
Smartphone-assisted intraoperative assessment of combined anteversion using the Ranawat technique provides a practical, low-cost method in uncemented total hip arthroplasty, particularly where navigation or robotic systems are unavailable.
Dr. Safia Sultana, Department of Orthopaedics, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana, India. E-mail: sultanasafia2017@gmail.com
Abstract
Introduction: Optimal component positioning is critical for stability following total hip arthroplasty (THA). Combined anteversion (CA), incorporating both acetabular and femoral component orientation, has been proposed as a more reliable stability parameter than isolated acetabular positioning. However, accurate intraoperative assessment of CA without navigation remains challenging. This study prospectively evaluated the reliability and feasibility of surgeon-estimated CA using the Ranawat coplanar test compared with post-operative computed tomography (CT) measurements and correlated these findings with short-term functional outcomes.
Materials and Methods: This prospective observational study included 45 consecutive patients undergoing uncemented THA at a single tertiary care center. Intraoperative CA was estimated using the Ranawat coplanar test with smartphone-assisted goniometric measurement. Post-operative CT scans were used to calculate CA using Widmer’s formula. Agreement between intraoperative and CT measurements was assessed using paired statistical analysis and the intraclass correlation coefficient (ICC). Functional outcomes were evaluated using the Harris Hip Score (HHS) over 6 months.
Results: Mean intraoperative CA was 34.13° ± 8.39°, and mean CT-calculated CA was 36.01° ± 13.08°, with a mean difference of 1.88° (P = 0.177). Moderate agreement was observed (ICC = 0.65; 95% CI: 0.47–0.79). Mean HHS improved from 46.16 preoperatively to 90.87 at 6 months.
Conclusion: Intraoperative CA estimation using the Ranawat coplanar test demonstrated acceptable agreement with CT-based measurements.
Keywords: Combined anteversion, total hip arthroplasty, component positioning, computed tomography, intraoperative assessment of combined anteversion, Ranawat technique.
Total hip arthroplasty (THA) has revolutionized the treatment of end-stage hip arthritis, with success dependent critically on optimal component positioning[1]. While Lewinnek’s acetabular “safe zone” (40° ± 10° inclination and 15° ± 10° anteversion) has guided cup placement for decades [2], accumulating evidence demonstrates that isolated acetabular positioning is insufficient for stability, particularly with cementless femoral stems where anatomic constraints unpredictably influence orientation [3,4]. The concept of combined anteversion (CA), i.e., the sum of acetabular and femoral anteversion, was introduced by McKibbin based on anatomical studies, which showed physiological CA ranges from 30° to 40° [5], and has since been applied to THA [6]. Widmer’s formula (CA = Cup Anteversion + 0.7 × Femoral Anteversion, optimal target 37.3°) [7] and clinical studies demonstrating a 6.9-fold increased dislocation risk outside the 40–60° CA range [8] have established CA as a more comprehensive parameter for stability. Previous studies have further validated this concept [3,9]. The Ranawat coplanar test is a clinical method that provides intraoperative CA assessment [10], though studies comparing surgeon estimates with computed tomography (CT) measurements show precision values of 11–17° and errors exceeding 10° in 23% of cases [11]. A CT scan is the best method to assess exact component positioning in multiple planes [12,13]. While navigation and robotic systems offer enhanced precision, their prohibitive costs limit accessibility in resource-constrained settings [14]. Previous studies have evaluated surgeon estimation accuracy for isolated acetabular [12] or femoral [11] components, but a comprehensive assessment of CA using the Ranawat technique against post-operative CT measurements of the version remains limited. The purpose of this study was to prospectively evaluate the reliability of surgeon estimation of CA with a smartphone application using the Ranawat coplanar test in uncemented THA, by comparing with post-operative CT scan calculations, and to correlate these measurements with short-term functional outcomes.
