
Repurposing degloved skin as a primary full-thickness autograft provides a highly effective strategy that facilitates early definitive wound coverage and functional recovery, which significantly reduces the surgical and economic burden in an extensive lower limb traumatic injury.
Dr. Rishabh Guliani, Department of Orthopaedics, Dayanand Medical College and Hospital, Ludhiana, Punjab, India. E-mail: dr.rishabhguliani@gmail.com
Abstract
Introduction: Degloving injuries involve the traumatic separation of skin or underlying tissues from their respective bone structures, typically resulting from high-energy mechanisms such as road traffic accidents. The hallmark of these lesions is the avulsion of septal and muscular perforators, which devascularizes the skin envelope and may lead to delayed full-thickness necrosis or limb loss if mismanaged. Historically, these injuries require staged procedures to replace the skin; however, this case report highlights the role of primary full-thickness skin grafting (FTSG) using repurposed tissue performed during the primary debridement. By carefully defatting and converting degloved skin into a graft, surgeons can provide a viable pathway for early definitive coverage.
Case Report: A 64-year-old male presented following high-energy mechanisms, such as a road traffic accident, with a Tscherne Grade III extensive degloving injury of the right lower limb, measuring 35 × 15 cm and involving 60–70% of the limb circumference. Following stabilization with an across-knee external fixator and radical surgical debridement, a Morel–Lavallee lesion was identified. Skin regions with clinically doubtful vascularity were excised, defatted, and repurposed as a primary full-thickness autologous graft. Although a marginal necrosis involving 20–30% of the graft required a split-thickness skin graft, the final functional and esthetic outcomes were excellent with a reduction in pain over time. Progressive epithelialization was observed during follow-up, with complete epithelial cover achieved by the 3-month visit.
Conclusion: Repurposing avulsed tissue into a primary FTSG provides a practical alternative to the conventional multistage reconstruction. This approach provides early wound stabilization while minimizing the need for repeated surgeries.
Keywords: Avulsed skin, degloving injury, full-thickness skin graft, Morel–Lavallée lesion, lower limb injury, split-thickness skin graft, autologous skin graft, limb salvage.
Degloving injuries occur when the skin or underlying tissues are separated from the respective bone structures. These are usually a result of high-energy mechanisms such as traumatic road accidents, wringer injuries, or industrial roller accidents. The lower and upper extremities are among the most common sites [1,2]. Depending on the duration and intensity of each of the offending forces, the resulting injury can consist of an open abraded wound of variable depth and surface [3], an area of undermining of soft tissue envelope which can affect part or the full circumference of the limb in single or multiple planes [4]. The hallmark of this type of lesion is avulsion of the septal and muscular perforators, which further devascularises an important part of the skin envelope. Mismanagement of such injuries can result in delayed full-thickness necrosis of the avulsed skin flap and even loss of the limb or systemic life-threatening complications [5]. Historically, these injuries require extensive irrigation followed by debridement and a staged procedure to replace “like with like” skin. To achieve these results, autologous skin grafts have always been the main treatment for wound reconstruction. These are categorized into split-thickness skin grafts (STGs), full-thickness skin grafts (FTSGs), and epidermal grafts based solely on the composition of the skin [6,7]. Among these, FTSG can be used to help close a variety of wounds. These grafts are relatively simple to perform and provide for a rapid primary closure of full-thickness wounds that might otherwise take a prolonged period to heal. The objective of this case report is to highlight the role of primary FTSG performed during index debridement. By repurposing the degloved skin, carefully defatting and converting it into a graft, we demonstrate a viable pathway for early definitive coverage. This approach effectively bypasses the need for multiple staged procedures, thereby reducing significant economic burden and long clinical wait times typically seen in extensive lower limb trauma.
