
Musculoskeletal involvement is present in nearly one-third of patients with psoriasis and is strongly associated with longer disease duration, nail involvement, and higher cutaneous disease severity, underscoring the need for systematic orthopedic screening in routine care.
Dr. Preetam Singh Katroliya, Department of Dermatology, SRVS Medical College, Shivpuri, Madhya Pradesh, India. E-mail: preetam.k11@gmail.com
Abstract
Background: Psoriasis is a chronic inflammatory skin disorder frequently associated with extracutaneous manifestations, particularly involving the musculoskeletal system. Orthopedic involvement contributes substantially to morbidity but often remains underdiagnosed. This study aimed to evaluate the prevalence and pattern of musculoskeletal manifestations in patients with psoriasis and to assess their association with clinical disease characteristics.
Material and methods: A hospital-based cross-sectional study was conducted among 180 adult patients with clinically confirmed psoriasis attending a tertiary care center. Demographic details, disease duration, clinical type of psoriasis, nail involvement, and disease severity assessed by the psoriasis area and severity index (PASI) were recorded. All patients underwent a structured orthopedic evaluation for musculoskeletal manifestations. Laboratory parameters and radiological investigations were performed where indicated. Data were analyzed using appropriate statistical tests, with a P < 0.05 considered statistically significant.
Results: The mean age of participants was 42.6 ± 11.8 years, with males constituting 62.2% of the study population. Musculoskeletal involvement was observed in 54 patients (30.0%). Peripheral joint involvement was the most common pattern (17.8%), followed by axial (6.7%) and combined peripheral and axial involvement (5.6%). The knee (48.1%) and ankle (40.7%) were the most frequently affected joints. Enthesitis and dactylitis were present in 10.0% and 7.8% of patients, respectively. Musculoskeletal involvement was significantly associated with longer disease duration (≥5 years), nail involvement, and moderate to severe psoriasis (PASI ≥10) (P < 0.05). Elevated erythrocyte sedimentation rate and C-reactive protein were noted in 59.3% and 51.9% of affected patients, respectively, while 44.4% showed radiographic abnormalities.
Conclusion: Musculoskeletal manifestations affect a substantial proportion of patients with psoriasis and are significantly associated with disease severity, duration, and nail involvement. Routine screening for orthopedic involvement should be integrated into the clinical evaluation of patients with psoriasis to enable early diagnosis and appropriate management.
Keywords: Psoriasis, musculoskeletal involvement, psoriatic arthritis, orthopedic manifestations, cross-sectional study.
Psoriasis is a chronic, immune-mediated inflammatory skin disease with substantial effects on physical health and quality of life. Beyond cutaneous involvement, psoriasis is increasingly recognized as part of a broader “psoriatic disease” spectrum, in which systemic inflammation contributes to clinically important comorbidities, including musculoskeletal disease. In contemporary syntheses, plaque psoriasis is frequently associated with psoriatic arthritis and other comorbidities that together amplify overall morbidity [1].
Musculoskeletal involvement represents a major extracutaneous domain of psoriatic disease and may affect peripheral joints, entheses, digits (dactylitis), and the axial skeleton. Current evidence supports that a meaningful proportion of individuals with psoriasis develop inflammatory musculoskeletal disease, and expert overviews emphasize that joints and entheses are central target tissues within psoriatic disease [2].
Across observational studies, pooled estimates indicate that psoriatic arthritis occurs in approximately one-fifth of patients with psoriasis overall, with variation by geography, study design, and classification approach; in meta-analytic work that included large psoriasis cohorts, the pooled proportion of psoriatic arthritis among patients with psoriasis was ~19.7%, and estimates were higher in studies applying formal classification criteria [3]. In dermatology-facing reviews, prevalence ranges extending into higher values are also described, and a clinically relevant fraction of psoriatic arthritis remains unrecognized among patients with psoriasis, reinforcing the need for orthopedic-focused assessment in routine care [4].
Identifying patients at higher risk of musculoskeletal involvement is important for early evaluation. Dermatologic features have practical value for risk stratification; synthesis of epidemiological and mechanistic data highlights psoriasis severity and nail disease as among the most consistent skin-related predictors linked to future psoriatic arthritis [5].