This study was designed as a single-center prospective observational study to assess the feasibility and reliability of surgeon-estimated CA in routine practice. This study included 45 consecutive patients who underwent uncemented THA at our tertiary care center. Institutional ethics committee approval was obtained (No: 1310/2022; Date: March 30, 2022), and all patients provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki. Patients with osteoarthritis of the hip who consented to the study were included, and patients with active infection, medical contraindications to surgery, ipsilateral femoral deformity, or patients requiring cemented fixation were excluded from the study. Standard pre-operative radiographs of the affected hip and pelvis were taken before surgery and in the post-operative period, along with a CT scan from the lumbar spine (L2) to the knee for assessment of CA. Functional outcome was analyzed using the Harris Hip Score (HHS) [15] in the pre-operative and post-operative period. All procedures were performed by two senior surgeons (KCS, PC) using the posterior approach with patients in the lateral decubitus position under combined spinal-epidural anesthesia. The operating table was positioned horizontally without tilt using a spirit level to standardize pelvic orientation. Following standard capsulotomy and femoral head dislocation, acetabular preparation proceeded with sequential reaming. Cup positioning targeted anatomical anteversion by aligning the inferior edge parallel to the transverse acetabular ligament [16,17], an important anatomical landmark for patient-specific cup orientation. After press-fit cup implantation, femoral canal preparation and uncemented stem insertion followed. Intraoperative acetabular inclination and anteversion were estimated by the surgeon using anatomical landmarks (transverse acetabular ligament, anterior and posterior walls) and external guides [16,17] (Fig. 1).
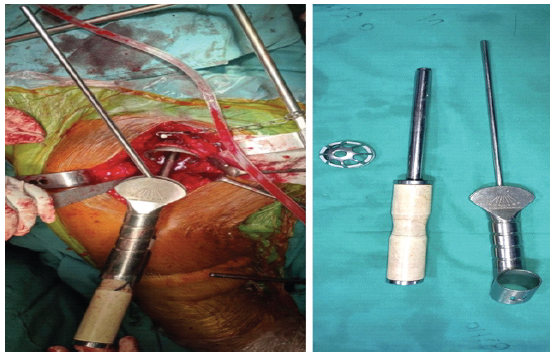
Figure 1: Acetabular positioning guides.
Intraoperative CA assessment
Following trial reduction, CA was assessed using the Ranawat coplanar test [10]. With the hip at neutral flexion-extension, the leg was internally rotated until the femoral head became coplanar with the acetabular cup base. A clinical photograph was captured from the foot end of the operating table with the tibia visible against a horizontal reference. The internal rotation angle was measured using a smartphone application (Image Meter, Android) [18], installed on a single standardized Android smartphone (Redmi Note 10 Pro Max model used consistently for all cases). Calibration was performed before each use by verifying measurements against a predetermined reference angle on a flat surface. This technique has been previously used intra-operatively to assess acetabular component orientation in THA [19,20,21] (Fig. 2). The resulting internal rotation angle represented the intraoperative CA estimate. The elevated acetabular liner was placed appropriately based on the CA value obtained to provide additional support.
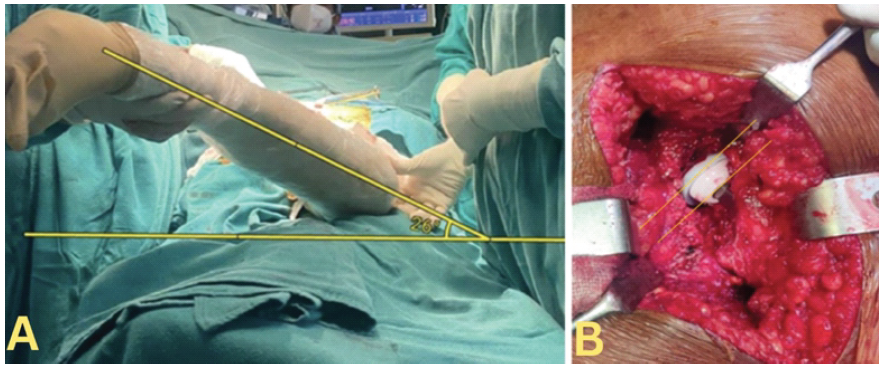
Figure 2: Smartphone application (Imagemeter) measuring the internal rotation of the hip from the foot end of the table. A clinical photograph was captured from the foot end of the operating table with the tibia visible against a horizontal reference, and the angle made by the tibia with the horizontal is measured as combined anteversion (a). With the hip at neutral flexion-extension, the leg was internally rotated until the femoral head became coplanar with the acetabular cup base (b).