A 64-year-old male presented to the emergency department on September 11th, 2025, following a high-energy road traffic accident involving a collision between a two-wheeler and a four-wheeler. On arrival, the patient was resuscitated and hemodynamically optimized as per standard trauma protocols. He was conscious and cooperative with a Glasgow Coma Scale score of 15/15. Initial vital parameters included a blood pressure of 130/80 mm Hg and a heart rate of 96 beats/min. Further local examination revealed an extensive degloving injury of the right lower limb involving the proximal leg, knee, and distal thigh. The wound was measured approximately 35 × 15 cm and involved 60–70% of the limb circumference (Fig. 1).

Figure 1: Right lower limb demonstrating a circumferential degloving injury measuring 35 × 15 cm and involving 60–70% of limb circumference (September 11th).
The wound was also grossly contaminated with road debris. There was pain and a restricted range of motion over the affected knee. The distal limb vascularity was clinically preserved with palpable dorsalis pedis and posterior tibial pulses, a warm limb, and, on recording, a capillary refill time of <2 s was seen. Neurological examination also revealed intact motor and sensory function distal to the injury. Based on the severity of soft-tissue injury, the lesion was classified as Tscherne Grade III. The mangled extremity severity score was recorded as 6, and given preserved distal perfusion, absence of prolonged ischemia, and an overall physiological stability, a multidisciplinary decision was made to proceed with limb salvage rather than primary amputation. The patient was taken to the operating theatre on the day of presentation. The associated injuries were also identified during the initial assessment, which included an open fracture of the proximal phalanx of the right first and third toes. To manage the complexity of a suspected multi-ligamentous injury and extensive degloving, we prioritized immediate limb stabilization with an across-knee external fixator. This approach served a dual purpose: It neutralized mechanical shear forces that could further compromise the fragile periarticular soft tissue, while providing a stable environment for essential wound care and monitoring, as shown in X-ray (Fig. 2).
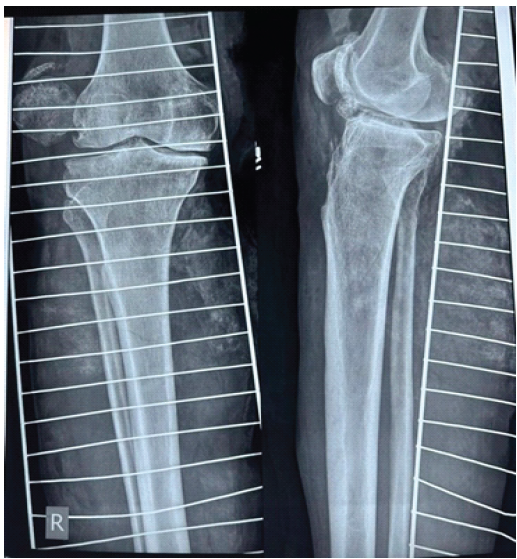
Figure 2: Anteroposterior and lateral X-ray of the right knee demonstrating an across-knee external fixator (September 11th). Confirms limb stabilization to limit shear forces and enable definitive soft-tissue management.
The procedure began with an extensive surgical debridement of all devitalized soft tissue, complemented by copious wound irrigation. Intraoperatively, we identified a profound circumferential skin degloving consistent with a massive Morel–Lavallee lesion that spanned the distal thigh, knee, and proximal leg. During this exploration, regions of skin in both the proximal and distal margins exhibiting clinically doubtful vascularity were excised alongside the underlying devitalized subcutaneous fat. Rather than discarding this tissue, we meticulously defatted the excised skin and repurposed it as a primary full-thickness autologous graft. Prepared to a thickness of approximately 0.8–1 mm, the graft was then meshed at a 1.5:1 ratio to ensure adequate fluid drainage and applied over the defect, with definitive fixation achieved using surgical staples (Fig. 3).

Figure 3: Application of a primary full-thickness autologous skin graft after defatting and meshing (1.5:1), thickness 0.8–1 mm (September 11th). Shows an immediate, definitive coverage strategy after primary debridement.
