
Achieving positive medial cortical reduction in unstable intertrochanteric fractures significantly improves fracture stability, functional recovery, and reduces implant-related complications.
Dr. Parimal Vairagade, Department of Orthopaedic Surgery, NKP Salve Institute of Medical Sciences, Nagpur - 440019, Maharashtra, India. E-mail: pvairagade01@gmail.com
Abstract
Introduction: Intertrochanteric fractures, especially unstable fractures, are common among the elderly and present significant challenges in terms of fracture healing and post-operative recovery. The medial cortex of the femur plays a crucial role in maintaining fracture stability and promoting healing. This study explores the impact of medial cortical reduction on the outcomes of fixation in unstable intertrochanteric fractures.
Objectives: To assess the effect of medial cortical reduction on fracture healing, functional recovery, and implant failure in patients with unstable intertrochanteric fractures.
Materials and Methods: A prospective observational study was conducted on 50 patients with unstable intertrochanteric fractures. Patients were categorized into three groups based on the quality of medial cortical reduction achieved: positive, neutral, or negative. Functional recovery was evaluated using the walking ability score (WAS) at 4, 6, and 12 weeks post-surgery.
Results: Patients with positive medial cortical reduction showed significantly higher WAS scores at all follow-up points, indicating better functional recovery. The complication rate was 10%, with implant failure observed in 4% of cases. The positive reduction group had the best outcomes in terms of healing and functional recovery.
Conclusion: Positive medial cortical reduction is associated with superior functional recovery, reduced implant failure, and better overall outcomes in unstable intertrochanteric fractures. Achieving optimal medial cortical reduction should be prioritized during surgical fixation for these fractures.
Keywords: Medial cortical reduction, unstable intertrochanteric fractures, fracture healing, functional recovery, implant failure, walking ability score, proximal femoral nailing, dynamic hip screw, surgical fixation, osteoporotic bone, hip fractures, orthopedic surgery, femoral fracture stability, biomechanics.
Intertrochanteric fractures are among the most frequent hip fractures in the elderly, representing a leading cause of morbidity, loss of independence, and perioperative mortality in older adults worldwide. These injuries typically arise from low-energy mechanisms such as ground-level falls, with their incidence expected to rise substantially as the global population ages [1,2]. The femoral medial cortex, which is the posteromedial bony buttress of the proximal femur, is a critical determinant of fracture stability, as it resists compressive loads during weight-bearing and maintains the spatial relationship between the femoral head and shaft [3,4].
Unstable intertrochanteric fracture patterns (AO/Orthopaedic Trauma Association [OTA] 31-A2 and 31-A3) are defined by disruption of the medial cortical column, resulting in compromised intrinsic stability that challenges both reduction and fixation [5,6]. When medial cortical continuity cannot be restored, excessive stress is transferred to the implant, predisposing to catastrophic complications, including screw cut-out, varus collapse, non-union, and mechanical failure [7,8]. Despite widespread adoption of intramedullary cephalomedullary nails, implant-related failure rates remain non-negligible in cases where anatomic reduction is suboptimal [9,10]. The quality of medial cortical reduction, classified as positive, neutral, or negative based on the degree of posteromedial cortical contact restored intraoperatively, has therefore emerged as a key modifiable determinant of surgical outcome. However, the precise functional impact across reduction categories requires further characterization.
Several national and international studies have examined predictors of fixation failure in unstable intertrochanteric fractures [11-18], yet comparisons across medial cortical reduction categories, particularly with respect to serial functional recovery, remain underreported in prospective cohorts. The present study was therefore designed to prospectively assess the effect of medial cortical reduction quality (positive, neutral, or negative) on fracture healing, functional recovery measured by the walking ability score (WAS) at 4, 6, and 12 weeks postoperatively, and implant-related complication rates in patients with unstable intertrochanteric fractures treated at a tertiary trauma center.
Study design
This was a prospective observational study conducted at a tertiary healthcare center. The study aimed to assess the impact of medial cortical reduction on the outcomes of fixation in patients with unstable intertrochanteric fractures by calculating WAS at 4, 6, and 12 weeks. The study included patients from January 2025 to December 2025, and data were collected from the outpatient and inpatient departments of the hospital.
