
Western Indian thoracolumbar junction (T11–L2) pedicles measure 5.14–6.39 mm width (narrower than Western norms), supporting 4.5–6.5 mm converging screws (40–50 mm length) for safe fixation, with all parameters increasing caudally and significant sex differences.
Dr. Kishore Parihar, Department of Orthopedics, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India. E-mail: drkishoreparihar@gmail.com
Abstract
Introduction: Morphometric data for safe transpedicular screw placement at the thoracolumbar junction (T11–L2) remain limited for Indian populations, despite ethnic variations affecting screw sizing and complications. This study provides prospective computed tomography-based reference values for Western India.
Materials and Methods: Prospective analysis of 200 consecutive adults (≥20 years; 110 males, 90 females) with back pain but normal thoracolumbar imaging (June 2021–August 2023) at a Western Indian tertiary center was conducted. Ethical approval taken from Institutional Ethics Committee, AIIMS Jodhpur (IEC No.- AIIMS/IEC/2022/4070). The bilateral pedicle width, interpedicular distance (IPD), anterior cortex depth, and transpedicular angle measured at T11–L2 using digital imaging and communications in medicine viewer (1–2 mm slices). Means ± standard deviation were compared by sex using unpaired t-tests (P < 0.05 significant; Excel).
Results: Pedicle width increased caudally (T11: 5.14 ± 0.87 mm; L2: 6.39 ± 0.89 mm), with male > female at T12/L1 (P < 0.01). IPD rose from T11 (1.74 ± 0.20 cm) to L2 (2.15 ± 0.20 cm; L1 P = 0.039 by sex). Transpedicular angle: T11 (19.96 ± 2.20°) to L2 (23.06 ± 1.42°; all P < 0.05 by sex). Anterior cortex depth peaked at L1 (5.05 ± 0.86 cm). Safe screws: Thoracic 4.5–5.5 mm, lumbar 5.5–6.5 mm.
Conclusion: Western Indian norms show narrower pedicles than Western data, aligning with other Indian series but adding a T11–L2 focus. This aids in ethnicity-specific screw selection to reduce misplacement in thoracolumbar fixation.
Keywords: Thoracolumbar junction, pedicle morphometry, transpedicular screw, computed tomography, Indian population.
The thoracolumbar junction (T11–L2) marks the transition from rigid thoracic kyphosis to flexible lumbar lordosis, rendering it biomechanically vulnerable to fractures and instability that require fixation [1,2]. The unique anatomy, combining the end of the spinal cord and beginning of the cauda equina, makes this region particularly susceptible to injury from traumatic insults, with a subsequent need for surgical stabilization [3].
The gold standard for posterior stabilization in cases of instability, degenerative disease, trauma, and spinal deformity is transpedicular screws placement [4,5,6]. Their insertion is still difficult technically, though. The overall incidence of neurological, visceral, and vascular complications can reach 4–42%, with reported misplacement rates based on post-operative computed tomography (CT) scans reaching 11% [7,8,9]. To prevent medial or lateral pedicle wall breaches and anterior cortex perforation, accurate screw placement necessitates a deep comprehension of vertebral and pedicle morphometry.
Significantly affecting safe screw diameter, length, and trajectory are racial and ethnic variations in pedicle and vertebral dimensions [10,11]. Indian pedicle dimensions are frequently overestimated by Western morphometric standards, which could result in improper screw selection and a higher risk of complications [12]. Although earlier Indian research has looked at lower dorsal regions (Acharya et al.) or lumbar vertebrae (Mitra et al.), there is still a dearth of prospective CT-based morphometry that focuses on the thoracolumbar junction (T11–L2) in Western Indian populations [13,14].
To determine the ideal screw size, trajectory, and length, key morphometric parameters such as pedicle width, interpedicular distance (IPD), depth of anterior cortex, and transpedicular angle are crucial. To reduce complications, these parameters help surgeons choose the right implants and plan safe insertion trajectories.
In 200 Western Indian adults, this study establishes prospective CT-derived morphometric norms for the thoracolumbar junction. It then compares the results with previous Indian and international literature and offers clinical recommendations for transpedicular screw fixation in this population. These measurements should be interpreted in the context of Western Indian ethnicity, as substantial intra‑national variation in body habitus and skeletal dimensions is recognized across Indian regions.
The study was conducted at the Department of Orthopedics and Research Center at a tertiary care facility. Ethical approval taken from Institutional Ethics Committee, AIIMS Jodhpur (IEC No.- AIIMS/IEC/2022/4070) in June, 2022.