The time required for the preparation of this graft did not significantly exceed that of routine debridement, and no tourniquet was used during the procedure. A wound coverage of 60–70% was achieved using the harvested skin graft, while the open fractures of the right first and third toes were debrided and subsequently stabilized using two 1.5-mm K-wires. During the inpatient stay from September 12 to 25, 2025, the patient was managed with regular dressing changes using sterile paraffin gauze, targeted bedside debridements and the administration of broad-spectrum intravenous antibiotics (Fig. 4).

Figure 4: The right lower limb during the inpatient ward stay (September 12–25, 2025). The across-knee external fixator remains in situ for continued stabilization. Demonstrates early graft adherence, developing granulation tissue, and identifies marginal areas at risk of devitalization.
Postoperatively, the patient was mobilized from post-operative day 2 using a walker with partial weight bearing, which gradually progressed to full weight bearing with walker support as wound healing allowed. Early post-operative dressings performed within the first 3–5 days demonstrated healthy granulation tissue with 60–70% graft uptake. As anticipated, some patchy areas of graft devitalization were noted at the wound margins, particularly in regions corresponding to the original zones of compromised skin vascularity (Fig. 5).

Figure 5: Progress of graft integration between post-operative days 5 and 10, showing 70% uptake of the meshed autograft and patchy marginal necrosis. Defines the extent of non-viable graft requiring local debridement and guides the need for secondary coverage.
Between post-operative days 5 and 10, superficial graft necrosis involving 20–30% of the grafted surface area became evident. We managed these areas with local debridement during changes while preserving well-adhered grafted areas. Inflammatory markers were monitored serially to track clinical progress. Initial post-operative laboratory evaluation showed a C-reactive protein (CRP) level of approximately 168 mg/L and a total leukocyte count of 15.2 × 109/L, which progressively decreased to a CRP of approximately 22 mg/L and a total leukocyte count of 8.9 × 109/L. The patient was discharged on September 25th, 2025, with instructions for home-based wound care and schedule outpatient follow-up. At discharge, the wound showed robust granulation tissue with 70–75% viable graft intake. He was subsequently readmitted on October 4th, 2025, for definitive coverage of the residual wound areas using an STSG harvested from the contralateral thigh (Fig. 6).

Figure 6: Post-operative view following split-thickness skin grafting. The graft is secured with surgical staples, achieving definitive wound closure where the primary graft did not integrate (October 04, 2025).
At this time, an examination under anesthesia confirmed the absence of any multi-ligamentous knee instability, allowing for the safe removal of the external fixator. Overall operative efficiency was maintained as the extent of skin salvaged during the primary procedure reduced the requirement for the extensive graft harvest in subsequent procedures, thereby shortening operative time in later stages. Following a 1-week post-operative observation period, both the primary FTSG and the secondary STSG demonstrated satisfactory integration, and the patient was cleared to begin physiotherapy. At the 3-month follow-up (January 2026), clinical examination showed a well-healed soft-tissue envelope with stable scarring, excellent graft uptake, and no residual ulceration (Fig. 7 and 8). The patient demonstrated improving pain control over time and expressed satisfaction with the functional recovery and final appearance of the limb.

Figure 7 & 8: Clinical assessment at 3 months showing well-healed skin graft with robust soft-tissue coverage across the distal thigh, knee, and proximal leg. There is complete graft integration, stable scarring, and no evidence of residual ulceration, demonstrating good healing following degloving injury and readiness for functional rehabilitation.
