
A long-stem antibiotic-coated custom Austin Moore prosthesis may be considered as a salvage option in complex infected ipsilateral femoral fractures when conventional strategies fail.
Dr Ajit S Rathod, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: ajit.rathod.5659@gmail.com
Abstract
Introduction: Ipsilateral femoral neck and shaft fractures are rare injuries (2–10%), typically resulting from high-energy trauma. Dual fixation using a dynamic hip screw (DHS) and distal femoral nailing (DFN) is standard; however, deep infection following such fixation presents a major therapeutic challenge.
Case Report: We report a case of a middle-aged male with an ipsilateral femoral neck and shaft fracture managed initially with DHS and DFN. The post-operative course was complicated by chronic deep infection with persistent sinus and implant loosening despite repeated debridement and antibiotic therapy.
Management and Outcome: The patient underwent implant removal, radical debridement, and reconstruction using a long-stem antibiotic-coated custom-made Austin Moore prosthesis. At 2-year follow-up, the patient was infection-free, pain-free, ambulatory without support, and demonstrated satisfactory functional outcome as assessed by Harris Hip Score.
Conclusion: A custom long-stem antibiotic-coated Austin Moore prosthesis may serve as a feasible single-stage salvage option in selected cases of infected dual femoral fixation. However, further studies are required to validate its reproducibility and long-term outcomes.
Keywords: Ipsilateral femur fracture, dynamic hip screw, distal femoral nail, infection, Austin Moore prosthesis.
Ipsilateral fractures of the femoral neck and shaft are uncommon but complex injuries, accounting for approximately 2–10% of femoral fractures [1,2]. These injuries typically occur due to high-energy trauma, such as road traffic accidents or falls from height [1,2]. Standard treatment involves dual fixation, commonly with dynamic hip screw (DHS) for the neck fracture and intramedullary or distal femoral nailing for the shaft [2,3]. While this approach offers good mechanical stability, complications, such as non-union, implant failure, and deep infection can significantly compromise outcomes [1,4,5]. Among these, infection following dual implant fixation is particularly difficult to manage because of the presence of multiple implants, associated bone loss, instability, and a poor biological environment [5,6]. Recent advances suggest that Prosthetic reconstruction, particularly with antibiotic-coated custom implants, can serve as an effective salvage strategy by addressing both infection and biomechanics in a single stage [7,8,9,10]. We present a rare case of infected DHS and distal femur nails (DFN) in an ipsilateral femoral neck and shaft fracture successfully managed with a long-stem antibiotic-coated custom-made Austin Moore prosthesis.
A 40-year-old male presented following a high-energy road traffic accident with pain, deformity, and inability to bear weight on the left lower limb. Clinical examination revealed an open wound measuring approximately 3 × 2 cm over the hip and thigh region. Radiographs demonstrated a displaced femoral neck fracture with an ipsilateral femoral shaft fracture (Fig. 1).
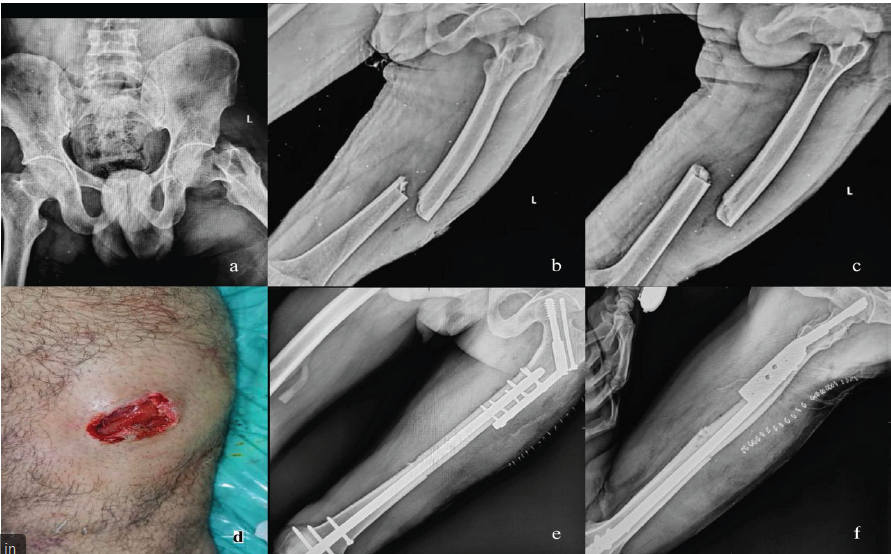
Figure 1: Pre-operative X-rays, clinical picture, and post-operative X-rays. (a) X-ray pelvis and both hips anterior posterior (AP) view, (b) X-ray left femur AP view, (c) X-ray left femur lateral view, (d) clinical picture on the day of presentation, (e) post-operative X-ray left femur AP view, (f) post-operative X-ray left femur lateral view.