Study population
Consecutive adult patients presenting to the outpatient department with complaints of back pain who underwent clinical and radiological evaluation were screened, and only those with normal neurological examination and normal thoracolumbar imaging were included. A total of 200 patients (110 males [55%] and 90 females [45%]) meeting the eligibility criteria were included in the study.
Study design and setting
This prospective observational study was conducted at a tertiary care center in Western India (AIIMS Jodhpur, Rajasthan) between June 2021 and August 2023.
Inclusion criteria
- Adults aged ≥ge years with normal neurological examination
- Radiographs and CT scans of the thoracolumbar junction (T11, T12, L1 and L2) were reported as normal
- Adults with body mass index within 18.5–24.9 kg/m2
Exclusion criteria
- History of prior spinal surgery, deformities, or pre-existing spinal pathology
- Age <20 years
- Anomalies or Abnormalities at the thoracolumbar junction.
Data collection
All patients underwent anteroposterior and lateral radiographs of the thoracolumbar spine, followed by plain CT scanning of the thoracolumbar junction (T11–L2) using 1–2 mm axial slice thickness. Images were analyzed using digital imaging and communications in medicine viewer software. At each level, measurements were obtained separately on the right and left sides and then averaged to derive a single representative value per vertebra for analysis; we did not perform formal side‑to‑side comparative statistics. We restricted our analysis to transverse‑plane parameters that directly inform screw diameter, mediolateral trajectory, and length (pedicle width, IPD, transpedicular angle, and anterior cortex depth); sagittal parameters such as pedicle height and sagittal pedicle angle were not assessed.
The following parameters were measured bilaterally at each vertebral level (T11, T12, L1, and L2) with right and left values averaged:
- Pedicle width: Distance between medial and lateral cortices at the narrowest part of the pedicle isthmus, measured perpendicular to the pedicle axis (defined as the line bisecting the narrowest pedicle diameter) (Fig. 1)
- IPD: Distance between the medial surfaces of the right and left pedicles at the level of the isthmus (Fig. 1)
- Depth of anterior cortex (screw path length): Distance from the posterior aspect of the laminar cortex to the anterior cortex of the vertebral body, measured along the pedicle axis (Fig. 1)
- Transpedicular angle: Angle formed between a line passing through the pedicle axis and a line parallel to the vertebral body midline in the transverse plane (Fig. 1).
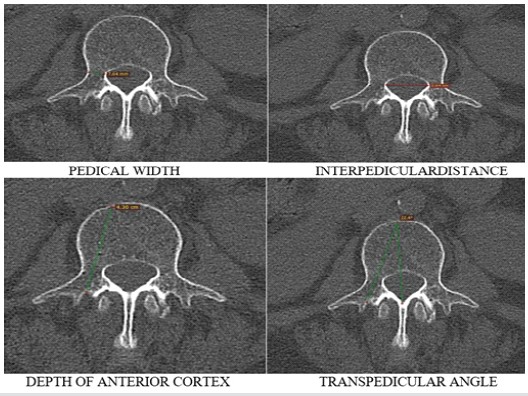
Figure 1: Different parameters measured in study.
All measurements were performed primarily by a single fellowship‑trained orthopedic surgeon, blinded to patient demographics. To assess reproducibility, a second observer independently repeated measurements on a random subset of 30 CT scans; interobserver reliability for all parameters was excellent (intraclass correlation coefficient >0.95).
Statistical analysis
Data were entered and analyzed using Microsoft Excel 365. Descriptive statistics (mean ± standard deviation, range) were calculated for all parameters. Sex-based comparisons were performed using unpaired t-tests with 95% confidence intervals. Statistical significance was set at P < 0.05.
Demographics
The study included 200 patients aged 20–70+ years. Age distribution showed the highest representation in the 50–59 years group (49 patients, 24.5%), followed by 40–49 years group (41 patients, 20.5%). Males comprised 55% (n = 110) and females 45% (n = 90) of the cohort (Table 1).