Study population
The study included 50 patients who met the following criteria:
Sample size and sampling technique
All the patients presented to tertiary healthcare centers with unstable intertrochanteric femur fractures. The Effect of Positive Medial Cortical Support in Reduction of Pertrochanteric Fractures with Posteromedial Wall Defect Using a Dynamic Hip Screw
Myung Rae Cho 1, Jae Hyuk Lee 1, Jai Bum Kwon 1, Jung Suk Do 1, Seung Bum Chae 1, Won-Kee Choi 1
WAS post-operative according to the grade of medial cortical support.
Mean: 6.18.
Standard deviation: 1.33.
Formula for sampling size: n = z2(1-α/2)XSD2/L2
Where Z2(1-α/2) = is the standard normal variate at (1-α/2) level.
SD is the standard deviation.
L=Precision = 0.5.
Required sample size = 50.
Inclusion criteria
-
- Patients aged ≥18 years
- Patients diagnosed with unstable intertrochanteric fractures classified as 31A2.2 or 31A2.3 according to the AO/OTA classification
- Willingness to participate in the study and provide informed consent.
Exclusion criteria
-
- Stable intertrochanteric fractures (classified as AO31.A1)
- Ipsilateral fractures or polytrauma
- Patients with severe comorbidities that would affect post-operative recovery
- Patients unwilling to follow-up or provide informed consent.
Patients were selected consecutively from the hospital’s trauma registry and fracture clinic based on the inclusion criteria. The study was approved by the hospital’s ethics committee, and written informed consent was obtained from all participants.
Pre-operative assessment
All patients underwent a thorough clinical evaluation, including:
- Detailed history: Mechanism of injury, pre-existing comorbidities (such as osteoporosis, diabetes, or hypertension), and pre-injury functional status.
- Physical examination: Including inspection, palpation, and range of motion assessment of the affected hip.
Radiological evaluation
-
- Standard anteroposterior and lateral X-rays of the hip joint to confirm fracture pattern and classification
- Computed tomography scans were performed in selected cases for complex fractures with comminution or extension into the subtrochanteric region
- Bone mineral density (BMD) was assessed for patients with a history of osteoporosis or significant risk factors.
Surgical technique
All patients underwent surgical fixation of their fractures using one of the following methods, depending on the fracture pattern and the surgeon’s preference:
- Proximal femoral nailing (PFN): This was the most commonly used surgical technique, chosen for its biomechanical advantages, especially in unstable fractures.
- Long PFN (Long PFN): Used in cases where there was significant subtrochanteric extension.
- Dynamic hip screw (DHS): Used in patients with more stable fractures or in cases where PFN was not deemed appropriate.
Reduction technique
- The reduction of the fracture was performed under fluoroscopic guidance, with the goal of achieving optimal alignment and restoration of the medial cortex
- Medial cortical reduction was classified as follows [19]:
- Positive reduction: Full restoration of the medial cortex, ensuring proper alignment and load transmission
- Neutral reduction: Partial restoration of the medial cortex with some loss of alignment but no significant instability
- Negative reduction: Significant misalignment or failure to restore the medial cortex, leading to compromised fracture stability.
The fractures were stabilized with cephalomedullary nails, or in some cases, DHSs or locking plates, based on the surgeon’s assessment.
Post-operative management
Post-operative care followed standard protocols, including:
- Pain management: A multimodal analgesia protocol, including non-steroidal anti-inflammatory drugs, opioids for breakthrough pain, and regional nerve blocks if necessary.
- Early mobilization: Patients were encouraged to start weight-bearing as per the fracture stability and type of fixation.
- Antibiotic prophylaxis: Prophylactic antibiotics were administered perioperatively to prevent surgical site infections.
- Thromboembolic prophylaxis: Low-molecular-weight heparin was used to prevent deep vein thrombosis.
Surgery performed on study subjects (Fig. 1)
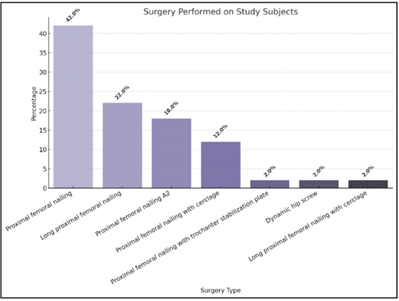
Figure 1: Surgery performed on study subjects.