Given that musculoskeletal involvement in psoriasis may be underrecognized and can occur across different stages of disease, early identification remains a clinical challenge. Moreover, data on the burden and pattern of orthopedic manifestations in Indian hospital-based settings are limited. Therefore, this cross-sectional study was conducted to quantify the prevalence and spectrum of musculoskeletal involvement among patients with psoriasis and to evaluate its association with key clinical characteristics, including disease duration, cutaneous severity, and nail involvement, to support earlier detection and improved clinical outcomes.
Study design and setting
This was a hospital-based, cross-sectional observational study conducted in a tertiary care teaching hospital in India. The study was carried out over a period of 18 months.
Ethical considerations
The study protocol was reviewed and approved by the Institutional Ethics Committee (No. 161/IEC/GMC/2025, 09th July 2025). All procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment.
Study population
Adult patients with a confirmed diagnosis of psoriasis attending the dermatology outpatient clinic during the study period were screened for eligibility. Psoriasis was diagnosed clinically by a consultant dermatologist, with histopathological confirmation obtained when the diagnosis was uncertain.
Sample size
The sample size was calculated assuming a prevalence of musculoskeletal involvement in psoriasis of 30%, based on previously reported estimates [6], with a 95% confidence level and an absolute precision of 7%. Using the standard single-proportion formula, the minimum required sample size was 165. To account for possible incomplete data, a total of 180 patients were included in the final analysis.
Inclusion criteria
- Age ≥18 years
- Clinically confirmed diagnosis of psoriasis of any type
- Disease duration of at least 6 months
- Willingness to provide written informed consent
Exclusion criteria
- Known diagnosis of inflammatory arthritis unrelated to psoriasis (e.g., rheumatoid arthritis, ankylosing spondylitis)
- History of major joint trauma or orthopedic surgery within the past year
- Presence of chronic systemic illnesses affecting the musculoskeletal system (e.g., chronic kidney disease–mineral bone disorder, advanced liver disease)
- Current pregnancy or lactation
Data collection
After obtaining informed consent, eligible participants underwent a detailed clinical evaluation using a structured pro forma. Demographic data (age, sex), disease-related variables (type of psoriasis, duration of disease, age at onset), and treatment history were recorded. Severity of cutaneous disease was assessed using the psoriasis area and severity index (PASI) and body surface area involvement. Nail involvement was documented based on clinical examination.
Orthopedic assessment
All participants were evaluated for musculoskeletal manifestations by an orthopedic specialist blinded to PASI scores. Assessment included:
- History of joint pain, stiffness, swelling, and functional limitation
- Pattern of joint involvement (peripheral, axial, or combined)
- Presence of enthesitis, dactylitis, or deformities
- Duration and diurnal variation of musculoskeletal symptoms.
A comprehensive musculoskeletal examination was performed, including inspection, palpation, range of motion testing, and assessment for tenderness and swelling.
Radiological evaluation
Plain radiographs of symptomatic joints were obtained where clinically indicated. Radiographic findings were assessed for joint space narrowing, erosions, osteophyte formation, periosteal reaction, and sacroiliac involvement. Imaging interpretation was performed by a radiologist blinded to clinical details.
Laboratory investigations
Baseline laboratory investigations included erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Rheumatoid factor and anti-cyclic citrullinated peptide antibodies were tested in selected cases to exclude alternative inflammatory arthritides when clinically indicated.
Outcome measures
The primary outcome was the prevalence of orthopedic manifestations among patients with psoriasis. Secondary outcomes included the pattern of joint involvement and the association between musculoskeletal manifestations and disease duration, severity of psoriasis, and nail involvement.
Statistical analysis
Data were entered into Microsoft Excel and analyzed using SPSS software (version 26.0). Continuous variables were expressed as mean ± standard deviation. Categorical variables were presented as frequencies and percentages. Associations between categorical variables were assessed using the Chi-square test. Continuous variables were compared using the independent t-test or Mann–Whitney U test based on data distribution. A P < 0.05 was considered statistically significant.
A total of 180 patients with psoriasis were included in the final analysis. The mean age of the study population was 42.6 ± 11.8 years, with a male predominance (62.2%). The majority of patients had plaque-type psoriasis (81.1%), and the median duration of disease was 6.0 years. Nail involvement was observed in 41.1% of cases. Nearly half of the patients (45.6%) had moderate to severe disease, defined by a PASI score ≥10 (Table 1).
