250-0685.319.
Authors: Raghvendra Choubey[1], Amit Jain[2].
[1] Department of Orthopedics, Bundelkhand Medical College, Saugor, Madhya Pradesh, India.
[2] Department of Anesthesia, Bundelkhand Medical College, Saugor, Madhya Pradesh, India.
Address of Correspondence
Dr. Raghvendra Choubey
Department of Orthopedics & Traumatology, Bundelkhand Medical College, Sagour, Madhya Pradesh, India. Email: dr_raghvendra2006@yahoo.co.in
Abstract
Introduction: Mucoid degeneration of the anterior cruciate ligament (ACL) is a very rare cause of knee pain. Patient having mucoid degeneration of ACL seeks multiple orthopedic consultation and most of the time treating orthopedican miss its diagnosis either because of lack of experience or rare cause of pain unless doctor sought magnetic resonance imaging (MRI) of knee.
Case Report: We report a case of mucoid degeneration of the ACL in a 50-year-old female with knee pain of 18 months duration. The patient presented with extension block of the knee. After arthroscopic debridement of the lesion, the patient regained full range of motion of the knee and were pain-free at follow-up.
Conclusion: A long duration of non-specific knee pain in a patient should be evaluated with MRI. Mucoid degeneration of the ACL is suspected when an apparently thickened and ill-defined ligament with increased signal intensity on all sequences in MRI is identified in a patient with physically intact ligament and no obvious trauma history. Arthroscopic debridement of the mucoid degeneration of the ACL was safe and effective in the patient.
Keywords: Orthopedics, arthoscopy, anterior cruciate ligament.
Introduction
Mucoid degeneration of the anterior cruciate ligament (ACL) has been described in a few reports [1-6]. The lesion presents with knee pain and restriction of flexion. Here, we present a case of mucoid degeneration that was treated with arthroscopic debridement with good results.
Case Report
Clinical history
The 50-year-old female patient presented with non-specific left knee pain of 18 months duration and gradual difficulty in terminal extension. He had no previous knee injury and did not complain of giving way sensation. Examination of the knee showed loss of 15° of terminal extension without a ligamentous laxity or patella-femoral pathology. Results of both McMurray’s and apprehension’s tests were negative, and the patient was able to fully flex the knee without pain. There were no clinical signs or symptoms consistent with instability. The patient received conservative treatment for months, but the condition did not improve. Magnetic resonance imaging (MRI) of the knee was performed.
Imaging findings
Coronal proton density-weighted MRI of the right knee consists of a slice through the middle aspect of the knee which shows a thickening of the ACL (Fig. 1). The ACL shows a normal orientation with preserved fibers and homogeneously increased signal intensity. The slice demonstrates an ill-defined ACL with diffuse increased signal intensity.