Demographics
- Age distribution: The study cohort had a mean age of 69.4 standard deviation, with 52% of patients aged ≥70 years, 34% aged 50–70 years, and 14% aged <50 years (Table 1 and Fig. 2).
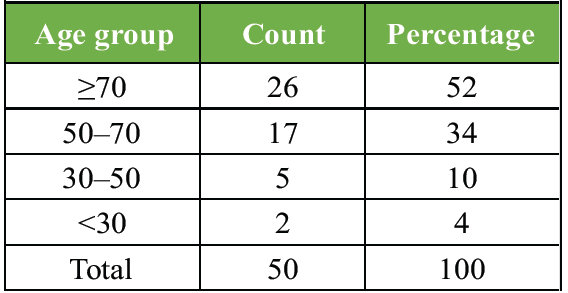
Table 1: Age group distribution of study subjects
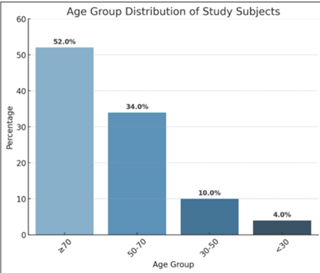
Figure 2: Age group distribution of study subjects.
- Sex distribution: Males constituted 57.99% of the cohort, with females making up 42% (Table 2 and Fig. 3).
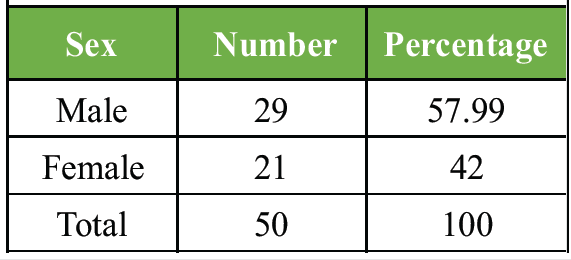
Table 2: Sex distribution in study subjects
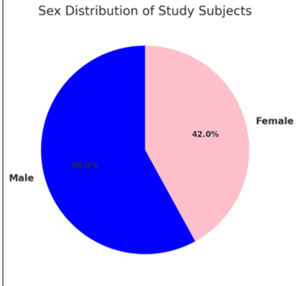
Figure 3: Sex distribution in study subjects.
Fracture classification
The majority of fractures were classified as AO31.A2.2 (34%), followed by AO31.A1.2 (18%) and AO31.A3.2 (16%) (Table 3 and Fig. 4).
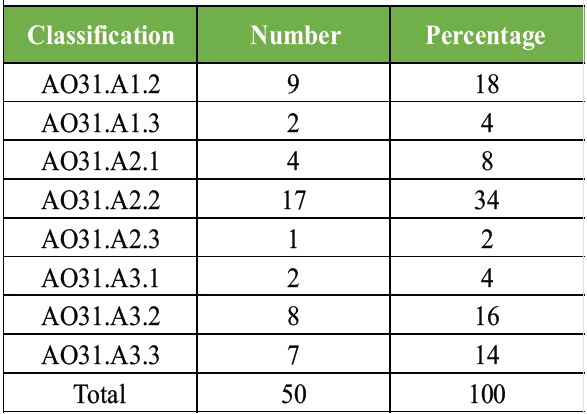
Table 3: Distribution of study subjects as per classification of fracture
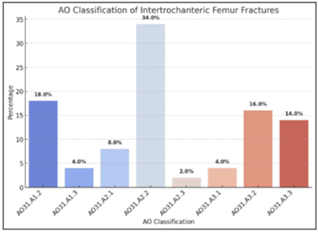
Figure 4: Distribution of study subjects as per the classification of fracture.
Surgical procedures
PFN was the most common surgery (42%).
Long PFN was used in 22%, and PFN antirotation II (PFNA2) in 18% (Table 4).