The management of extensive lower limb degloving injuries remains a big challenge in reconstructive surgery, primarily because the clinical appearance of the skin in the emergency department is often a poor predictor of its ultimate viability. As Kyriakidis et al. observed, the shearing forces involved in these high-energy traumas disrupt the musculocutaneous perforators, leading to a delayed necrosis that can typically manifest days after the initial surgery [8]. In our patient’s case, a critical surgical decision was made during the initial debridement to move beyond simple irrigation and passive observation. We identified adjacent skin areas where the vascularity appeared marginal or at high risk of impending necrosis. Rather than adopting a traditional “wait-and-see approach,” often involving prolonged negative pressure wound therapy and eventual STSG, our case suggests that immediate reconstruction using the avulsed tissue as a primary FTSG may offer an efficient path to recovery. This approach aligns with the findings of Yan et al., who reviewed 129 cases of lower limb degloving and concluded that immediate FTSG following radical debridement is not only feasible but superior in achieving limb salvage [9]. Our decision to repurpose the avulsed skin aligns with the principles described by Gazes et al., who advocate for the use of autologous FTSG from tissue “destined to be discarded” to diminish donor site morbidity and lower risk of rejection [10]. Albu et al. have noted that while there is surprisingly little literature supporting the use of large primary FTSGs, the biological benefit of replacing the skin in its entirety remains a logical and effective strategy [11]. Furthermore, our approach offers a cost-effective alternative to more recent technological advancements in wound care. While dermal regeneration templates (e.g., Integra) and autologous homologous skin constructs have shown success in complex trauma [12,13], they frequently necessitate a two-staged surgical process, extended hospitalization, and substantial material costs that can be prohibitive in many clinical settings. We achieved immediate wound coverage and avoided the need for an early staged reconstructive pathway. The post-operative CRP trend, which fell from 168 mg/L to 22 mg/L over 2 weeks, was consistent with an uncomplicated post-operative recovery pattern. The interpretation is in keeping with the systematic review by Kruidenier et al., which showed that CRP kinetics after trauma surgery are most useful when read as part of the overall clinical picture, with an early peak followed by a steady decline supporting satisfactory recovery in the absence of deep infection or ongoing tissue injury [14]. It is important to acknowledge the risks of primary grafting in a contaminated trauma setting. In our patient, while 70–75% of the graft integrated successfully, 20–30% of the margins underwent superficial necrosis, which required debridement and contralateral STGs for definitive closure. The patient began assisted ambulation with a walker from post-operative day 2, with partial weight bearing progressing to full weight bearing. The patient reported a gradual reduction in pain and was satisfied with the functional and cosmetic outcome. Although knee range of motion is routinely assessed as a part of functional outcome evaluation, formal assessment was not performed in this case while the spanning external fixator remained in situ, which limits reliable joint examination. Functional assessment was therefore based on wound healing, ambulation status, pain progression, and patient satisfaction during follow-up. Nevertheless, the initial FTSG provided early, durable coverage of the defect and supported subsequent rehabilitation. This aligns with existing reports suggesting that some degree of secondary grafting is often required when using traumatized skin [8]. This case proves that even when skin vascularity is clinically doubtful, primary conversion to a full-thickness graft can significantly reduce the total number of interventions, shorten hospital stay, and yield functional and esthetic results compared to traditional staged grafting techniques.
This case shows that harvesting avulsed tissue and reapplying it as a primary full-thickness graft during the index procedure helps earlier recovery and prevents prolonged hospitalization. Even though the graft margins experienced superficial necrosis, requiring local debridement and a supplemental STSG, the final functional and esthetic results were excellent. Ultimately, viewing tissue as a surgical resource rather than waste helps reduce both the physiological stress on the patient and the overall cost of their care.
Extensive degloving injuries typically prompt a wait-and-see approach involving prolonged wound therapy and staged reconstructions. This case demonstrates that the immediate conversion of avulsed tissue into a primary full-thickness autograft is a highly effective clinical strategy for achieving early definitive coverage. By performing radical index debridement, defatting avulsed skin, and using it as a graft, surgeons can significantly decrease the recovery time and can get excellent functional results.
