
Tension‑free patch reconstruction (ovine ECM) for tibialis anterior herniation can relieve pain and lower the risk of post-operative compartment syndrome compared with tight primary closure.
Dr. Hitarth Gathani, Department of Orthopaedics, SportsMed, Mumbai, Maharashtra, India. E-mail: hitarthjgathani@gmail.com
Abstract
Introduction: Muscle herniation occurs when muscle protrudes through a defect in its deep fascia. The tibialis anterior is most frequently involved and symptomatic cases present with an activity‑dependent bulge and pain. Dynamic ultrasonography (USG) confirms the diagnosis while magnetic resonance imaging can delineate the defect and exclude other differentials.
Case Report: A 35‑year‑old male had exertional anterior shin pain with a reducible swelling over mid‑tibialis anterior that accentuated on dorsiflexion. Dynamic USG confirmed a focal fascial defect with herniation. After failed conservative treatment, the defect was bridged using an inlay ovine extracellular matrix patch to avoid high‑tension primary closure. Post-operative rehabilitation enabled return to full sport within weeks; he remained symptom‑free at follow‑up.
Conclusion: For tibialis anterior herniation, tension‑free patch reconstruction is a reasonable option to preserve function and reduce the risk of compartment syndrome associated with tight fascial approximation.
Keywords: Tibialis anterior herniation, myofascial herniation, dynamic ultrasonography, ovine extracellular matrix, patch repair, compartment syndrome.
Muscle herniation is an uncommon but important cause of exertional leg pain. It results from a focal defect or weakness in the deep fascia allowing underlying muscle to protrude into the subcutaneous plane. The condition may be congenital, related to fascial weakness, or acquired following trauma, repetitive micro‑stress, or increased intracompartmental pressures. Among the leg compartments, the anterior compartment is particularly predisposed due to its relatively tight fascia and superficial location of the tibialis anterior muscle. Among the leg compartments, the anterior compartment—especially the tibialis anterior—has the tightest investing fascia and is most often affected [1]. Patients typically describe an activity‑dependent, soft, sometimes reducible mass that enlarges with dorsiflexion and lessens at rest; pain, cramping, or localized tenderness can occur [1,2]. Dynamic ultrasonography (USG) is the diagnostic test of choice, with magnetic resonance imaging (MRI) reserved for equivocal cases or to exclude alternative pathology [2]. Asymptomatic or mildly symptomatic hernias are treated conservatively; surgery is considered for persistent pain, functional limitation, or cosmetic concern. Because tight primary fascial closure can precipitate anterior compartment syndrome, many authors advocate tension‑free techniques, including patch or mesh augmentation for larger defects [3,4,7]. We report a tibialis anterior herniation treated with an inlay ovine extracellular matrix (ECM) patch and review the rationale for reinforced closure.
A 35‑year‑old male presented with persistent anterior shin pain exacerbated by running and prolonged walking. The patient reported a gradually progressive swelling over the anterior aspect of the leg, which became more prominent during physical activity and reduced at rest. There was no history of acute trauma, but the patient was physically active and engaged in regular sports. Examination revealed a soft, well‑defined swelling over the mid‑portion of the tibialis. There were no sensory or vascular deficits, and strength across ankle dorsiflexors and plantarflexors was intact. MRI [Fig. 1,2] was suggestive of fat stranding at the site of the herniation and was not conclusive of the diagnosis. Dynamic USG [Fig. 1] was done with the foot dorsiflexion and after some jogging which confirmed a focal defect in the tibialis anterior fascia with muscle herniation which was not visible on regular ultrasound.
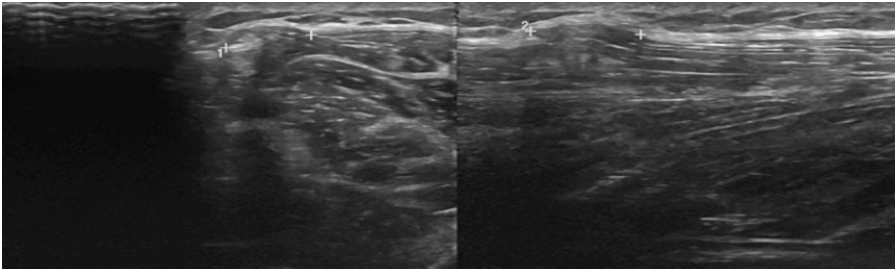
Figure 1: Dynamic ultrasonography of tibialis anterior herniation. Short-axis ultrasonography demonstrating a focal fascial defect with protrusion of tibialis
anterior on resisted dorsiflexion. Location: mid-anterior leg; Timing: Pre-operative.
