
Persistent heel pain after minimally invasive Achilles tendon repair using PARS Achilles Midsubstance SpeedBridge™ may be caused by anchor-related irritation and can be successfully treated by surgical anchor excision when conservative management fails.
Dr. David Roche, Department of Foot and Ankle, Santy Orthopaedic Center, FIFA Medical Centre of Excellence, Jean Mermoz Private Hospital, Générale de Santé–Ramsay Group, Lyon, France. E-mail: dmmdroche@gmail.com
Abstract
Introduction: Minimally invasive repair of acute Achilles tendon rupture (ATR) using the percutaneous Achilles repair system (PARS) represents a reliable surgical option, with complication rates comparable to other techniques. Heel pain at the anchor insertion site has been reported as a post-operative complication but is rarely discussed in the literature. This report describes the successful treatment of persistent heel pain through surgical anchor excision.
Case Report: A 24-year-old man sustained a football-related injury to his left ankle in May 2023. He was referred to the emergency department with a clinical and ultrasonographic diagnosis of acute ATR. The patient underwent minimally invasive repair performed by an experienced foot and ankle surgeon using the PARS Achilles Midsubstance SpeedBridge™ Repair technique. Five months postoperatively, the patient reported pain localized to the lateral aspect of the heel near the anchor insertion site. Despite conservative management, symptoms persisted, leading to surgical excision of the anchor. At 1-year follow-up, the patient had fully recovered.
Conclusion: Persistent anchor-induced heel pain after minimally invasive repair of acute ATR using PARS Achilles Midsubstance SpeedBridge™ Repair can be successfully treated with surgical anchor excision, despite reports in the literature suggesting potential spontaneous resolution.
Keywords: Achilles tendon rupture, percutaneous Achilles repair system, heel pain, anchor irritation, surgical anchor removal.
Achilles tendon rupture (ATR) is one of the most common tendon injuries in the adult population and an increasingly common pathology [1]. Due to increasing activity levels in the population, there is a heightened need to ensure biomechanical function and performance of the posterior muscle chain following the ATR treatment. Despite numerous methods of treatment having been described to restore patients to their previous activities and avoid future disability, the ideal treatment for these lesions is still controversial [2,3]. If surgical treatment is considered, one of the 4 categories can be chosen: Open repair, percutaneous repair, mini-open repair, and augmentative repair [3]. Minimally invasive repair of acute ATR using the percutaneous Achilles repair system (PARS) represents a relevant surgical option compared with other techniques with no significant differences in rates of post-operative complications [2,4,5,6,7,8]. Heel pain at the anchor insertion site has been listed as a post-operative complication but is rarely discussed in the literature [9,10,11]. This is a case report of a young athlete with an ATR operated using PARS Achilles Midsubstance SpeedBridge™ Repair, which experienced persistent heel pain at the anchor insertion site starting at 5-month post-operative despite conservative treatment. This report describes the successful treatment of heel pain by surgical anchor excision and it seeks to highlight the existence of this complication when using the PARS Achilles Midsubstance SpeedBridge™. Furthermore, this paper aims to contribute to the literature by providing a reference when considering treatment options in similar cases and proposes avenues for future research regarding the incidence and causes of these complications. This paper was written according to SCARE guidelines [12].