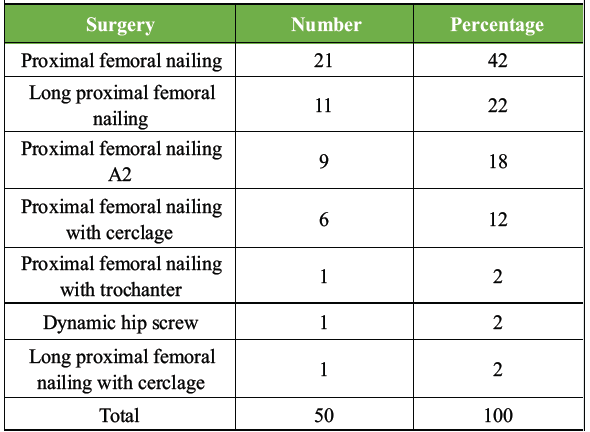
Table 4: Distribution of study subjects as per surgery performed
Other techniques, including PFN with cerclage wiring (12%) and DHS (2%), were utilized in specific cases.
Reduction type
- Positive medial cortical reduction: Achieved in 38% of patients
- Neutral medial cortical reduction: Achieved in 38%
- Negative medial cortical reduction: Achieved in 24%.
(Tables 5 and 6, Fig. 5).
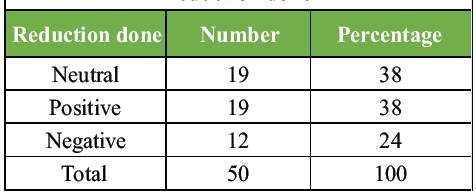
Table 5: Distribution of study subjects as per reduction done
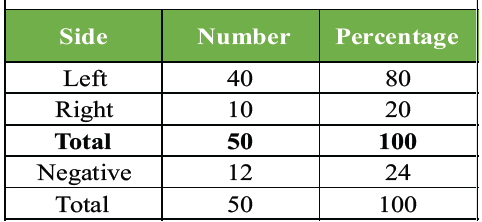
Table 6: Distribution of study subjects as per side involved in fracture
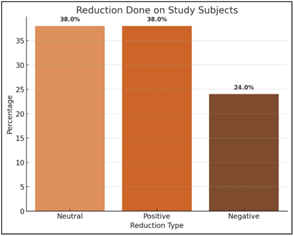
Figure 5: Reduction done on study subjects.
Complications
The complication rate was 10%, with implant failure occurring in 4% of patients.
Functional recovery (WAS)
- Positive medial cortical reduction: Patients with positive reduction showed the highest WAS scores at all follow-up points (4 weeks: 14.05 ± 1.87, 6 weeks: 17.0 ± 1.86, and 12 weeks: 19.42 ± 1.61).
- Neutral medial cortical reduction: Moderate improvement in WAS scores (4 weeks: 13.0 ± 1.45, 6 weeks: 16.37 ± 1.8, and 12 weeks: 19.21 ± 1.87).
- Negative medial cortical reduction: The lowest WAS scores (4 weeks: 9.67 ± 1.56, 6 weeks: 12.0 ± 1.54, and 12 weeks: 14.33 ± 1.92) (Tables 7 and 8, Fig. 6 & 7).
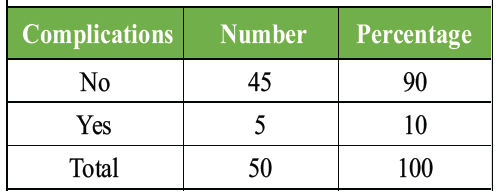
Table 7: Distribution of study subjects as per the presence of complications
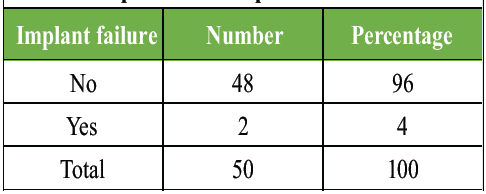
Table 8: Distribution of study subjects as per the presence of implant failure
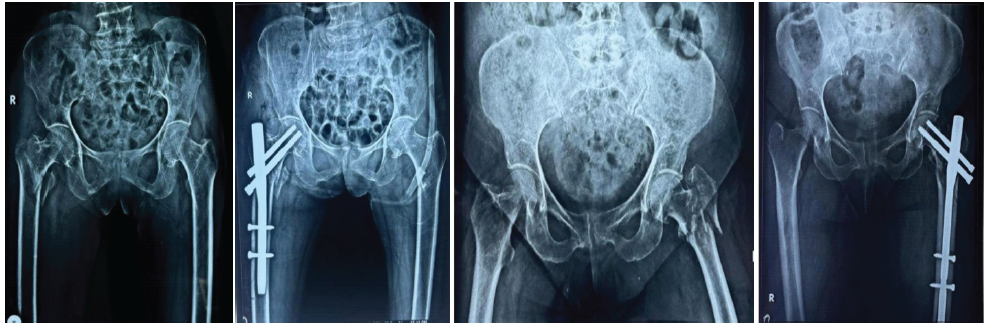
Figure 6: (a) Pre-operative X-ray. (b) Post-operative X-ray (immediate X-ray). (c) Negative medial cortical reduction pre-operative X-ray. (d) Post-operative X-ray.