Sagittal proton density-weighted MRI (Fig. 2). The slice demonstrates an ill-defined ACL with increased signal intensity and a “celery stalk” appearance of intact fibers. The girth of the ACL is increased in size. When mucoid degeneration is present, an amorphous mucoid matrix increases the signal intensity of the ACL and is focally collected between intact, almost parallel fibers. This appearance bears similarity to a stalk of celery (Celery Stalk Sign).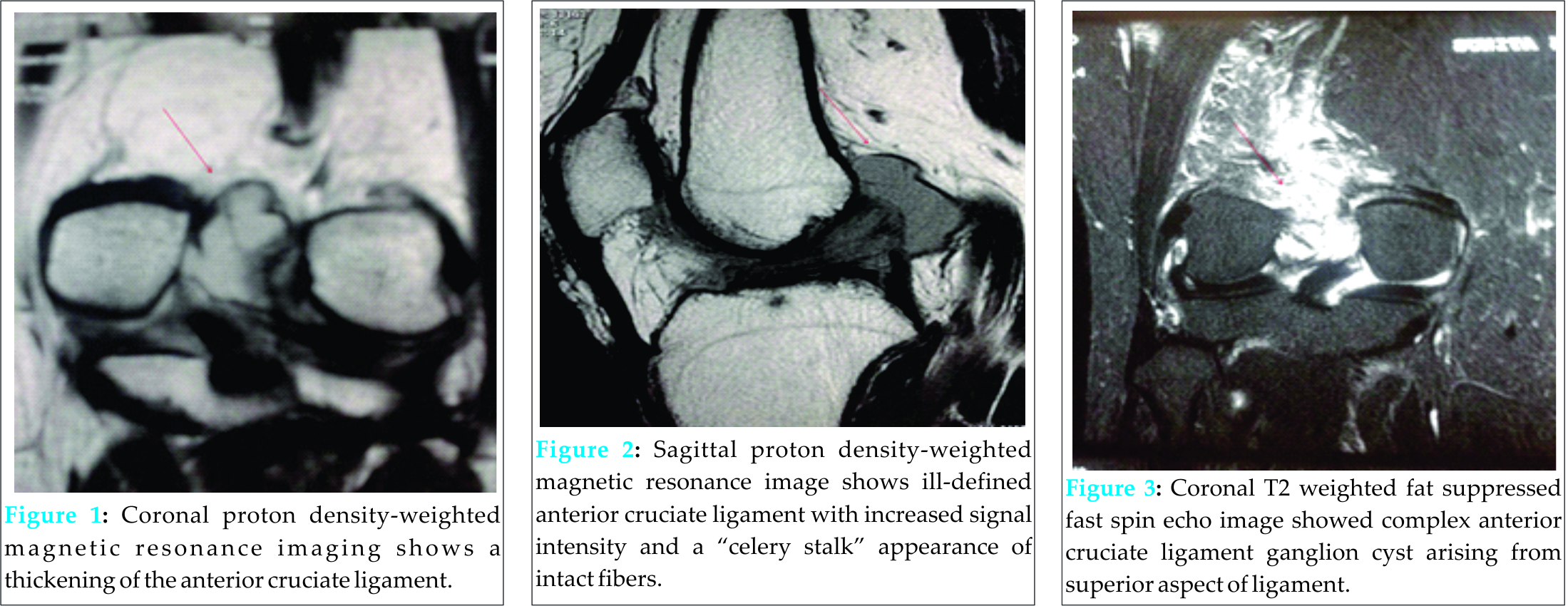
Coronal T2 weighted fat suppressed fast spin echo image (Fig. 3) showed complex ACL ganglion cyst arising from superior aspect of ligament. The ACL presented increased signal intensity. These changes were consistent with ACL ganglion cyst. Images did not show secondary signs of ACL injury.
Intraoperative findings
Under arthroscopic examination, some yellowish content in the ACL was found (Fig. 4). The yellowish content did not limit the range of motion or cause any mechanical block. This yellowish lesion of the ACL was debrided (Fig. 5). The patient had no complaint about his left knee at the 12 months follow-up.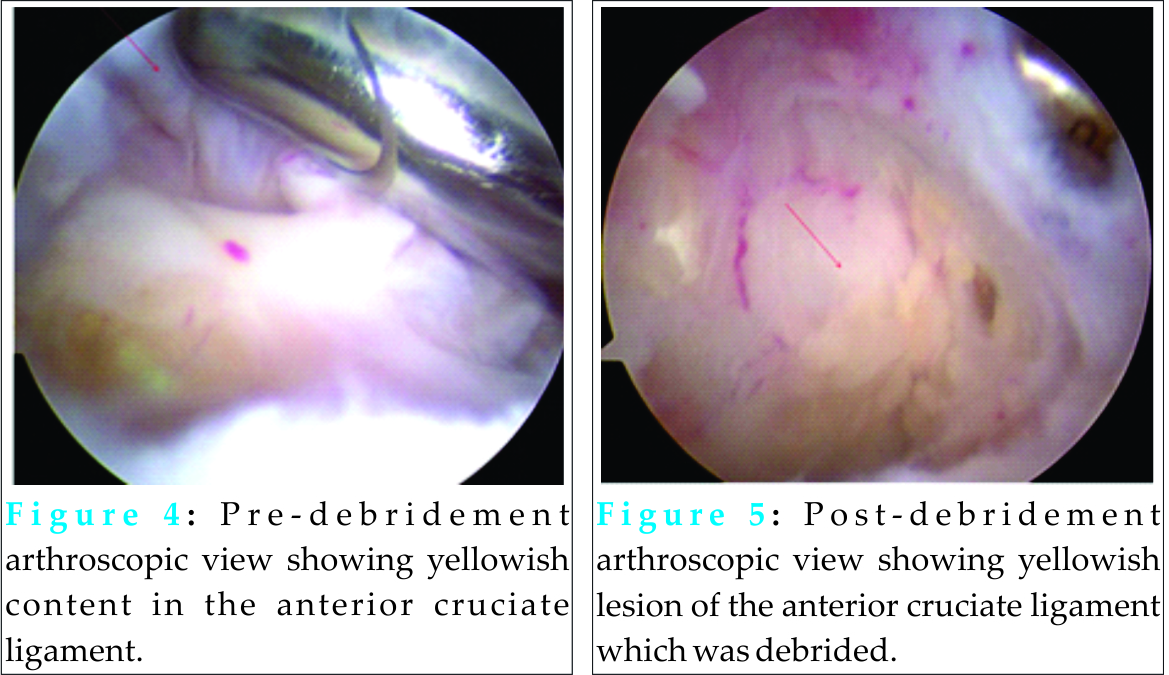
Discussion
Ganglion cyst of the ACL with intraosseous ganglia at the attachments is an unusual lesion and rarely reported [1,2,6-9,11]. ACL mucoid degeneration and ganglia, commonly coexist on MRI, both have a high association with intraosseous cysts and are typically not associated with ligament instability (secondary signs of ACL injury are usually absent) [10]. It is postulated that mucoid degeneration may be a predisposing factor to the formation of ACL ganglion cysts [1]. The pathogenesis of mucoid degeneration is unclear, but injury, ganglion cysts, and degenerative process have been implicated as the most likely etiologic factors in the production of this change. Two theories are generally accepted. One theory holds that this lesion may simply represent a continuum of senescent degeneration of the ligament (age-related degeneration). The second theory considers that congenitally or acquired synovial tissue entrapment may be the cause of cystic lesions within mucinous degeneration [3]. The patients may be symptomatic or asymptomatic. Pain is the most common complaint at presentation. The source of pain is unclear and may be either mechanical irritation due to the bulk of the ligament or a chemically mediated reaction [12]. All patients present with non-specific knee pain or pain similar to those caused by a mass or local bone erosion of which some with restriction of flexion [4]. Patients may also be unable to fully flex or extend the knee. No restriction of knee extension, no complaints of instability, no major trauma episode preceding the symptoms has been reported. It affects middle-aged patients, between 35 and 52 years old [4,11]. Clinical presentation associated with ganglion cysts of the ACL is variable in the literature. Most reported cases are