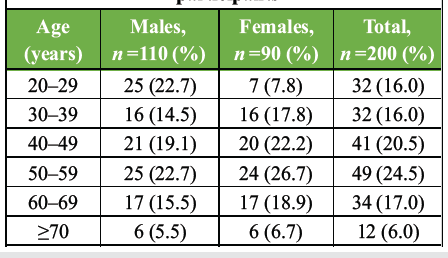
Table 1: Age and sex distribution of study participants
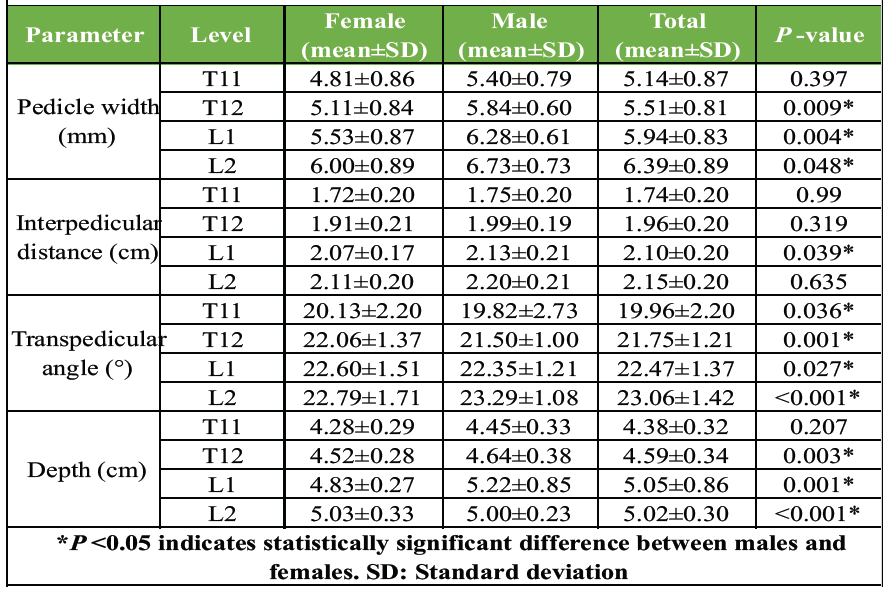
Table 2: Morphometric characteristics by sex and vertebral level (n=200)
Morphometric measurements
All morphometric parameters showed a caudal increase from T11 to L2 (Table 2). Sex-based differences were observed in multiple parameters. Mean pedicle width increased progressively from T11 (5.14 ± 0.87 mm) to L2 (6.39 ± 0.89 mm). Males demonstrated significantly greater pedicle width than females at T12 (P = 0.009) and L1 (P = 0.004), with a trend toward significance at L2 (P = 0.048). IPD increased caudally from T11 (1.74 ± 0.20 cm) to L2 (2.15 ± 0.20 cm). Significant sex differences were observed at L1 (P = 0.039), with males showing larger values. The transpedicular angle ranged from 19.96 ± 2.20° at T11 to 23.06 ± 1.42° at L2. Significant sex differences were observed at all vertebral levels (P < 0.05), with the most pronounced difference at L2 (P < 0.001). Anterior cortex depth peaked at L1 (5.05 ± 0.86 cm) and was minimal at T11 (4.38 ± 0.32 cm). Significant sex differences were noted at T12, L1, and L2 (all P < 0.01) (Table 2).
The thoracolumbar junction represents a critical transitional zone where posterior fixation with transpedicular screws is frequently required for trauma, deformity, and degenerative conditions [15]. Precise knowledge of regional morphometry, which differs greatly among ethnic groups, is necessary for successful screw placement [10,11]. This prospective CT-based study fills a major gap in population-specific data by providing detailed morphometric norms for the T11–L2 vertebrae in 200 Western Indian adults.
Pedicle width and clinical implications
According to our results, pedicle width gradually increases from T11 (5.14 ± 0.87 mm) to L2 (6.39 ± 0.89 mm), with males exhibiting noticeably larger dimensions than females at T12 and L1. According to Olsewski et al., lumbar pedicle widths in Caucasian subjects ranged from 7 to 10 mm, which is significantly smaller than those found in Western populations [16]. But closely correspond with other studies conducted in India. Acharya et al. reported lower dorsal values of 4.5–6.0 mm [14], whereas Mitra et al. found lumbar pedicle widths of 6.0–8.3 mm in males and 5.2–7.1 mm in females [13]. International research by Zindrick et al. and Kim et al. [12,17] is consistent with the caudal increase pattern and male predominance. Clinical recommendation: 4.5–5.5 mm for thoracic levels (T11–T12) and 5.5–6.5 mm for upper lumbar levels (L1–L2) are safe screw diameters for Western Indian patients, according to our data. Pedicle fracture and cortical breach are risks associated with using larger diameter screws made for Western populations.
With notable sex differences at L1, IPD increased from T11 (1.74 ± 0.20 cm) to L2 (2.15 ± 0.20 cm). Although our absolute values are smaller, this caudal widening trend is consistent with ethnic variations and is like findings by Marchesi et al. [18]. IPD measurements are essential for determining the size of the spinal canal and the risk of stenosis, which is especially important in degenerative diseases.