Figure 7: (a) Pre-operative X-ray. (b) Post-operative X-ray. (c) Implant failure seen in a negative medial cortical reduction at 12 weeks pre-operative X-ray. (d) Post-operative X-ray. (e) 12 weeks post-operative.
The primary finding of this study is that the quality of medial cortical reduction is a significant and independent determinant of functional recovery following surgical fixation of unstable intertrochanteric fractures. Patients who achieved positive medial cortical reduction demonstrated markedly superior WASs at all three post-operative time-points (4 weeks: 14.05 ± 1.87; 6 weeks: 17.0 ± 1.86; and 12 weeks: 19.42 ± 1.61) compared with both neutral and negative reduction groups, directly addressing the study’s primary objective. This trajectory indicates that restoration of the posteromedial bony buttress confers biomechanical stability sufficient to support earlier and more effective weight-bearing rehabilitation.
These findings are consistent with prior national and international literature. Gotfried described the biomechanical rationale for positive medial cortical reduction, demonstrating that cortical overlap at the fracture site redirects axial loads through bone rather than implant, thereby reducing the risk of mechanical failure [20,21]. Similarly, Tsukada et al. reported that post-operative fracture stability on lateral radiographs – closely linked to medial cortical contact – was a key predictor of functional outcome after pertrochanteric fixation [22]. Chang et al. [19] and Kozono et al. [23] likewise emphasized that failure to achieve adequate posteromedial reduction substantially increased the risk of varus collapse and screw cut-out, consistent with our finding of a 4% implant failure rate concentrated in the negative reduction subgroup. Where our results differ from some retrospective series is in the relatively low overall complication rate (10%), which may reflect the predominantly intramedullary approach used (PFN in 42% and long PFN in 22% of cases), as intramedullary devices have been consistently shown to outperform DHSs in truly unstable patterns.
In terms of order of importance, the quality of medial cortical reduction represents the most impactful finding of this study, followed by the choice of surgical implant and then patient-level demographic factors. Age and gender had a measurable but non-significant influence on functional recovery in our cohort: younger patients (<50 years) achieved faster WAS improvement, likely attributable to superior bone quality and lower comorbidity burden, yet this advantage did not reach statistical significance against the older strata at 12 weeks – underlining that optimizing reduction quality can partially offset the disadvantage of osteoporotic bone. Male patients demonstrated modestly higher scores at 6 weeks, though gender differences were resolved by the 12-week follow-up. These findings parallel international data suggesting that surgical quality supersedes demographic factors as a predictor of short-term functional recovery in hip fractures treated with contemporary fixation constructs.
The results of this study further support the use of PFN as the primary fixation strategy for unstable intertrochanteric fractures, consistent with current international guidelines and published systematic reviews. PFN and its variants (long PFN and PFNA-II) accounted for 84% of procedures in this series, and their load-sharing intramedullary design reduces implant stress at the fracture site when compared with extramedullary devices such as DHS. The infrequent use of DHS (2%) in this cohort reflects the evolving consensus that extramedullary fixation is biomechanically suboptimal for AO31-A2 and A3 patterns, particularly in the presence of poor BMD.