References
- 1. Khan AT, Tahmeedullah, Obaidullah. Degloving injuries of the lower limb. J Coll Physicians Surg Pak 2004;14:416-8. [Google Scholar] [PubMed]
- 2. Lim SM, Lee ST. The pattern and management of traumatic soft tissue injuries of the lower limb. Ann Acad Med Singap 1982;11:145-53. [Google Scholar] [PubMed]
- 3. Hudson DA, Knottenbelt JD, Krige JE. Closed degloving injuries: Results following conservative surgery. Plast Reconstr Surg 1992;89:853-5. [Google Scholar] [PubMed]
- 4. Arnez ZM, Khan U, Tyler MP. Classification of soft-tissue degloving in limb trauma. J Plast Reconstr Aesthet Surg 2010;63:1865-9. [Google Scholar] [PubMed]
- 5. Mandel MA. The management of lower extremity degloving injuries. Ann Plast Surg 1981;6:1-5. [Google Scholar] [PubMed]
- 6. Kanapathy M, Smith OJ, Hachach-Haram N, Bystrzonowski N, Mosahebi A, Richards T. Protocol for a systematic review of the efficacy of epidermal grafting for wound healing. Syst Rev 2016;5:92. [Google Scholar] [PubMed]
- 7. Andreassi A, Bilenchi R, Biagioli M, D’Aniello C. Classification and pathophysiology of skin grafts. Clin Dermatol 2005;23:332-7. [Google Scholar] [PubMed]
- 8. Kyriakidis A, Katsaros I, Vafias E, Agorgianitis L, Kyriakidis V, Zacharopoulos A. Degloving injury of the lower extremity: Report of two cases. Acta Med Acad 2019;48:303-6. [Google Scholar] [PubMed]
- 9. Yan H, Gao W, Li Z, Wang C, Liu S, Zhang F, et al. The management of degloving injury of lower extremities: Technical refinement and classification. J Trauma Acute Care Surg 2013;74:604-10. [Google Scholar] [PubMed]
- 10. Gazes MI, Au AS, Jariwala T, Vyce SD. Degloving traumatic lesser toe injury reconstruction with full-thickness skin graft from partially amputated autologous toe donor site: A case report. J Am Podiatr Med Assoc 2022;112:20-14. [Google Scholar] [PubMed]
- 11. Albu E, Alexandru A, Marinescu B, Ene R, Cârstoiu C. Combining tangential hydrodissection, panniculectomy, and negative pressure wound therapy in treating extensive degloving injury of the leg. J Med Life 2014;7:123-6. [Google Scholar] [PubMed]
- 12. Attia A, Elmenoufy T, Atta T, Harfoush A, Tarek S. Combination of negative pressure wound therapy (NPWT) and Integra dermal regeneration template (IDRT) in the lower extremity wound; Our experience with 4 cases. JPRAS Open 2020;24:32-9. [Google Scholar] [PubMed]
- 13. Khavanin N, Soltanian HT. Successful use of an autologous homologous skin construct for the management of acute surgical and traumatic wounds: A clinical experience in two patients. Wounds 2022;34:E74-7. [Google Scholar] [PubMed]
- 14. Kruidenier J, Dingemans SA, Van Dieren S, De Jong VM, Goslings JC, Schepers T. C-reactive protein kinetics and its predictive value in orthopedic (trauma) surgery: A systematic review. Acta Orthop Belg 2018;84:397-406</p> [Google Scholar] [PubMed]
- 15. <p> [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature
July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series
July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series July 1, 2026 Short-term Functional Outcomes of Shoulder Girdle Limb Salvage in Primary Bone Tumors: A 2-year Follow-up Study
July 1, 2026 Short-term Functional Outcomes of Shoulder Girdle Limb Salvage in Primary Bone Tumors: A 2-year Follow-up Study June 1, 2026 Limb Salvage in a Mangled Foot with Severe Midfoot Bone Loss: A Case Report and Review of Principles of Reconstruction
June 1, 2026 Limb Salvage in a Mangled Foot with Severe Midfoot Bone Loss: A Case Report and Review of Principles of Reconstruction