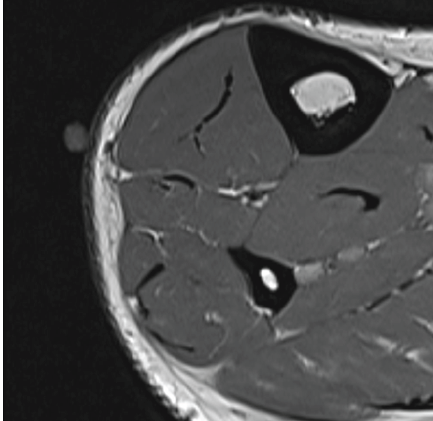
Figure 2: Magnetic resonance imaging (MRI) suggestive of fat stranding.
Axial MRI showing fat stranding at the site of defect. Location: Mid-anterior
leg; Timing: Pre-operative.
An initial trial of rest, activity modification, and compression stockings failed to relieve symptoms. Given functional limitation, operative management was undertaken. Intraoperatively, a 2 × 2 cm discrete fascial defect [Fig. 3] was identified with tibialis anterior herniation and bridged with an inlay ovine ECM patch, secured without excessive tension to avoid compartment constriction. The matrix patch was fixed with braided polyglactin[Fig. 4]. Post-operative recovery was uneventful. Guided by progressive physiotherapy, the patient resumed full sport within weeks and remained asymptomatic at follow‑up, consistent with outcomes reported for reinforced repairs [4,5]. No palpable defect on 3 weeks and 3 months follow up [Fig. 5].
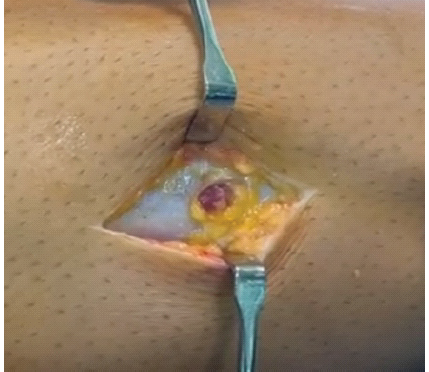
Figure 3: Intraoperative view of fascial defect with herniating tibialis
anterior muscle. Timing: Intraoperative immediately after fixation.
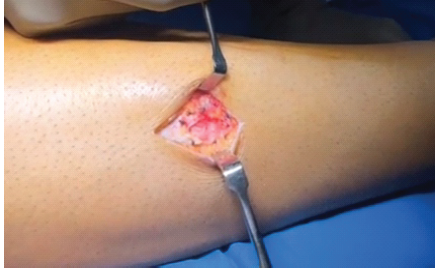
Figure 4: Intraoperative view of fascial defect and inlay ovine extracellular matrix patch. Intraoperative photograph demonstrating defect margins and
tension-free inlay patch reconstruction; Timing: Intraoperative immediately after fixation.

Figure 5: Post-operative scar with the foot in dorsiflexion, with no swelling, timing: 3 weeks post-operative.
Dynamic USG reliably demonstrates a focal fascial defect with outward bulging of muscle during stress maneuvers and is recommended as first‑line imaging [2]. MRI is valuable when USG is equivocal or to evaluate atypical presentations and exclude mimics (hematoma, arteriovenous malformation, neoplasm, or foreign bodies) [1,6]. Misdiagnosis is documented—for example, a retained foreign body initially labeled as a tibialis anterior herniation—underscoring the need for appropriate imaging in non‑classic cases [6,7]. Surgical options include longitudinal decompressive fasciotomy, primary fascial repair, and patch or mesh augmentation. Primary closure involves direct suturing of the fascial defect and may be considered in very small defects with minimal tension. However, in the anterior compartment, where fascia is inherently tight, primary closure can significantly increase intracompartmental pressure. This may compromise vascular perfusion and lead to compartment syndrome. In contrast, patch reconstruction using biological or synthetic materials allows for tension‑free repair. The ovine extracellular matrix acts as a scaffold for host tissue integration and remodeling. Advantages include reduced risk of compartment syndrome, preservation of muscle function, and lower recurrence rates. Disadvantages may include cost, potential for foreign body reaction (though minimal with biologics), and need for careful fixation. In the present case, primary closure was avoided due to the size of the defect (2 × 2 cm) and concern for increased compartmental pressure. A tension‑free ovine ECM patch provided adequate coverage while maintaining physiological compartment dynamics [1,4,8]. Primary repair may be suitable for very small, lax‑edge defects, but risks elevated intracompartmental pressures in the tight anterior compartment; acute compartment syndrome and muscle necrosis have been reported after tight approximation [3,8]. Reinforced closure with synthetic mesh (polyester/polypropylene) or biologic matrices spans the defect under minimal tension and has been associated with good functional results and low complication rates in small series and case reports [4,5,7]. Our use of an ovine ECM patch follows the same tension‑sparing principle. Ovine ECM is a bioscaffold comprising the decellularized propria submucosa isolated from sheep fore stomach (“rumen”) tissue [9]. They are used to regenerate tissue coverage over exposed structures and fill soft-tissue defects. Post-operative surveillance remains essential, along with a strengthening and graded return‑to‑sport protocol.