The patient underwent primary fixation with DHS for the femoral neck fracture and DFN fixation for the shaft fracture. The immediate post-operative recovery was initially uneventful (Fig. 1). On post-operative day 10, serosanguinous discharge was noted from the wound, although culture was negative at that stage. Debridement was performed, and intravenous antibiotics were administered. By post-operative day 30, wound gaping developed, for which vacuum-assisted closure therapy was applied. At 5 months, the patient continued to have persistent wound discharge, and culture showed methicillin-resistant Staphylococcus aureus (MRSA). The patient was planned for debridement and antibiotic-coated cement bead insertion (Fig. 2).

Figure 2: 5 Months post-injury clinical picture and post-operative X-rays. (a) Clinical picture showing wound gaping and discharging sinus, (b) post-antibiotic coated cement bead insertion X-ray left femur anterior posterior view, (c) post-antibiotic coated cement bead insertion X-ray left femur lateral view.
At 18 months, he presented with a discharging sinus, implant loosening on radiographs, and loss of cortical continuity on the medial and posterolateral aspect on computed tomography, indicating chronic infection and failure of fixation (Fig. 3). Despite multiple debridements, intravenous antibiotics, and antibiotic cement bead insertion, infection persisted. The chronicity of infection, implant loosening, and compromised biology made further fixation strategies less favourable.
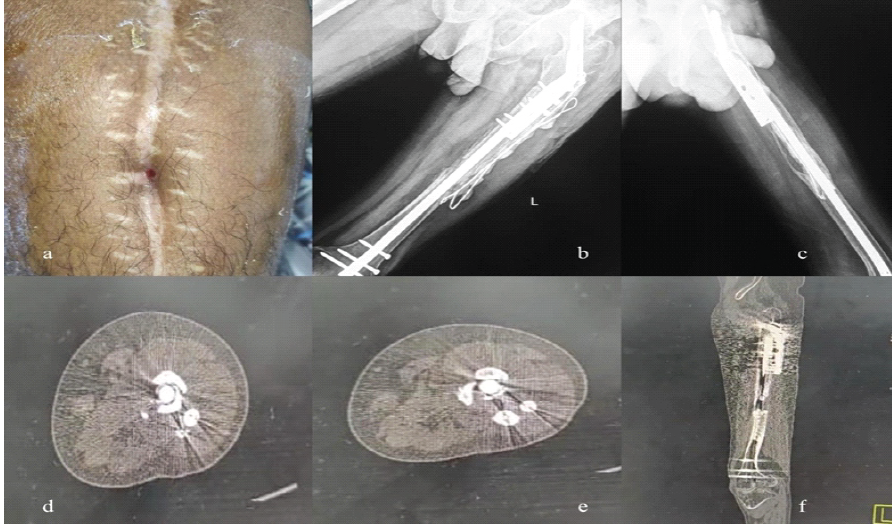
Figure 3: 18 Months Post Injury Clinical Picture, X-Rays and computed tomography (CT) images.
(a) – Clinical Picture showing Discharging sinus
(b), (c) – Post injury X-Rays showing loosening of Implants
(d), (e), (f) – CT showing no Cortical Continuity at medial and posterolateral aspect
The patient had undergone multiple prior surgical interventions with persistent infection and implant failure, resulting in significant biological and mechanical compromise. Considering the chronicity of infection, poor bone stock, and the patient’s preference to avoid multiple staged procedures, a single-stage salvage approach was planned. The objective was to achieve infection control, restore limb function, and minimize further surgical morbidity.
A salvage procedure was planned in view of persistent infection and implant failure. The patient underwent removal of the DHS and distal femoral nail, followed by radical debridement of all infected and necrotic tissue. Reconstruction was performed using a long-stem antibiotic-coated custom Austin Moore prosthesis.