Post-operative assessment
Anteroposterior pelvis and cross-table lateral hip radiographs were obtained on the 2nd post-operative day, along with a CT-scan (from L4 vertebra to distal femoral condyles). Acetabular anteversion, inclination, and femoral anteversion were measured on CT images using standardized radiological techniques by two qualified surgeons who were not part of the operating team [13,22] (Figs. 3 and 4). CA was calculated using Widmer’s formula: CA = acetabular anteversion + 0.7 × femoral anteversion [7]. Measurements from the contralateral native hip served as anatomical reference values.
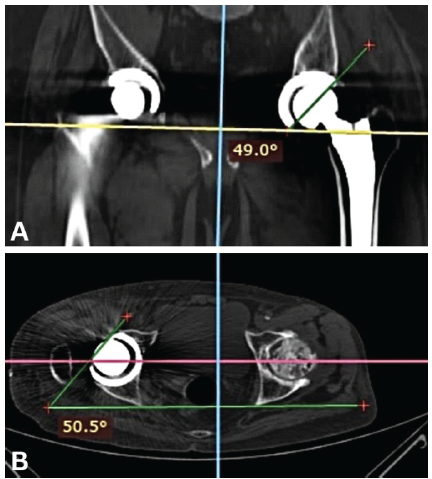
Figure 3: Computed tomography measurement of acetabular inclination (a) and acetabular anteversion (b).
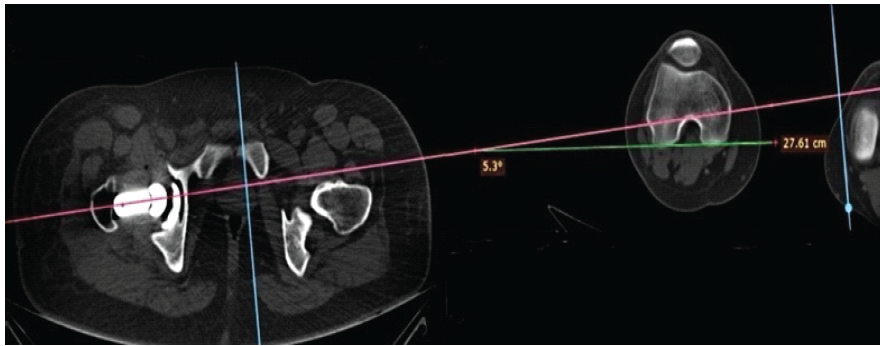
Figure 4: Computed tomography measurement of femoral anteversion.
Follow-up and outcomes
Patients were followed at 10 days, 1 month, 3 months, and 6 months. Functional outcome was assessed by independent surgeons who were not part of the operating team, using HHS [15] at each visit, graded as poor (<70), fair (70–79), good (80–89), or excellent (90–100). Complications, including dislocation, infection, and periprosthetic fracture, were recorded.
Statistical analysis
Continuous variables are presented as mean ± standard deviation. Paired t-tests compared intraoperative estimates with CT measurements. Statistical significance was set at P < 0.05. Agreement between intraoperative surgeon-estimated CA and post-operative CT-calculated CA was assessed using the intraclass correlation coefficient (ICC). A two-way mixed-effects model with absolute agreement for single measurements (ICC [3,1]) was used to compare the two measurement methods. ICC values were interpreted as poor (<0.5), moderate (0.5–0.75), good (0.75–0.9), or excellent (>0.9).