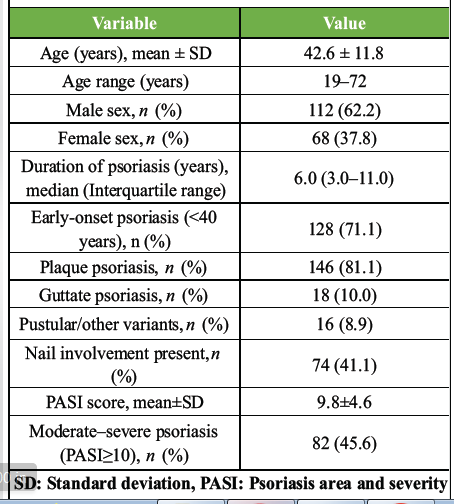
Table 1: Baseline demographic and clinical characteristics of the study population (n=180)
Musculoskeletal involvement was identified in 54 patients (30.0%). Among these, peripheral joint involvement was the most common pattern (17.8%), followed by axial involvement (6.7%) and combined peripheral and axial disease (5.6%). Features suggestive of inflammatory musculoskeletal disease included morning stiffness lasting more than 30 min (16.1%), enthesitis (10.0%), and dactylitis (7.8%) (Table 2).
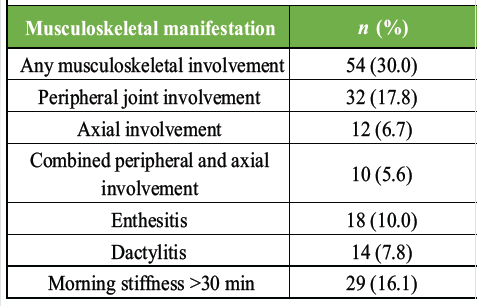
Table 2: Prevalence and pattern of musculoskeletal involvement among patients with psoriasis
Analysis of joint distribution among patients with musculoskeletal manifestations showed that the knee joint was most frequently affected (48.1%), followed by the ankle (40.7%) and wrist (33.3%). Involvement of the small joints of the hands was noted in 29.6% of patients, while sacroiliac joint involvement was observed in 22.2% (Fig. 1).
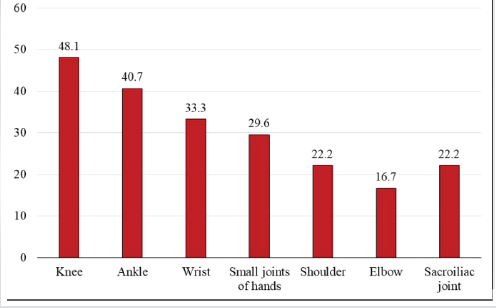
Figure 1. Distribution of joints involved in patients (n=54).
Patients with musculoskeletal involvement were significantly older compared to those without involvement (45.3 ± 10.9 years vs. 41.4 ± 12.1 years; P = 0.041). A significantly higher proportion of patients with musculoskeletal manifestations had a disease duration of 5 years or more (70.4% vs. 44.4%; P = 0.002). Nail involvement was also more frequent in patients with musculoskeletal manifestations (63.0% vs. 31.7%; P < 0.001). Similarly, moderate to severe psoriasis (PASI ≥ 10) was significantly associated with musculoskeletal involvement (66.7% vs. 36.5%; P < 0.001). There was no statistically significant association between sex and musculoskeletal involvement (P = 0.412) (Table 3).
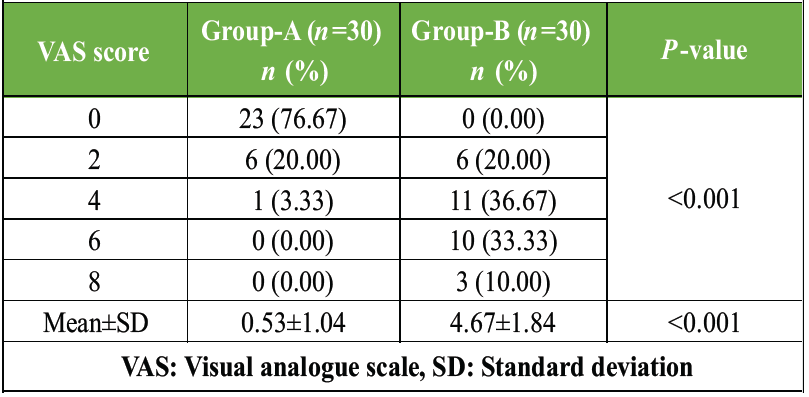 Table 3: Comparison of post-operative pain using VAS score in the immediate post-operative period between group-A and group-B
Table 3: Comparison of post-operative pain using VAS score in the immediate post-operative period between group-A and group-B
Among patients with musculoskeletal involvement, laboratory evaluation showed elevated ESR in 59.3% and elevated CRP in 51.9% of cases. Radiographic abnormalities were detected in 44.4% of these patients. The most common radiological findings included joint space narrowing (25.9%) and erosive changes (18.5%), while sacroiliitis was identified in 14.8% of patients (Table 4).