Tibialis anterior muscle herniation should be suspected in young, active patients with a dynamic anterolateral leg bulge and exertional pain. Dynamic USG confirms the diagnosis. When symptoms persist despite conservative care, tension‑free reconstruction using a patch or mesh is a pragmatic option to avoid the risks of tight primary closure, facilitating rapid and durable return to sport.
Avoid high‑tension primary closure of anterior‑compartment fascial defects. Tension‑free patch reconstruction (biologic or synthetic) reduces the risk of post-operative compartment syndrome and enables a reliable return to activity.
References
- 1. Nguyen JT, Nguyen JL, Wheatley MJ, Nguyen TA. Muscle hernias of the leg: A case report and comprehensive review of the literature. Can J Plast Surg 2013;21:243-7. [Google Scholar] [PubMed]
- 2. Sharma N, Kumar N, Verma R, Jhobta A. Tibialis anterior muscle hernia: A case of chronic, dull pain and swelling in leg diagnosed by dynamic ultrasonography. Pol J Radiol 2017;82:293-5. [Google Scholar] [PubMed]
- 3. Li YT, Hung CC, Pan RY, Hua SY. Compartment syndrome following directly repair of hernia of anterior tibialis. J Med Sci 2015;35:261-3. [Google Scholar] [PubMed]
- 4. Dönmez G, Evrenos MK, Cereb M, Karanfil Y, Doral MN. Double layer repair of tibialis anterior muscle hernia in a soccer player: A case report and review of the literature. Muscles Ligaments Tendons J 2015;5:331-4. [Google Scholar] [PubMed]
- 5. Al Rehaili HA, Al Ghamdi AM, Al Juhani WS. Tibialis anterior muscle herniation repaired with trevira tube: A surgical technique and review of literature. J Musculoskelet Surg Res 2019;3:357-62. [Google Scholar] [PubMed]
- 6. Sara L. Foreign body misdiagnosed as myofascial herniation of tibialis anterior muscle. J Orthop Physician Assist 2021;9:e20.00038. [Google Scholar] [PubMed]
- 7. Siliprandi L, Martini G, Chiarelli A, Mazzoleni F. Surgical repair of an anterior tibialis muscle hernia with Mersilene mesh. Plast Reconstr Surg 1993;91:154-7. [Google Scholar] [PubMed]
- 8. Masoumi A, Ramogida G. Tibialis anterior herniation – a rare clinical entity: A case report and review of the literature. J Can Chiropr Assoc 2020;64:88-91. [Google Scholar] [PubMed]
- 9. Lawlor J, Bosque BA, Frampton C, Young DA, Martyka P. Limb salvage via surgical soft-tissue reconstruction with ovine forestomach matrix grafts: A prospective study. Plast Reconstr Surg Glob Open 2024;12:e6406. [Google Scholar] [PubMed]
- 10. Almdahl SM, Due J Jr., Samdal FA. Compartment syndrome with muscle necrosis following repair of hernia of tibialis anterior. Case report. Acta Chir Scand 1987;153:695. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Management of Naja kaouthia Envenomation at a Quaternary Urban Medical Center: A Case Report
May 1, 2026 Management of Naja kaouthia Envenomation at a Quaternary Urban Medical Center: A Case Report March 1, 2026 Traumatic Tibialis Anterior Muscle Herniation with a Large Fascial Defect Managed by Prolene Mesh Repair: A Rare Case Report
March 1, 2026 Traumatic Tibialis Anterior Muscle Herniation with a Large Fascial Defect Managed by Prolene Mesh Repair: A Rare Case Report September 1, 2025 A Case of Volkmann’s Ischemic Contracture – A Case Report
September 1, 2025 A Case of Volkmann’s Ischemic Contracture – A Case Report October 1, 2024 Beyond Tradition: “Figure of 8” Casting for Gartland Type 1 and Type 2A Pediatric Supracondylar Fractures of Humerus: Video Technique
October 1, 2024 Beyond Tradition: “Figure of 8” Casting for Gartland Type 1 and Type 2A Pediatric Supracondylar Fractures of Humerus: Video Technique