There were notable sex differences at every level of the transpedicular angle, which varied from 19.96 ± 2.20° at T11 to 23.06 ± 1.42° at L2. The degree of medial convergence necessary for a safe screw trajectory is indicated by these angles. Similar progressive increases from the thoracic to lumbar spine were reported by Zindrick et al. [17], with L5 exhibiting the steepest angle (29.8°).
According to our results, to maximize purchase and prevent medial wall breach, screws should be positioned at the thoracolumbar junction with 20–23° medial angulation.
The maximum screw path length was found at L1 (5.05 ± 0.86 cm), where the anterior cortex depth peaked. These measurements help to determine the ideal screw length, which is 40–45 mm for thoracic levels and 45–50 mm for lumbar levels. This ensures sufficient purchase without anterior perforation and damage to the great vessels.
Our study contributes T11–L2-specific information. Therefore, while our results may be broadly informative for Indian patients with similar anthropometric profiles, they cannot be assumed to represent Eastern, Northern, or Southern Indian populations without region-specific validation. Although Acharya et al. studied lower dorsal vertebrae (T10–L5) and Mitra et al. provided extensive lumbar data (L1–L5), neither study specifically addressed the thoracolumbar junction with our sample size [13,14]. The need for ethnicity-specific implant design and preoperative planning tools for the Indian population is further supported by our findings of narrower pedicles in comparison to Western norms. Our recommendations for screw diameter, length, and convergence are derived from morphometric measurements rather than from a linked surgical cohort, and we did not evaluate actual pedicle screw placement accuracy or clinical outcomes at each vertebral level. By restricting inclusion to radiologically normal thoracolumbar segments, we focused on defining normative morphometry; however, this reduces direct generalizability to patients with deformity, fractures, or advanced degeneration, who constitute a large proportion of those undergoing instrumentation.
The study’s large sample size (n = 200), prospective design, superior accuracy of CT-based measurements over conventional radiography, and particular attention to the clinically relevant T11–L2 region are its strengths.
Study limitations
The results represent regional, symptomatic adults rather than a true community-based, pan-Indian population because it was a single-center study from Western India with a hospital-based sample of back-pain patients. Selection bias and limited applicability to pathological spines (fracture, deformity, degeneration) may still exist even though only people with normal neurological examinations and thoracolumbar imaging were included. Multivariate modeling of morphometric predictors was not possible because the right and left pedicles were averaged, side-to-side asymmetry and age-stratified differences were not examined. We only evaluated four transverse-plane parameters on axial CT slices that were primarily 1–2 mm, with a few legacy scans up to 5 mm. We also did not use specialized three-dimensional (3D) reconstruction. Our recommendations for screw diameter, length, and trajectory are based on morphometric safety margins and have not yet been prospectively correlated with intraoperative screw placement accuracy or post-operative outcomes. Multicenter, multiregional validation studies are necessary before wider generalization.
The thoracolumbar junction (T11–L2) morphometric norms of 200 Western Indian adults are established in this prospective CT-based study. Important conclusions include: Safe screw parameters: 4.5–5.5 mm diameter (thoracic), 5.5–6.5 mm (lumbar), 40–50 mm length, and 20–23° medial angulation; progressive caudal increase in all parameters (width, IPD, angle, depth); significant sex differences requiring consideration in surgical planning; pedicle widths (5.14–6.39 mm) narrower than Western populations but consistent with Indian ethnic patterns. By improving surgical safety and accuracy in transpedicular screw fixation for Western Indian patients, these ethnicity-specific reference values lower complications in this biomechanically delicate area. For the Indian market, we recommend implementing these standards for preoperative planning and implant design. Future research should include multicenter cohorts from different Indian regions, incorporate standardized thin‑slice CT with 3D reconstruction, collect detailed anthropometric data, and prospectively correlate these morphometric recommendations with pedicle screw placement accuracy and clinical outcomes.
For safe transpedicular fixation in Western Indian thoracolumbar junction cases, we advise using 4.5–5.5 mm screws (thoracic T11–T12) and 5.5–6.5 mm screws (lumbar L1–L2) with 40–50 mm length and converging trajectory (20–23°).