A 24-year-old man suffered a football trauma in May 2023 on his left ankle. He felt a sudden pain and a popping sensation in a backward deceleration movement with no contact. The patient was referred to the emergency department with a clinical and ultrasonographic diagnosis of ATR but he chose to be operated on in a private clinic. On physical examination, he had a palpable defect about the Achilles tendon, with a hematoma on the rearfoot, he was unable to plantar flex his foot, he had a positive Thompson’s squeeze test on the left side, he had an asymmetric Matles test, and a positive test of Brunet-Guedj. This was the first reported injury to its left ankle. The patient was overweight with a body mass index of 25.4 with no other medical conditions. He was a non-smoker. The patient exercised regularly. He reported no recent use of fluoroquinolones or corticosteroids and denied any history of prior pain or significant medical conditions. He denied any family history of collagen disorder. With the patient’s consent and after the risks and benefits of the surgical intervention were explained, the patient was operated on by a surgeon experienced in foot and ankle surgery 3 days after injury using the technique described by Liechti et al. [10] With the patient in the prone position, a tourniquet on the superior thigh was placed. Perioperative antibiotic prophylaxis was initiated. The proximal stump of the ATR was identified on palpation. A 2 cm vertical incision on the medial side of the ATR was made. The PARS jig (Arthrex, Naples, Florida, USA) was placed in the incision and advanced proximally between the tendon and paratenon until it was stopped by the triceps surae complex muscle belly. The device was opened just enough to ensure that the proximal tendon is between the 2 arms of the PARS jig. FiberWires (Arthrex, Naples, Florida, USA) and FiberTape (Arthrex, Naples, Florida, USA) sutures are shuttled through the jig. The device was then slowly removed from the leg, pulling the suture through the incision site and within the paratenon. The strands were then passed through the distal Achilles stump using a Banana SutureLasso (Arthrex, Naples, Florida, USA). Then, the strands were secured into the calcaneus on the medial and lateral sides with a 4.75-mm SwiveLock (Arthrex, Naples, Florida, USA) on each side, whereas the foot was held in full plantar flexion [10]. The patient was discharged the same day with post-operative instructions, including the use of a long boot with heel wedges while remaining non-weight-bearing for the first 3 weeks. Pain control drugs and deep venous thrombosis prophylaxis were prescribed for 3 weeks. Physiotherapy was initiated after 3 weeks, with a gradual reduction in heel wedge height. The boot was discontinued at 6 weeks, with a single-heel wedge recommended thereafter until 2 months postoperatively. At the 1-month postoperative follow-up, the patient reported no significant pain and was fully weight-bearing with the assistance of a single crutch. The Thompson test was negative, with a slight equinus asymmetry. Surgical wounds were completely healed, with no tenderness on heel palpation. The patient was advised to continue the rehabilitation program. Five months after surgery, the patient began reporting pain localized to the lateral aspect of the heel, specifically near the anchor insertion site, with an Achilles’ tendon total rupture score (ATRS) of 27 [13]. The magnetic resonance imaging showed bone edema around the anchor sites (Fig. 1).
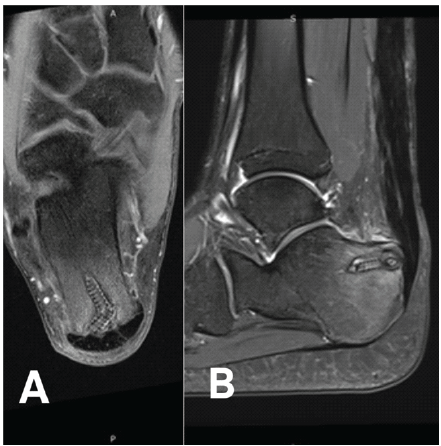
Figure 1: Magnetic resonance imaging (MRI) at 5 months after surgery of the left ankle in axial (a) and sagittal plane (b). MRI revealing mild calcaneal edema around the Bio SwiveLock (Arthrex) insertion site.
Despite conservative treatment for 2 months, the pain persisted, leading to the decision to perform surgical intervention. In December 2023, with the patient’s consent and after the risks and benefits of the surgical intervention were explained, the operation was performed through the use of a tourniquet (300 mmHg) on the proximal thigh with the patient under general anesthesia and antibioprophylaxis with the patient placed in the prone position. Re-exposure of the posterior approach was done, and the suture threads were located, leading to the anchor. The sutures and anchor were then removed. Inflammatory tissue at the tendon site was carefully cleaned, followed by extensive irrigation. The surgical site was closed in layers, and a dry dressing was applied. The patient was discharged the same day with post-operative instructions, including the use of a long boot with full-weight bearing for the first 2 weeks for skin healing. Pain control drugs for the 1st week were prescribed with no deep venous thrombosis prophylaxis. Rehabilitation was begun in post-operative week 2. At the 1-month post-operative follow-up, the patient reported a decrease in pain compared to the pre-operative level. He was able to fully bear weight, although with a subtle limp. The Thompson test was negative, with equinus symmetry, with delaying surgical scar healing. Three months postoperatively, the patient reported no pain and no limp. The Thompson test was negative with complete scar healing. One year after the last surgery, the patient has fully recovered, with no pain and no limp. He has returned to the same level of physical activity as before the ATR, with an ATRS of 82.