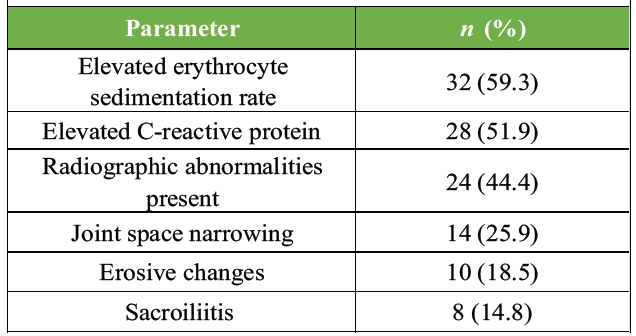
Table 4: Laboratory and radiological findings in patients with musculoskeletal involvement (n=54)
Fig. 2 radiograph shows classic psoriatic arthritis changes (highlighted by arrows), including pencil-in-cup deformities, osteolysis, joint space narrowing, and new bone formation.

Figure 2. Radiograph showing classic psoriatic arthritis changes (highlighted by arrows).
In this cross-sectional study of 180 patients with psoriasis, musculoskeletal involvement was identified in 30.0% of participants, with peripheral joint disease forming the predominant pattern. This estimate aligns with widely cited ranges, suggesting that a substantial minority of patients with psoriasis develop inflammatory musculoskeletal disease, and reinforces the concept that joint and entheseal involvement represents a frequent extracutaneous domain of psoriatic disease [7]. In addition, musculoskeletal symptoms may be common even in patients without a formal diagnosis of psoriatic arthritis; a large US claims-based retrospective analysis demonstrated high rates of musculoskeletal symptoms among patients with newly diagnosed psoriasis over longitudinal follow-up, highlighting the clinical burden of musculoskeletal complaints in dermatology populations [8].
Peripheral joint involvement was most frequent in our cohort, and the knee and ankle were commonly affected joints. This distribution is consistent with the heterogeneous articular expression of psoriatic disease encountered in routine practice, where large-joint and peripheral patterns are regularly observed. Importantly, our study also documented axial involvement in a subset of patients and radiographic sacroiliitis in 14.8% of those with musculoskeletal manifestations. Contemporary reviews emphasize that axial psoriatic arthritis remains challenging to define due to variable terminology, overlap with axial spondyloarthritis, and the absence of universally accepted classification criteria, which may contribute to under-recognition of axial disease across clinical settings [9].
A key observation in our analysis was the significant association between musculoskeletal involvement and psoriasis duration ≥5 years, nail involvement, and moderate–severe cutaneous disease (PASI ≥ 10). The relationship between greater skin disease burden and subsequent or concurrent inflammatory arthritis has been supported in population-based prospective work, where higher skin involvement/severity was associated with increased risk of developing psoriatic arthritis; notably, PASI > 20 (vs. <10) has been linked with substantially higher hazard for psoriatic arthritis in cohort data [10]. The strong association with nail involvement in our study is clinically relevant, as nail disease in psoriatic arthritis populations has been associated with worse overall disease activity and impaired quality of life and work productivity in registry analyses, supporting the value of careful nail assessment during musculoskeletal screening [11].
Inflammatory markers were elevated in approximately half of affected patients (ESR 59.3%, CRP 51.9%), and radiographic abnormalities were present in 44.4%. While elevated acute-phase reactants may support inflammatory disease activity, they are not uniformly abnormal in psoriatic arthritis, and the absence of a specific biomarker remains a recognized diagnostic challenge [12]. Structural joint damage is clinically meaningful because it may accumulate early and is strongly linked to disability; a methodological review of structural damage progression highlights that conventional radiography remains the standard approach for damage assessment, and summarizes evidence that a meaningful proportion of patients demonstrate structural damage relatively early in the disease course [13].