The custom prosthesis was prepared using intraoperative measurement of the contralateral femoral head to achieve appropriate sizing. Antibiotic-loaded bone cement (vancomycin 2 g and tobramycin 1.2 g per 40 g cement) was applied over the prosthesis using a sterile improvised mold to ensure a uniform coating and adequate cement mantle while avoiding excessive bulk that could hinder insertion. An autoclaved scoop was utilized to shape the prosthetic head to the desired dimensions. The long stem was designed to bypass the infected and structurally compromised segment of the femoral shaft, allowing distal fixation in relatively healthy bone and providing stability across the partially united fracture. This single-stage approach aimed to achieve infection control, maintain limb length, and facilitate early mobilization through combined mechanical stability and high local antibiotic delivery [6,7]. The decision for this strategy was further supported by the need for definitive management in a setting of chronic infection and prior surgical interventions [8–11]. [Fig.4]
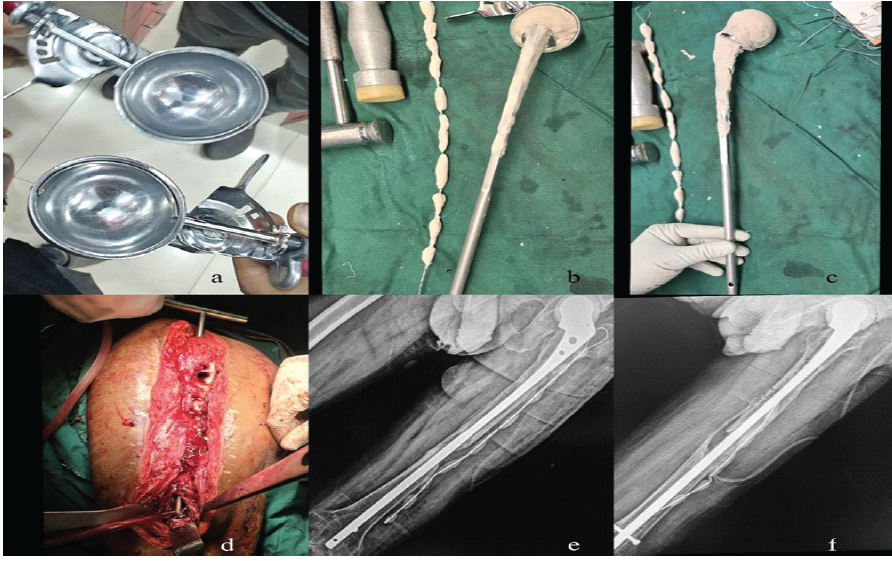
Figure 4: Intra-operative implants used, clinical picture, and post-operative X-rays. (a) Ice-cream scoop of measured dimension as per the head of the femur, (b and c) customized cement-coated AMP with antibiotic-coated cement beads, (d) intra-op clinical picture of exposure, (e and f) post-operative X-rays (anterior posterior and lateral).
Outcome:
Postoperatively, the patient was mobilized early with partial weight-bearing and progressed to full weight-bearing from 2 weeks onwards. At 2-year follow-up, the patient remained pain-free, ambulatory without support, and showed no clinical or radiological evidence of recurrent infection. Radiographs demonstrated stable prosthesis positioning. [Fig.5]
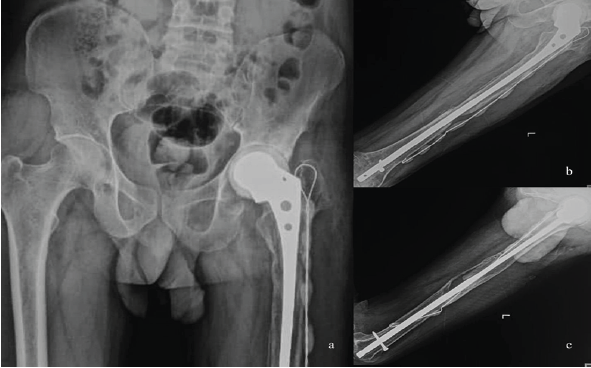
Figure 5: 2 Year follow-up X-rays, (a) X-ray pelvis and both hips anterior posterior (AP) view, (b) X-ray left femur AP view, (c) X-ray left femur lateral view.
Functional outcome was assessed using the Harris Hip Score, with a total score of 82 points, indicating a good functional result. This reflects satisfactory functional recovery despite multiple prior surgical interventions.
Management of infection following dual fixation in ipsilateral femoral neck and shaft fractures remains challenging, with no universally accepted treatment protocol. Conventional options include staged procedures with implant removal, antibiotic spacers, and delayed reconstruction; arthrodesis; or megaprosthesis reconstruction. Each approach carries limitations such as prolonged treatment duration, compromised function, or technical complexity. [3,5,6,9,10] In the present case, a single-stage salvage strategy was chosen due to chronic infection, implant loosening, poor bone stock, and the patient’s preference to avoid multiple surgical procedures. The use of an antibiotic-coated prosthesis allows simultaneous mechanical stability and high local antibiotic delivery. However, this approach should be considered selectively, particularly when conventional fixation or staged reconstruction is unlikely to succeed. [6–8] Compared to megaprosthesis, this technique may be more cost-effective and adaptable, especially in resource-limited settings, although it lacks standardization and long-term outcome data. [8–11] Arthrodesis, while effective for infection control, significantly compromises joint function and patient satisfaction. Functional outcome was assessed using the Harris Hip Score, with a total score of 82 points, indicating a good functional result. The breakdown was as follows: pain (44/44), function (30/47), absence of deformity (4/4), and range of motion (4/5). The reduced function score reflects the presence of approximately 2 cm limb shortening and a mild Trendelenburg gait. Despite these limitations, the patient remained pain-free and ambulatory without support, indicating satisfactory functional recovery following multiple prior surgical interventions. The absence of reinfection or implant-related complications at 2-year follow-up further supports the potential durability of this salvage strategy in selected cases. Thus, this case highlights a potential salvage option rather than establishing a definitive treatment strategy, and the findings should be interpreted with caution. This approach may be particularly relevant in resource-limited settings where access to megaprosthesis is constrained.