We report a case of a young athlete with an ATR operated using PARS Achilles Midsubstance SpeedBridge™ Repair, who experienced persistent heel pain at the anchor insertion site starting at 5-month post-operative, and despite conservative treatment, surgical anchor excision successfully treated heel pain. Heel pain at the anchor insertion site has been mentioned possibly due to the failure to bury each calcaneal anchor into the tunnels properly or it may also be correlated to the period of increased physical therapy intensity at an average of 12 weeks (9–15 weeks) postoperatively but the heel pain resolves by 20 weeks (range, 12–20 weeks) [7,8,9]. In this case, the anchor did not extend beyond the calcaneal cortex (Fig. 2), and the pain was not resolved with conservative treatment, which makes this case different from what is written so far in the literature Anchor-induced heel pain following minimally invasive repair of an acute ATR using the PARS Achilles Midsubstance SpeedBridge™ technique has thus far only been reported as a postoperative complication.Recent evidence by Peabody et al. comparing PARS and midsubstance SpeedBridge techniques reported comparable functional outcomes but highlighted that implant-related irritation, including cases requiring secondary anchor removal, may occur and deserves greater attention in the evaluation of post-operative complications [14]. Highlighting the existence of this complication proposes avenues for future research.
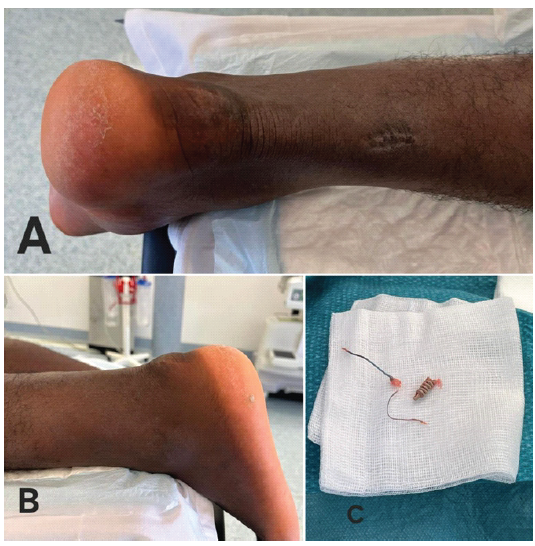
Figure 2: (a) Clinical photograph of the posterior aspect of the heel showing localized swelling and skin changes over the lateral calcaneal region corresponding to the anchor insertion site. (b) Lateral view of the heel demonstrating focal tenderness and prominence at the anchor location. (c) Intraoperative photograph showing the removed calcaneal anchor, which did not extend beyond the calcaneal cortex, along with the associated sutures following surgical excision.
Anchor-induced heel pain after minimally invasive repair of acute ATR using PARS Achilles Midsubstance SpeedBridge™ Repair can be treated surgically, even though the literature suggests that it resolves spontaneously. Studies are needed to understand the underlying mechanism and physiopathology, to clarify the causes, incidence, and risk factors.
Persistent heel pain after minimally invasive repair of acute Achilles tendon rupture using PARS Achilles Midsubstance SpeedBridge™ Repair, although uncommon, should not be overlooked. When pain persists despite adequate conservative management, implant-related irritation must be considered. This case highlights that surgical anchor excision can be an effective and definitive treatment, leading to symptom resolution and full functional recovery
References
- 1. Lemme NJ, Li NY, DeFroda SF, Kleiner J, Owens BD. Epidemiology of Achilles tendon ruptures in the United States: Athletic and nonathletic injuries from 2012 to 2016. Orthop J Sports Med. 2018 Nov 26;6(11):2325967118808238. doi: 10.1177/2325967118808238. PMID: 30505872; PMCID: PMC6259075. [Google Scholar] [PubMed] [CrossRef]
- 2. Macaluso B, Hassan CR, Swanson DR, Nazemi A, Zaverukha E, Paulus M, et al. Biomechanical comparison of krackow repair and percutaneous Achilles repair system for Achilles tendon rupture fixation: A cadaveric and finite element analysis study. Foot Ankle Orthop. 2022 Mar 31;7(1):24730114221088502. doi: 10.1177/24730114221088502. PMID: 35386585; PMCID: PMC8978323. [Google Scholar] [PubMed] [CrossRef]