Patient demographics and surgical characteristics (Table 1)
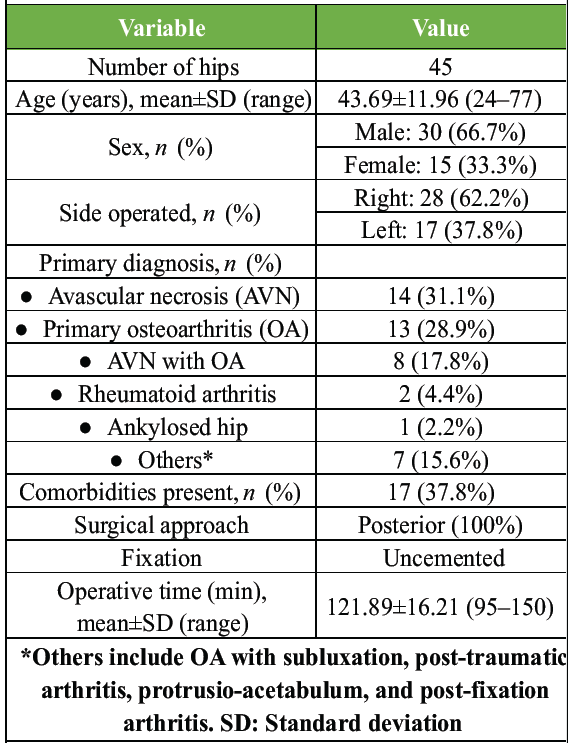
Table 1: Patient demographics and surgical characteristics (n=45)
Mean intraoperative CA assessed by the Ranawat test was 34.133° ± 8.3879° (range 13.5–50.0°). Post-operative CT-calculated CA was 36.0147° ± 13.08456° (range 8.96–67.20°). The mean difference of 1.88° was not statistically significant (P = 0.177). Intraclass correlation analysis demonstrated moderate agreement between intraoperative surgeon-estimated CA and post-operative CT-calculated CA (ICC = 0.65; 95% CI, 0.47–0.79). 73.33% of patients (n = 33) had CA values within the acceptable safe zone of 20–50°. Post-operative CA was significantly greater than contralateral native hip CA (27.1016° ± 7.16071°, P = 0.001) (Table 2).
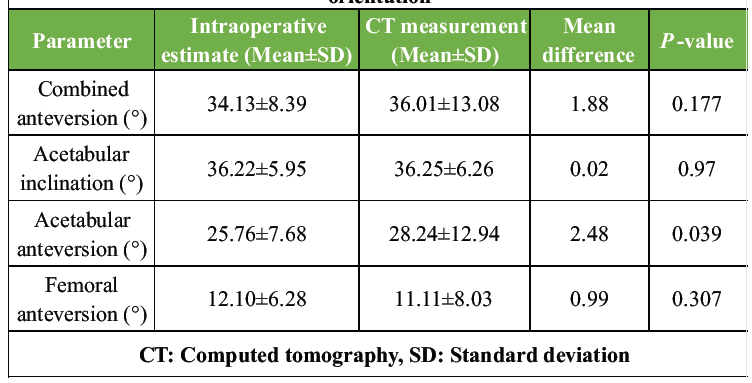
Table 2: Comparison of intraoperative and CT-measured component orientation
Intraoperative estimate of acetabular inclination (36.22° ± 5.950°) closely matched CT measurement (36.247° ± 6.2632°), with a mean difference of 0.0244° (P = 0.970). Intraoperative estimate of acetabular anteversion (25.76° ± 7.679°) was significantly lower than CT measurement (28.236° ± 12.9445°), with a mean difference of 2.48° (P = 0.039). Post-operative acetabular anteversion exceeded contralateral native hip (18.691° ± 6.2671°, P = 0.001). Post-operative femoral anteversion measured on CT was 11.1116° ± 8.03379° (range −10.00° to 30.10°). No significant difference existed between the operated side and contralateral native femoral anteversion (12.6822° ± 7.73181°, P = 0.347).