These findings collectively underscore the importance of systematic screening and early referral pathways for musculoskeletal disease in psoriasis clinics. Published work notes that a proportion of psoriatic arthritis cases remain undiagnosed in dermatology settings, and screening instruments such as the psoriasis epidemiology screening tool have been advocated to support early recognition and triage [12,14]. The clinical consequences of delayed diagnosis are substantial; population-based research indicates that diagnostic delay of even 6–12 months is associated with poorer outcomes and greater joint damage, emphasizing the need for timely detection [15]. In addition to clinical assessment, evolving imaging strategies can aid early detection and characterization of disease domains; recent imaging-focused reviews describe how ultrasound and magnetic resonance imaging (MRI) complement radiographs by improving sensitivity for inflammatory and structural lesions, which may be particularly valuable in early or subclinical disease [16].
The present study has several strengths. It includes a well-defined cohort of 180 patients with clinically confirmed psoriasis and provides a systematic assessment of musculoskeletal manifestations using a structured pro forma and standardized clinical examination. The use of PASI scoring allowed objective stratification of disease severity, and the blinded orthopedic evaluation minimized observer bias. In addition, the study comprehensively reports the pattern of joint involvement, specific clinical features such as enthesitis and dactylitis, and supportive laboratory (ESR, CRP) and radiographic findings, thereby offering a clinically relevant overview of orthopedic manifestations in routine practice.
However, certain limitations should be considered. The cross-sectional design limits the ability to establish temporal or causal relationships between psoriasis characteristics (such as duration ≥5 years, PASI ≥ 10, and nail involvement) and musculoskeletal manifestations, as observed in Table 3. Being a hospital-based study conducted at a tertiary care center, there is a possibility of referral bias, which may overestimate the prevalence (30.0%) and severity of musculoskeletal involvement. Radiological evaluation was performed only in symptomatic patients, which may have underestimated subclinical joint disease and influenced the proportion of radiographic abnormalities as reported in Table 4. Advanced imaging modalities such as MRI or musculoskeletal ultrasound were not utilized, further limiting early detection of inflammatory changes. In addition, formal classification criteria for psoriatic arthritis were not uniformly applied, and diagnosis was based on clinical and supportive findings, which may affect comparability with epidemiological studies.
This cross-sectional study demonstrates that musculoskeletal involvement is present in nearly one-third of patients with psoriasis, with peripheral joint disease being the most frequent manifestation. Longer disease duration, higher cutaneous disease severity, and the presence of nail involvement were significantly associated with orthopedic manifestations, highlighting the close interplay between skin and musculoskeletal disease. The findings underscore the importance of routine orthopedic evaluation in patients with psoriasis, particularly in those with long-standing or moderate to severe disease, to facilitate early identification and timely management of musculoskeletal involvement and potentially prevent long-term functional impairment.
Psoriasis should be approached as a multisystem inflammatory disease rather than a purely cutaneous disorder, as a substantial proportion of patients have clinically significant but often underrecognized musculoskeletal involvement. Peripheral joint disease, particularly involving the knee and ankle, is the most frequent pattern, while axial disease and enthesitis are also clinically relevant. Patients with long-standing psoriasis, nail changes, and moderate to severe skin involvement represent a high-risk group for inflammatory musculoskeletal manifestations. Incorporating routine musculoskeletal assessment and early referral pathways into psoriasis management can facilitate timely diagnosis and intervention, potentially reducing long-term joint damage and functional impairment.