- 3. Yang X, Meng H, Quan Q, Peng J, Lu S, Wang A. Management of acute Achilles tendon ruptures: A review. Bone Joint Res 2018;7:561-9. [Google Scholar] [PubMed]
- 4. Caolo KC, Eble SK, Rider C, Elliott AJ, Demetracopoulos CA, Deland JT, et al. Clinical outcomes and complications with open vs minimally invasive Achilles tendon repair. Foot Ankle Orthop. 2021 Nov 29;6(4):24730114211060063. doi: 10.1177/24730114211060063. PMID: 35097483; PMCID: PMC8646203. [Google Scholar] [PubMed] [CrossRef]
- 5. Lawson J, Tarapore R, Sequeira S, Imbergamo C, Tarka M, Guyton G, et al. Open and percutaneous approaches have similar biomechanical results for primary midsubstance Achilles tendon repair: A meta-analysis. Arthrosc Sports Med Rehabil 2024;6:100924. [Google Scholar] [PubMed]
- 6. Li Y, Jiang Q, Chen H, Xin H, He Q, Ruan D, Comparison of mini-open repair system and percutaneous repair for acute Achilles tendon rupture. BMC Musculoskelet Disord 2021;22:914. [Google Scholar] [PubMed]
- 7. Melinte MA, Nistor DV, De Souza Conde RA, Hernández RG, Wijaya P, Marvin K, et al. Mini-open versus percutaneous surgical repair for acute Achilles tendon rupture: A systematic review and meta-analysis. Int Orthop 2024;49:259-69. [Google Scholar] [PubMed]
- 8. Primo De Araujo JP, Mota Garcia Moreno MV, De Souza Guimarães J, Torres Gomes MJ, Marçal Vieira TE, Souza Jalil V. Comparison between the open and minimally invasive repair technique in acute Achilles tendon injuries. Sci J Foot Ankle 2018;12:265-70. [Google Scholar] [PubMed]
- 9. Clanton T, Stake IK, Bartush K, Jamieson MD. Minimally invasive Achilles repair techniques. Orthop Clin North Am 2020;51:391-402. [Google Scholar] [PubMed]
- 10. Liechti DJ, Moatshe G, Backus JD, Marchetti DC, Clanton TO. A percutaneous knotless technique for acute Achilles tendon ruptures. Arthrosc Tech 2018;7:e171-8. [Google Scholar] [PubMed]
- 11. McWilliam JR, Mackay G. The internal brace for midsubstance Achilles ruptures. Foot Ankle Int 2016;37:794-800. [Google Scholar] [PubMed]
- 12. Agha RA, Borrelli MR, Farwana R, Koshy K, Fowler AJ, Orgill DP, et al. The SCARE 2018 statement: Updating consensus surgical case report (SCARE) guidelines. Int J Surg 2018;60:132-6. [Google Scholar] [PubMed]
- 13. Buckinx F, Lecoq G, Bornheim S, Van Beveren J, Valcu A, Daniel C, et al. French translation and validation of the Achilles tendon total rupture score “ATRS”. Foot Ankle Surg 2020;26:662-8. [Google Scholar] [PubMed]
- 14. Peabody JJ, Hadley SM Jr., Bergman R, Westvold SJ, Olamigoke FO, Chang S, et al. Functional outcomes following minimally invasive Achilles rupture repair: A retrospective comparative study of PARS and midsubstance speedbridge techniques. J Orthop Surg 2025;20:390. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report December 1, 2025 A Prospective Case Series: Functional Outcomes after Calcaneal Tuberosity Partial Resection for Haglund’s Syndrome
December 1, 2025 A Prospective Case Series: Functional Outcomes after Calcaneal Tuberosity Partial Resection for Haglund’s Syndrome February 10, 2024 Heel Pain Management in Haglund’s Deformity Targeting Sural Nerve Branches under Ultrasound Guidance: Case Report
February 10, 2024 Heel Pain Management in Haglund’s Deformity Targeting Sural Nerve Branches under Ultrasound Guidance: Case Report February 10, 2024 Plantar Fasciitis with Chronic Baxter’s Neuropathy Causing Hindfoot Pain – A Case Report
February 10, 2024 Plantar Fasciitis with Chronic Baxter’s Neuropathy Causing Hindfoot Pain – A Case Report