Functional outcomes and complications
Mean pre-operative HHS was 46.16 ± 9.714 (range 30–65). At 1 month postoperatively, HHS improved to 89.67 ± 4.338 (range 77–96, P = 0.001). At 6 months, HHS reached 90.87 ± 3.202 (range 83–96, P = 0.001 vs. pre-operative; P = 0.001 vs. 1 month, mean improvement 1.2 points). At 6 months, 40 hips (88.9%) achieved excellent results (HHS ≥90), and 5 hips (11.1%) achieved good results (HHS 80–89) (Table 3).
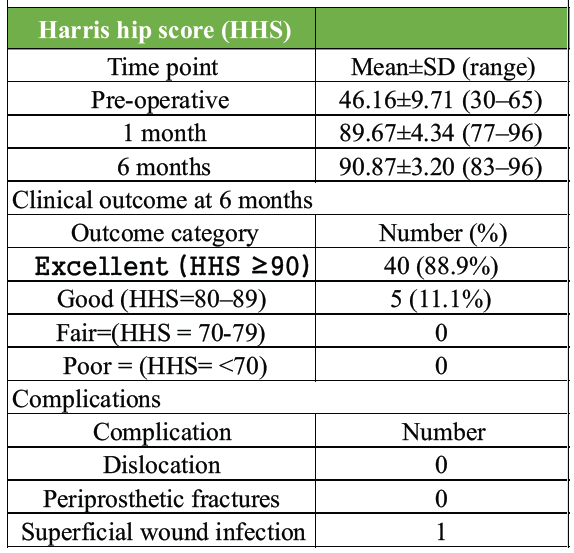
Table 3: Functional outcomes and complications
No cases of dislocations or periprosthetic fractures occurred during the 6-month follow-up. There was one case of superficial wound infection, which was managed with debridement and closure, along with antibiotics, that healed without any further complications.
Accurate restoration of CA in THA is critical to optimize stability, range of motion, impingement-free articulation, and implant longevity. Malposition of either the acetabular or femoral component can predispose to instability, edge loading, accelerated wear, and early failure [22,23,24]. While Lewinnek et al. originally described a “safe zone” for acetabular positioning [2], subsequent investigations have emphasized that component positioning must be interpreted in the context of femoral version; thus highlighting the importance of CA [7,25,26]. Ranawat originally proposed the concept of CA to reduce the risk of instability by accounting for both femoral and acetabular components [25]. Subsequent refinements by Widmer and Zurfluh mathematically modeled optimal CA to minimize impingement [7], and Dorr et al. emphasized functional CA based on spinopelvic dynamics [26]. Compared to these CT-based or navigation-based approaches, the present study evaluated a simple intraoperative clinical assessment augmented by a smartphone goniometer, thereby offering a cost-effective and widely accessible alternative. In the present prospective CT-based agreement study, the mean intraoperative CA assessed using the Ranawat technique with a smartphone application was 34.13° ± 8.38°, whereas post-operative CT-calculated CA was 36.01° ± 13.08°. The mean difference of 1.88° between the two methods was not statistically significant (P = 0.177), indicating no systematic bias between intraoperative estimation and CT-based measurement. Intraclass correlation analysis demonstrated moderate agreement (ICC = 0.65; 95% CI, 0.47–0.79). Although this level of agreement indicates reasonable clinical correlation between intraoperative estimation and CT-based measurement, it also suggests variability that may affect reproducibility, particularly among less experienced surgeons. This CA value approximates Widmer’s optimal target of 37.3° [7] and falls within the safe range of 25–45° advocated by Dorr et al. [3] and 40–60° by Jolles et al. [8], corroborated by excellent functional outcomes (mean HHS 90.9 at 6 months) and absence of dislocation during follow-up. While Dorr et al. [11] reported poor precision of the Ranawat test in a navigation-based comparison, the present study demonstrates improved performance, likely attributable to systematic photographic documentation with smartphone goniometry [19,20,21] rather than pure visual estimation, and strict adherence to standardized patient positioning. Our findings are consistent with Nakashima et al., [9] who reported a significant reduction in dislocation rates when CA principles were applied. Importantly, 73.33% of patients (n = 33) achieved post-operative CA values within the generally accepted safe zone of 20–50°, as described in the literature [7,25]. This proportion is comparable to reports from conventional instrumentation series and supports the practical applicability of the Ranawat-based method in uncemented THA. Although the post-operative CA was significantly greater than the contralateral native hip CA (27.10° ± 7.16°, P = 0.001), no instability events occurred during follow-up, suggesting that slightly increased anteversion within the acceptable range may not adversely affect short-term outcomes. Regarding individual component positioning, intraoperative acetabular inclination (36.22° ± 5.95°) showed excellent agreement