The findings of this study are preliminary in nature, given the single-center design, relatively small sample size of 50 patients, and follow-up limited to 12 weeks. Future multi-center prospective studies with longer follow-up periods (minimum 12 months), standardized radiological outcome measures including tip-apex distance and neck-shaft angle, and validated patient-reported outcome measures (e.g., Harris Hip Score and Oxford Hip Score) are needed to confirm and extend these findings. Investigation into the role of BMD as an effect modifier of reduction quality on functional outcomes would also be of significant interest. In addition, comparative studies examining the impact of different fluoroscopic reduction techniques on the probability of achieving positive medial cortical contact could provide actionable surgical guidance.
Several limitations of this study warrant acknowledgment. First, the single-center, single-year design may limit generalizability, as institutional surgical volume and expertise can influence reduction quality and outcomes. Second, the prospective observational design, while reducing recall bias, precludes causal inference and may be subject to selection bias in the assignment of surgical technique. Third, functional recovery was assessed solely by the WAS; future studies should incorporate additional validated instruments to capture pain, quality of life, and return to pre-injury activity level. Fourth, radiological outcomes beyond implant failure were not systematically quantified. Fifth, the study lacked sufficient power to conduct subgroup analyses stratified by fracture classification, BMD category, or surgeon experience. Despite these limitations, the consistency of the functional recovery trends across all follow-up points strengthens confidence in the directional findings.
The study demonstrates that achieving positive and neutral medial cortical reductions significantly improves functional outcomes and reduces complications in patients with unstable intertrochanteric fractures. Proper reduction and stabilization of the medial cortex not only enhances fracture stability but also significantly improves functional recovery and reduces the risk of implant failure. Surgeons should prioritize medial cortical alignment when performing surgical fixation to optimize patient outcomes, particularly in elderly patients with osteoporotic bone.
In unstable intertrochanteric fractures, restoration of medial cortical continuity should be a key intraoperative goal, as even subtle improvements in medial cortical reduction translate into better biomechanical stability, faster functional recovery, and lower rates of implant failure, especially in elderly patients with osteoporotic bone.
References
- 1. Russell TA, Sanders R. Pertrochanteric hip fractures: Time for change. J Orthop Trauma 2011;25:189-90. [Google Scholar] [PubMed]
- 2. Evans E. The treatment of trochanteric fractures of the femur. J Bone Joint Surg Br 1949;31:190-203. [Google Scholar] [PubMed]
- 3. Kaufer H. Mechanics of the treatment of hip injuries. Clin Orthop Relat Res 1980;146:53-61. [Google Scholar] [PubMed]
- 4. Sarmiento A. Intertrochanteric fractures of the femur: 150-degree-angle nail-plate fixation and early rehabilitation: A preliminary report of 100 cases. J Bone Joint Surg Am 1963;45:706-22. [Google Scholar] [PubMed]
- 5. Kokoroghiannis C, Aktselis I, Deligeorgis A, Fragkomichalos E, Papadimas D, Pappadas I. Evolving concepts of stability and intramedullary fixation of intertrochanteric fractures–a review. Injury 2012;43:686-93. [Google Scholar] [PubMed]
- 6. Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, et al. Fracture and dislocation classification compendium – 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21:S1-133. [Google Scholar] [PubMed]
- 7. Andruszkow H, Frink M, Fro¨mke C, Matityahu A, Zeckey C, Mommsen P, et al. Tipapex distance, hip screw placement, and neck shaft angle as potential risk factors for cut-out failure of hipscrews after surgical treatment of intertrochanteric fractures. Int Orthop 2012;36:2347-54. [Google Scholar] [PubMed]
- 8. Davis TR, Sher JL, Horsman A, Simpson M, Porter BB, Checketts RG. Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br 1990;72:26-31. [Google Scholar] [PubMed]
- 9. Frei HC, Hotz T, Cadosch D, Rudin M, Kach K. Central head perforation, or ‘‘cut through,’’ caused by the helical blade of the proximal femoral nail antirotation. J Orthop Trauma 2012;26:e102-7. [Google Scholar] [PubMed]
- 10. Zhou JQ, Chang SM. Failure of PFNA: Helical blade perforation and tip-apex distance. Injury 2012;43:1227-78. [Google Scholar] [PubMed]
- 11. Suhm N, Kaelin R, Studer P, Wang Q, Kressig RW, Rikli D, et al. Orthogeriatric care pathway: A prospective survey of impact on length of stay, mortality and institutionalisation. Arch Orthop Trauma Surg 2014;134:1261-9. [Google Scholar] [PubMed]
- 12. Chang SM, Song DL, Ma Z, Tao YL, Chen WL, Zhang LZ, et al. Mismatch of the short straight cephalomedullary nail (PFNA-II) with the anterior bow of the Femur in an Asian population. J Orthop Trauma 2014;28:17-22. [Google Scholar] [PubMed]
- 13. Johnson B, Stevenson J, Chamma R, Patel A, Rhee SJ, Lever C, et al. Short-term follow-up of pertrochanteric fractures treated using the proximal femoral locking plate. J Orthop Trauma 2014;28:283-7. [Google Scholar] [PubMed]
- 14. Jensen JS. Classification of trochanteric fractures. Acta Orthop Scand 1980;51:803-10. [Google Scholar] [PubMed]
- 15. Zuckerman JD, Sakales SR, Fabian DR, Frankel VH. Hip fractures in geriatric patients. Results of an interdisciplinary hospital care program. Clin Orthop Relat Res 1992;274:213-25. [Google Scholar] [PubMed]
- 16. Parker MJ, Palmer CR. A new mobility score for predicting mortality after hip fracture. J Bone Joint Surg Br 1993;75:797-8. [Google Scholar] [PubMed]
- 17. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am 1995;77:1058-64. [Google Scholar] [PubMed]
- 18. Kim Y, Dheep K, Lee J, Yoon YC, Shon WY, Oh CW, et al. Hook leverage technique for reduction of intertrochanteric fracture. Injury 2014;45:1006-10. [Google Scholar] [PubMed]
- 19. Chang SM, Zhang YQ, Ma Z, Li Q, Dargel J, Eysel P. Fracture reduction with positive medial cortical support: A key element in stability reconstruction for the unstable pertrochanteric hip fractures. Arch Orthop Trauma Surg. 2015;135:811-8. [Google Scholar] [PubMed]
- 20. Gotfried Y. The Gotfried (nonanatomic, closed) reduction of unstable subcapital femoral fractures. Tech Orthop 2012;27:259-61. [Google Scholar] [PubMed]
- 21. Gotfried Y, Kovalenko S, Fuchs D. Nonanatomical reduction of displaced subcapital femoral fractures (gotfried reduction). J Orthop Trauma 2013;27:e254-9. [Google Scholar] [PubMed]
- 22. Tsukada S, Okumura G, Matsueda M. Postoperative stability on lateral radiographs in the surgical treatment of pertrochanteric hip fractures. Arch Orthop Trauma Surg 2012;132:839-46 [Google Scholar] [PubMed]
- 23. Kozono N, Ikemura S, Yamashita A, Harada T, Watanabe T, Shirasawa K. Direct reduction may need to be considered to avoid postoperative subtype P in patients with an unstable trochanteric fracture: A retrospective study using a multivariate analysis. Arch Orthop Trauma Surg 2014;134:1649-54. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Clinical-Radiological Dissociation after Failed Monteggia Fixation: Preserved Function at 2 Years Despite Proximal Ulnar Fibrous Non-union and Chronic Lateral Radial Head Dislocation
July 1, 2026 Clinical-Radiological Dissociation after Failed Monteggia Fixation: Preserved Function at 2 Years Despite Proximal Ulnar Fibrous Non-union and Chronic Lateral Radial Head Dislocation July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report
June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report May 1, 2026 Salvage of Infected Dynamic Hip Screw and Distal Femur Nail Fixation for Ipsilateral Femoral Neck and Femoral Shaft Fracture Using Antibiotic-Coated Custom Long-Stem Austin Moore Prosthesis – A Rare Case Report
May 1, 2026 Salvage of Infected Dynamic Hip Screw and Distal Femur Nail Fixation for Ipsilateral Femoral Neck and Femoral Shaft Fracture Using Antibiotic-Coated Custom Long-Stem Austin Moore Prosthesis – A Rare Case Report