incidental findings without contributory symptoms. Some case reports have described symptoms, including pain at the medial joint line, mechanical locking, clicking, and swelling, to the presence of these cysts. Knee pain was the most common symptom reported. This, however, was a non-specific symptom and was attributed to other intraarticular causes in most patients [12]. Hsu et al. reported two cases of mucoid degeneration of the ACL. The first patient presented with extension block of the knee, and the second patient had simple knee pain. Both patients did not have obvious trauma history or clinical instability of the knee. After arthroscopic debridement of the lesion, both patients regained full range of motion of the knee and were pain-free at follow-up.
The MR-findings of mucoid degeneration of the ACL include: An ill-defined ACL, an increased ligamentous girth, a normal orientation of the ligament and an increased signal intensity on all sequences interspersed among visible intact ACL fibers (“celery stalk” appearance) [8]. Criteria for mucoid degeneration includes ligament bundles poorly seen on T1 weighted but with both bundles intact on T2 or PD weighted images. The lesion may manifest as an elongated cyst along the long axis of the ACL, or as an enlarged ACL. This appearance can mimic acute or chronic interstitial partial tears of the ligament [1]. Discrete intraosseous ganglia at the femoral and tibial attachments are observed in 77% of the cases with mucoid degeneration of the ACL. These ganglia consist of myxoid material and have generally no identifiable communication with the articular surface or joint cavity [3]. Mucinous degeneration of the ACL was described as a potential pitfall for the diagnosis of a ligament tear [1]. Long with tears and ACL ganglion cysts, mucoid degeneration is a relatively common cause of increased signal within the ACL [1]. The absence of clinical signs and symptoms consistent with instability also helps to avoid misdiagnosis [12]. Hodler et al., correlating between MRI appearance and histology findings in cadaveric specimens, found focal areas of signal increase in 29 of 38 ligaments. In 17 of these 29 ligaments, mucoid and/or eosinophilic degeneration was found, which appeared to have caused the focal MRI signal change [4].
Arthroscopic surgery is an optional therapy and implies partial excision of the sclerotic lesions of the ACL resulting in immediate pain relief and improvement of the range of motion without any symptoms of instability. The significant pain relief is being attributed to the decreased volume and tension in the ACL..
Conclusion
Arthroscopic debridement of the mucoid degeneration of the ACL is safe and effective according to literature reports and my experience. Mucoid degeneration of the ACL should be considered when an apparently thickened and ill-defined ACL with increased signal intensity on all sequences is identified in a patient with a clinically intact ACL..