with CT measurement (36.25° ± 6.26°), with a negligible mean difference. This finding reflects the reliability of goniometer-assisted assessment for coronal plane positioning, consistent with previous reports validating digital methods for acetabular alignment, other than navigation [27,28]. In contrast, intraoperative acetabular anteversion (25.76° ± 7.68°) was significantly lower than CT-measured anteversion (28.24° ± 12.94°), with a mean difference of 2.48° (P = 0.039). This discrepancy may be attributed to differences between operative reference planes and CT-based anatomical reference planes, as well as the influence of pelvic tilt [29,30]. Post-operative acetabular anteversion was also significantly higher than that of the contralateral native hip (18.69° ± 6.27°, P = 0.001), which may reflect intentional targeting of a higher anteversion to compensate for femoral version variability. Post-operative femoral anteversion measured on CT was 11.11° ± 8.03°, comparable to the contralateral native femur (12.68° ± 7.73°, P = 0.347). This suggests that the uncemented femoral component largely reproduced native femoral version, consistent with prior studies demonstrating that modern tapered stems tend to follow native femoral anatomy [31,32]. The relatively wide range (−10–30°) underscores the inherent variability in femoral anatomy and reinforces the importance of evaluating combined rather than isolated component anteversion. Functional outcomes were excellent. Mean HHS improved significantly from 46.16 preoperatively to 89.67 at 1 month and 90.87 at 6 months (P = 0.001). At 6 months, 88.9% of hips achieved excellent results, and 11.1% achieved good results, with no fair or poor outcomes. Notably, there were no dislocations or periprosthetic fractures during follow-up. Only one superficial wound infection occurred, successfully managed with debridement and antibiotics. The absence of instability events further supports the adequacy of the achieved CA range, consistent with literature correlating optimized CA with reduced dislocation risk [24,25,26]. This study has several limitations. First, the small sample size reflects ethical and practical constraints related to post-operative CT imaging, which is not routinely performed following THA and involves additional radiation exposure. Although the prospective design represents a methodological strength, it also limited recruitment feasibility and contributed to the relatively small sample size. Second, this was a single-center study performed at a tertiary referral institution, which may introduce institutional practice bias and limit external validity. Third, the procedures were performed by two experienced surgeons, and the intraoperative estimation relied on surgeon’ judgment using the Ranawat technique; therefore, the reproducibility of this method may vary among surgeons with different levels of experience. Furthermore, interobserver and intraobserver reliability of CT-based measurements of component anteversion were not assessed and constitute a further limitation of this study. In addition, the short-term follow-up does not allow assessment of long-term complications or implant survivorship. Finally, the use of a specific smartphone application and intraoperative positioning techniques of patients may introduce potential measurement variability related to pelvic tilt, camera positioning, and limb alignment. The principal strength of this study lies in its prospective design and use of a smartphone goniometer application to assess the CA using the Ranawat technique, offering a low-cost and practical solution, particularly in resource-limited settings. Longer follow-up is required to determine whether these alignment parameters translate into sustained functional benefit and implant survivorship.
The surgeon’s estimation of CA using the Ranawat coplanar test with smartphone-assisted measurement demonstrates moderate agreement with CT-based calculations. In settings where navigation and robotic technologies are not readily available, this technique represents a fair way of estimation of CA in uncemented THA, although intersurgeon variability may influence the consistency of results.