References
- 1. Iorio JA, Jakoi AM, Singla A. Biomechanics of degenerative spinal disorders. Asian Spine J 2016;10:377-84. [Google Scholar] [PubMed]
- 2. Beisse R. Endoscopic surgery on the thoracolumbar junction of the spine. Eur Spine J 2006;15:687-704. [Google Scholar] [PubMed]
- 3. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine (Phila Pa 1976) 1983;8:817-31. [Google Scholar] [PubMed]
- 4. Cho W, Cho SK, Wu C. The biomechanics of pedicle screw-based instrumentation. J Bone Joint Surg Br 2010;92:1061-5. [Google Scholar] [PubMed]
- 5. Goel VK, Gilbertson LG. Basic science of spinal instrumentation. Clin Orthop Relat Res 1997;335:10-31. [Google Scholar] [PubMed]
- 6. Hart RA, Hansen BL, Shea M, Hsu F, Anderson GJ. Pedicle screw placement in the thoracic spine: A comparison of image-guided and manual techniques in cadavers. Spine (Phila Pa 1976) 2005;30:E326-31. [Google Scholar] [PubMed]
- 7. Kosmopoulos V, Schizas C. Pedicle screw placement accuracy: A meta-analysis. Spine (Phila Pa 1976) 2007;32:E111-20. [Google Scholar] [PubMed]
- 8. Merloz P, Tonetti J, Pittet L, Coulomb M, Lavallee S, Sautot P. Pedicle screw placement using image guided techniques. Clin Orthop Relat Res 1998;354:39-48. [Google Scholar] [PubMed]
- 9. Laine T, Lund T, Ylikoski M, Lohikoski J, Schlenzka D. Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-40. [Google Scholar] [PubMed]
- 10. Christodoulou AG, Apostolou T, Ploumis A, Terzidis I, Hantzokos I, Pournaras J. Pedicle dimensions of the thoracic and lumbar vertebrae in the Greek population. Clin Anat 2005;18:404-8. [Google Scholar] [PubMed]
- 11. Schwarzenbach O, Berlemann U, Jost B, Visarius H, Arm E, Langlotz F, et al. Accuracy of computer-assisted pedicle screw placement. An in vivo computed tomography analysis. Spine (Phila Pa 1976) 1997;22:452-8. [Google Scholar] [PubMed]
- 12. Kim NH, Lee HM, Chung IH, Kim HJ, Kim SJ. Morphometric study of the pedicles of thoracic and lumbar vertebrae in Koreans. Spine (Phila Pa 1976) 1994;19:1390-4. [Google Scholar] [PubMed]
- 13. Mitra SR, Datir SP, Jadhav SO. Morphometric study of the lumbar pedicle in the Indian population as related to pedicular screw fixation. Spine (Phila Pa 1976) 2002;27:453-9. [Google Scholar] [PubMed]
- 14. Acharya S, Dorje T, Srivastava A. Lower dorsal and lumbar pedicle morphometry in Indian population: A study of four hundred fifty vertebrae. Spine (Phila Pa 1976) 2010;35:E378-84. [Google Scholar] [PubMed]
- 15. Vaccaro AR, An HS, Lin S, Sun S, Balderston RA, Cotler JM. Noncontiguous injuries of the spine. J Spinal Disord 1992;5:320-9. [Google Scholar] [PubMed]
- 16. Olsewski JM, Simmons EH, Kallen FC, Mendel FC, Severin CM, Berens DL. Morphometry of the lumbar spine: Anatomical perspectives related to transpedicular fixation. J Bone Joint Surg Am 1990;72:541-9. [Google Scholar] [PubMed]
- 17. Zindrick MR, Wiltse LL, Doornik A, Widell EH, Knight GW, Patwardhan AG, et al. Analysis of the morphometric characteristics of the thoracic and lumbar pedicles. Spine (Phila Pa 1976) 1987;12:160-6. [Google Scholar] [PubMed]
- 18. Marchesi D, Schneider E, Glauser P, Aebi M. Morphometric analysis of the thoracolumbar and lumbar pedicles, anatomo-radiologic study. Surg Radiol Anat 1988;10:317-22. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report
July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report April 1, 2026 Intraoperative Assessment of Combined Anteversion Using the Ranawat Technique with a Smartphone Application: A Prospective Computed Tomography-based Agreement Study in Uncemented Total Hip Arthroplasty
April 1, 2026 Intraoperative Assessment of Combined Anteversion Using the Ranawat Technique with a Smartphone Application: A Prospective Computed Tomography-based Agreement Study in Uncemented Total Hip Arthroplasty January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review
January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review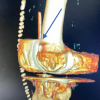 December 1, 2025 3D Computed Tomography-Guided Management of Retained Surgical Drain in Total Knee Arthroplasty: A Case Report and Technical Note
December 1, 2025 3D Computed Tomography-Guided Management of Retained Surgical Drain in Total Knee Arthroplasty: A Case Report and Technical Note