Clinical Message
A long duration of non-specific knee pain in a patient should be evaluated with MRI especially with clinically intact ligament and no obvious trauma history. Mucoid degeneration of the ACL is a very rare cause of knee pain. Patient having mucoid degeneration of ACL seeks multiple orthopedic consultation and most of the time treating orthopedician miss its diagnosis either because of lack of experience or rare cause of pain unless doctor sought MRI of knee. Arthroscopic debridement of the mucoid degeneration of the ACL was safe and effective in the patient..
Reference
1. Bergin D, Morrison WB, Carrino JA, Nallamshetty SN, Bartolozzi AR. Anterior cruciate ligament ganglia and mucoid degeneration: Coexistence and clinical correlation. AJR Am J Roentgenol 2004;182(5):1283-7.
2. Fealy S, Kenter K, Dines JS, Warren RF. Mucoid degeneration of the anterior cruciate ligament. Arthroscopy 2001;17(9):E37.
3. Hensen JJ, Coerkamp EG, Bloem JL, De Schepper AM. Mucoid degeneration of the anterior cruciate ligament. JBR-BTR 2007;90(3):192-3.
4. Hodler J, Haghighi P, Trudell D, Resnick D. The cruciate ligaments of the knee: Correlation between MR appearance and gross and histologic findings in cadaveric specimens. AJR Am J Roentgenol 1992;159(2):357-60.
5. Hsu CJ, Wang SC, Fong YC, Huang CY, Chiang IP, Hsu HC. Mucoid degeneration of the anterior cruciate ligament. J Chin Med Assoc 2006;69(9):449-52.
6. Kumar A, Bickerstaff DR, Grimwood JS, Suvarna SK. Mucoid cystic degeneration of the cruciate ligament. J Bone Joint Surg Br 1999;81(2):304-5.
7. Lancaster TF, Kirby AB, Beall DP, Wolff JD, Wu DH. Mucoid degeneration of the anterior cruciate ligament: A case report. J Okla State Med Assoc 2004;97(8):326-8.
8. McIntyre J, Moelleken S, Tirman P. Mucoid degeneration of the anterior cruciate ligament mistaken for ligamentous tears. Skeletal Radiol 2001;30(6):312-5.
9. Melloni P, Valls R, Yuguero M, Sáez A. Mucoid degeneration of the anterior cruciate ligament with erosion of the lateral femoral condyle. Skeletal Radiol 2004;33(6):359-62.
10. Narvekar A, Gajjar S. Mucoid degeneration of the anterior cruciate ligament. Arthroscopy 2004;20(2):141-6.
11. Nishimori M, Sumen Y, Sakaridani K. Mucoid degeneration of the anterior cruciate ligament – A report of two cases. Magn Reson Imaging 2004;22(9):1325-8.
12. Papadopoulou P. The celery stalk sign. Radiology 2007;245(3):916-7.
| How to Cite This Article: Amit P, Maharajan K, Varma B. Streptococcus pyogenes Associated Post-traumatic Brodie’s Abscess of Cuboid: A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3):87-89 . Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-319-fultext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Superior Gluteal Artery Perforation Following Girdlestone Resection Arthroplasty: A Case Report
December 1, 2025 Superior Gluteal Artery Perforation Following Girdlestone Resection Arthroplasty: A Case Report August 1, 2025 The Novel Use of a Custom Three-Dimensional-Printed Polycaprolactone-Tricalcium Phosphate Synthetic Bone Scaffold (Osteopore®) in the Management of a Critical-Sized Bone Defect for a Patient with an Open Intra-Articular Calcaneal Fracture – A Case Report
August 1, 2025 The Novel Use of a Custom Three-Dimensional-Printed Polycaprolactone-Tricalcium Phosphate Synthetic Bone Scaffold (Osteopore®) in the Management of a Critical-Sized Bone Defect for a Patient with an Open Intra-Articular Calcaneal Fracture – A Case Report April 1, 2025 Are Systematic Reviews and Meta-analysis on the Verge of Extinction with the Advent of Artificial intelligence?
April 1, 2025 Are Systematic Reviews and Meta-analysis on the Verge of Extinction with the Advent of Artificial intelligence? April 1, 2025 Team Work in Orthopedics – The Winning Formula
April 1, 2025 Team Work in Orthopedics – The Winning Formula