In resource-limited settings where component positioning relies heavily on surgeon expertise, smartphone-assisted assessment of combined anteversion using the Ranawat coplanar technique provides a simple and accessible intraoperative adjunct that may aid component orientation and improve surgical precision in uncemented total hip arthroplasty.
References
- 1. Knight SR, Aujla R, Biswas SP. Total hip arthroplasty – over 100 years of operative history. Orthop Rev (Pavia) 2011;3:e16. [Google Scholar] [PubMed]
- 2. 2 Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am 1978;60:217-20. [Google Scholar] [PubMed]
- 3. 3 Dorr LD, Malik A, Dastane M, Wan Z. Combined anteversion technique for total hip arthroplasty. Clin Orthop Relat Res 2009;467:119-27. [Google Scholar] [PubMed]
- 4. 4 Pierchon F, Pasquier G, Cotten A, Fontaine C, Clarisse J Duquennoy A. Causes of dislocation of total hip arthroplasty. CT study of component alignment. J Bone Joint Surg Br 1994;76:45-8. [Google Scholar] [PubMed]
- 5. 5 McKibbin B. Anatomical factors in the stability of the hip joint in the newborn. J Bone Joint Surg Br 1970;52:148-59. [Google Scholar] [PubMed]
- 6. 6 Fukunishi S, Fukui T, Nishio S, Fujihara Y, Okahisa S, Yoshiya S. Combined anteversion of the total hip arthroplasty implanted with image-free cup navigation and without stem navigation. J Orthop Surg (Hong Kong) 2014;22:62-5. [Google Scholar] [PubMed]
- 7. 7 Widmer KH, Zurfluh B. Compliant positioning of total hip components for optimal range of motion. J Orthop Res 2004;22:815-21. [Google Scholar] [PubMed]
- 8. 8 Jolles BM, Zangger P, Leyvraz PF. Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17:282-8. [Google Scholar] [PubMed]
- 9. 9 Nakashima Y, Hirata M, Akiyama M, Itokawa T, Yamamoto T, Motomura G, et al. Combined anteversion technique reduced the dislocation in cementless total hip arthroplasty. Int Orthop 2014;38:27-32. [Google Scholar] [PubMed]
- 10. 10 Lucas DE, Scott RD. Pearls: Clinical application of Ranawat’s sign. Clin Orthop Relat Res 2017;475:1289-91. [Google Scholar] [PubMed]
- 11. 11 Dorr LD, Wan Z, Malik A, Zhu J, Dastane M, Deshmane P. A comparison of surgeon estimation and computed tomographic measurement of femoral component anteversion in cementless total hip arthroplasty. J Bone Joint Surg Am 2009;91:2598-604. [Google Scholar] [PubMed]
- 12. 12 Saxler G, Marx A, Vandevelde D, Langlotz U, Tannast M, Wiese M, et al. The accuracy of free-hand cup positioning–a CT based measurement of cup placement in 105 total hip arthroplasties. Int Orthop 2004;28:198-201. [Google Scholar] [PubMed]
- 13. 13 Fujishiro T, Hayashi S, Kanzaki N, Hashimoto S, Kurosaka M, Kanno T, et al. Computed tomographic measurement of acetabular and femoral component version in total hip arthroplasty. Int Orthop 2014;38:941-6. [Google Scholar] [PubMed]
- 14. 14 Domb BG, El Bitar YF, Sadik AY, Stake CE, Botser IB. Comparison of robotic-assisted and conventional acetabular cup placement in THA: A matched-pair controlled study. Clin Orthop Relat Res 2014;472:329-36. [Google Scholar] [PubMed]
- 15. 15 Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am 1969;51:737-55. [Google Scholar] [PubMed]
- 16. 16 Archbold HA, Mockford B, Molloy D, McConway J, Ogonda L, Beverland D. The transverse acetabular ligament: An aid to orientation of the acetabular component during primary total hip replacement: A preliminary study of 1000 cases investigating postoperative stability J Bone Joint Surg Br 2006;88:883-6. [Google Scholar] [PubMed]