References
- 1. Armstrong AW, Blauvelt A, Callis Duffin K, Huang YH, Savage LJ, Guo L, et al. Psoriasis. Nat Rev Dis Primers 2025;11:45. [Google Scholar] [PubMed]
- 2. Mrowietz U, Lauffer F, Sondermann W, Gerdes S, Sewerin P. Psoriasis as a systemic disease. Dtsch Arztebl Int 2024;121:467-72. [Google Scholar] [PubMed]
- 3. Alinaghi F, Calov M, Kristensen LE, Gladman DD, Coates LC, Jullien D, et al. Prevalence of psoriatic arthritis in patients with psoriasis: A systematic review and meta-analysis of observational and clinical studies. J Am Acad Dermatol 2019;80:251-65.e19. [Google Scholar] [PubMed]
- 4. Perez-Chada LM, Elman S, Villa-Ruiz C, Armstrong AW, Gottlieb AB, Merola JF. Psoriatic arthritis: A comprehensive review for the dermatologist part I: Epidemiology, comorbidities, pathogenesis, and diagnosis. J Am Acad Dermatol 2025;92:969-82. [Google Scholar] [PubMed]
- 5. Fratton Z, Giovannini I, Zabotti A, Errichetti E. Skin and nail predictors of psoriatic arthritis development: A holistic overview integrating epidemiological and physiopathological data. J Clin Med 2024;13:6880. [Google Scholar] [PubMed]
- 6. Ocampo DV, Gladman D. Psoriatic arthritis. F1000Res 2019;8:F1000 Faculty Rev-1665. doi:10.12688/f1000research.19144.1. [Google Scholar] [PubMed] [CrossRef]
- 7. Hioki T, Komine M, Ohtsuki M. Diagnosis and intervention in early psoriatic arthritis. J Clin Med 2022;11:2051. [Google Scholar] [PubMed]
- 8. Merola JF, Patil D, Egana A, Steffens A, Webb NS, Gottlieb AB. Prevalence of musculoskeletal symptoms in patients with psoriasis and predictors associated with the development of psoriatic arthritis: Retrospective analysis of a US claims database. Dermatol Ther (Heidelb) 2023;13:2635-48. [Google Scholar] [PubMed]
- 9. Michelena X, López-Medina C, De Miguel E, Moreno-Ramos MJ, Queiro R, Marzo-Ortega H, et al. How are we addressing axial psoriatic arthritis in clinical practice? Rheumatol Ther 2024;11:1441-56. [Google Scholar] [PubMed]
- 10. Ogdie A, Shin DB, Love TJ, Gelfand JM. Body surface area affected by psoriasis and the risk for psoriatic arthritis: A prospective population-based cohort study. Rheumatology (Oxford) 2022;61:1877-84. [Google Scholar] [PubMed]
- 11. Mease PJ, Liu M, Rebello S, McLean RR, Dube B, Glynn M, et al. Association of nail psoriasis with disease activity measures and impact in psoriatic arthritis: Data from the corrona psoriatic arthritis/spondyloarthritis registry. J Rheumatol 2021;48:520-6. [Google Scholar] [PubMed]
- 12. Rida MA, Chandran V. Challenges in the clinical diagnosis of psoriatic arthritis. Clin Immunol 2020;214:108390. [Google Scholar] [PubMed]
- 13. Van Der Heijde D, Gladman DD, Kavanaugh A, Mease PJ. Assessing structural damage progression in psoriatic arthritis and its role as an outcome in research. Arthritis Res Ther 2020;22:18. [Google Scholar] [PubMed]
- 14. Chang J, Litvinov IV, Ly C, Netchiporouk E, Tsoukas A, Thuraisingam T, et al. Utilization of the psoriasis epidemiology screening tool (PEST): A risk stratification strategy for early referral of psoriatic arthritis patients to minimize irreversible erosive joint damage. J Cutan Med Surg 2022;26:600-3. [Google Scholar] [PubMed]
- 15. Karmacharya P, Wright K, Achenbach SJ, Bekele D, Crowson CS, Ogdie A, et al. Diagnostic delay in psoriatic arthritis: A population-based study. J Rheumatol 2021;48:1410-6. [Google Scholar] [PubMed]
- 16. Jin Y, Cheng IT, Wu D, Yan X, Lau SL, Wong NS, et al. Imaging in psoriatic arthritis: Established methods and emerging techniques. Ther Adv Musculoskelet Dis 2024;16:1759720X241288060 . [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2024 Tibial Dysplasia in Neurofibromatosis-1: A Rare Case Report and Review of Literature
February 10, 2024 Tibial Dysplasia in Neurofibromatosis-1: A Rare Case Report and Review of Literature May 1, 2026 Single-Stage Management of Anterior Cruciate Ligament Tear with Dual Menisci Bony Root Avulsion: A Rare Case Report and Review of Literature
May 1, 2026 Single-Stage Management of Anterior Cruciate Ligament Tear with Dual Menisci Bony Root Avulsion: A Rare Case Report and Review of Literature November 23, 2017 Unusual Presentation of Spinal Gout: 2 Cases Report and Literature Review
November 23, 2017 Unusual Presentation of Spinal Gout: 2 Cases Report and Literature Review September 8, 2018 Type III Monteggia Equivalent Lesion with Ipsilateral Fracture Lateral Condyle of Humerus in a Four-year-old Child: A Case Report and Literature Review
September 8, 2018 Type III Monteggia Equivalent Lesion with Ipsilateral Fracture Lateral Condyle of Humerus in a Four-year-old Child: A Case Report and Literature Review