Infected DHS and distal femoral nail fixation in ipsilateral femoral neck and shaft fractures represent a complex clinical challenge. Implant removal with thorough debridement followed by reconstruction using a long-stem antibiotic-coated custom Austin Moore prosthesis may provide a viable salvage option in selected cases. However, given the limitations of a single case and lack of comparative evidence, the results should be interpreted with caution despite encouraging mid-term outcomes, and further studies are required to establish its role in clinical practice.
In cases of ipsilateral femoral neck and shaft fractures treated with dual implants, persistent wound issues or delayed healing should raise suspicion of deep infection. Timely implant removal and thorough debridement are essential. In selected complex cases with poor bone stock and chronic infection, a long-stem antibiotic-coated custom prosthesis may be considered as a single-stage salvage option.
References
- 1. Gupta A, Jain A, Mittal S, Chowdhury B, Trikha V. Ipsilateral femoral neck and shaft fractures: Case series from a single Level-I trauma centre and review of literature. Eur J Orthop Surg Traumatol 2023;33:803-9. [Google Scholar] [PubMed]
- 2. Singh R, Rohilla R, Magu NK, Siwach R, Kadian V, Sangwan SS. Ipsilateral femoral neck and shaft fractures: A retrospective analysis of two treatment methods. J Orthop Traumatol 2008;9:141-7. [Google Scholar] [PubMed]
- 3. Alfonso D, Vasquez O, Egol K. Concomitant ipsilateral femoral neck and femoral shaft fracture nonunions: A report of three cases and a review of the literature. Iowa Orthop J 2006;26:112-8. [Google Scholar] [PubMed]
- 4. Kumar A, Khan R, Jameel J, Kumar S. Salvaging chronic nonunion of femoral neck and infected nonunion of ipsilateral femoral shaft fracture using intramedullary antibiotic cement spacer and external fixator alone. Cureus 2021;13:e12665. [Google Scholar] [PubMed]
- 5. Riedl M, Straub J, Walter N, Baertl S, Baumann F, Alt V, et al. Fracture-related infection of the proximal femur – diagnostics and treatment. Geriatr Orthop Surg Rehabil 2025;16:21514593251324768. [Google Scholar] [PubMed]
- 6. Jain AK, Sinha S. Infected nonunion of the long bones. Clin Orthop Relat Res 2005;431:57-65. [Google Scholar] [PubMed]
- 7. Hardes J, Von Eiff C, Streitbuerger A, Balke M, Budny T, Henrichs MP, et al. Reduction of periprosthetic infection with silver-coated megaprostheses in patients with bone sarcoma. J Surg Oncol 2010;101:389-95. [Google Scholar] [PubMed]
- 8. Cianni L, Taccari F, Bocchi MB, Micheli G, Sangiorgi F, Ziranu A, et al. Characteristics and epidemiology of megaprostheses infections: A systematic review. Healthcare (Basel) 2024;12:1283. [Google Scholar] [PubMed]
- 9. Şirin E, Sofulu Ö, Baysal Ö, Akgülle AH, Erol B. Staged management of infection with adjustable spacers after megaprosthesis implantation in primary sarcoma patients. Indian J Orthop 2023;57:938-47. [Google Scholar] [PubMed]
- 10. Hidayat AY, Rifardi D, Pribadi BP. Surgical options for improving the ipsilateral femoral neck, shaft, and distal femoral fracture: A case report and literature review. Int J Surg Case Rep 2024;116:109367. [Google Scholar] [PubMed]
- 11. Thonse R, Conway J. Antibiotic cement-coated interlocking nail for the treatment of infected nonunions and segmental bone defects. J Orthop Trauma 2007;21:258-68. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures
May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures March 1, 2026 Case Report: Chronic Olecranon Bursitis as a Risk Factor for Squamous Cell Carcinoma
March 1, 2026 Case Report: Chronic Olecranon Bursitis as a Risk Factor for Squamous Cell Carcinoma February 1, 2026 Simplified Negative Pressure Wound Therapy: A Cost-Effective Solution for Wound Management
February 1, 2026 Simplified Negative Pressure Wound Therapy: A Cost-Effective Solution for Wound Management