- 17. 17 Salal MH. transverse acetabular ligament as an anatomical landmark for intraoperative cup anteversion in primary total hip replacement. J Coll Physicians Surg Pak 2017;27:642-4. [Google Scholar] [PubMed]
- 18. 18 Available from: https://play.google.com/store/apps/details?id=de.dirkfarin.imagemeter&pcampaignid=MKT-Other-global-all-co-prtnr-py-PartBadge-Mar2515-1. Last accessed 16/02/2026. [Google Scholar] [PubMed]
- 19. 19 Peters FM, Greeff R, Goldstein N, Frey CT. Improving acetabular cup orientation in total hip arthroplasty by using smartphone technology. J Arthroplasty 2012;27:1324-30. [Google Scholar] [PubMed]
- 20. 20 Pongkunakorn A, Chatmaitri S, Diewwattanawiwat K. Use of smartphone to improve acetabular component positioning in total hip athroplasty: A comparative clinical study. J Orthop Surg (Hong Kong). 2019;27(1):2309499019825578. doi:10.1177/2309499019825578 [Google Scholar] [PubMed] [CrossRef]
- 21. 21 van Duren BH, Royeca JM, Cunningham CM, Lamb JN, Brew CJ, Pandit H. Can the use of an inclinometer improve acetabular cup inclination in total hip arthroplasty? A review of the literature. Hip Int. 2021;31(5):609-617. doi:10.1177/1120700020946716. [Google Scholar] [PubMed] [CrossRef]
- 22. 22 Murray DW. The definition and measurement of acetabular orientation. J Bone Joint Surg Br 1993;75:228-32. [Google Scholar] [PubMed]
- 23. 23 Biedermann R, Tonin A, Krismer M, Rachbauer F, Eibl G, Stöckl B. Reducing the risk of dislocation after total hip arthroplasty: The effect of orientation of the acetabular component. J Bone Joint Surg Br 2005;87:762-9. [Google Scholar] [PubMed]
- 24. 24 Dorr LD, Wan Z. Causes of and treatment protocol for instability of total hip replacement. Clin Orthop Relat Res 1998;355:144-51. [Google Scholar] [PubMed]
- 25. 25 Ranawat CS, Maynard MJ. Modern techniques of cemented total hip arthroplasty. Tech Orthop 1991;6:17-25. [Google Scholar] [PubMed]
- 26. 26 Dorr LD, Malik A, Wan Z, Long WT, Harris M. Precision and bias of imageless computer navigation and surgeon estimates for acetabular component position. Clin Orthop Relat Res 2007;465:92-9. [Google Scholar] [PubMed]
- 27. 27 Prasad Patro B, Roy M, Mahapatra MM, Jain D. The economical and reliable image free navigation system for acetabular cup implantation in total hip arthroplasty. J Clin Orthop Trauma 2025;65:102991. [Google Scholar] [PubMed]
- 28. 28 Peters CL, McPherson E, Jackson JD, Erickson JA. Reduction in early dislocation rate with large-diameter femoral heads in primary total hip arthroplasty. J Arthroplasty 2007;22 6 Suppl 2:140-4. [Google Scholar] [PubMed]
- 29. 29 Tannast M, Zheng G, Anderegg C, Burckhardt K, Langlotz F, Ganz R, et al. Tilt and rotation correction of acetabular version on pelvic radiographs. Clin Orthop Relat Res 2005;438:182-90. [Google Scholar] [PubMed]
- 30. 30 Lembeck B, Mueller O, Reize P, Wuelker N. Pelvic tilt makes acetabular cup navigation inaccurate. Acta Orthop 2005;76:517-23. [Google Scholar] [PubMed]
- 31. 31 Sugano N, Noble PC, Kamaric E, Salama JK, Ochi T, Tullos HS. The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br 1998;80:711-9. [Google Scholar] [PubMed]
- 32. 32 Wines AP, McNicol D. Computed tomography measurement of the accuracy of component version in total hip arthroplasty. J Arthroplasty 2006;21:696-701. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report
July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem
July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach