
Vitamin D deficiency is highly prevalent among patients with long-bone fractures and may impair the biological processes essential for optimal fracture healing. Weekly high-dose Vitamin D supplementation provides more rapid biochemical correction than daily low-dose regimens and is associated with a shorter time to radiological union. Targeted optimization of Vitamin D status may therefore serve as an effective adjunct to enhance fracture healing outcomes.
Dr. Prabakaran Vaithinathan, Department of General Medicine, Vinayaka Mission’s Medical College And Hospital, Puducherry, India. E-mail: vpkn0304@gmail.com
Abstract
Introduction: Vitamin D plays a critical role in bone metabolism and mineralization, and deficiency is highly prevalent among patients presenting with long-bone fractures. Impaired Vitamin D status may adversely affect fracture healing by disrupting calcium homeostasis and bone remodeling. However, the optimal supplementation regimen for improving fracture healing outcomes remains uncertain. To compare the effects of daily low-dose versus weekly high-dose Vitamin D supplementation on fracture healing and serum biomarker profiles in patients with long-bone fractures.
Materials and Methods: This prospective randomized study included 50 adult patients with acute long-bone fractures and baseline serum 25-hydroxyvitamin D levels below 30 ng/mL. Patients were randomized into two groups: Group A received oral Vitamin D3 1,000 IU daily, while Group B received oral Vitamin D3 60,000 IU weekly, both for 12 weeks. Serum Vitamin D, calcium, phosphorus, alkaline phosphatase, and parathyroid hormone (PTH) levels were assessed at baseline, 12 weeks, and 24 weeks. Fracture healing was evaluated clinically and radiologically, with time to union recorded. Statistical analysis was performed using appropriate parametric and non-parametric tests, with P < 0.05 considered significant.
Results: Both supplementation regimens significantly improved serum Vitamin D levels; however, the weekly regimen achieved higher levels at 12 weeks (32.8 ± 7.4 ng/mL vs. 27.3 ± 6.1 ng/mL; P = 0.01) and 24 weeks (36.2 ± 7.9 ng/mL vs. 30.5 ± 6.8 ng/mL; P = 0.004). Serum calcium levels increased and PTH levels decreased significantly, with greater changes observed in the weekly supplementation group. The mean time to radiological fracture union was significantly shorter in Group B (15.9 ± 2.8 weeks) compared to Group A (18.6 ± 3.2 weeks; P = 0.002). Both regimens were well tolerated, with no serious adverse events.
Conclusion: Weekly high-dose Vitamin D supplementation resulted in superior biochemical correction and faster fracture healing compared to daily low-dose supplementation in Vitamin D–deficient patients with long-bone fractures. Routine assessment and targeted correction of Vitamin D deficiency may improve fracture healing outcomes.
Keywords: Vitamin D supplementation, fracture healing, long-bone fractures, randomized controlled study, serum biomarkers.
Aim and background
Vitamin D plays a pivotal role in skeletal health through its regulation of calcium and phosphorus homeostasis, bone mineralization, and musculoskeletal function. Long-bone fractures constitute a significant global health burden, leading to prolonged disability, reduced quality of life, and substantial socioeconomic costs. Optimal fracture healing is a complex, multistage biological process involving inflammation, callus formation, mineralization, and remodeling, all of which are influenced by systemic and local metabolic factors. Among these, Vitamin D status has gained increasing attention as a potentially modifiable determinant of fracture healing outcomes [1]. Despite advances in surgical fixation techniques and post-operative rehabilitation, delayed union and non-union remain common complications, particularly in patients with underlying nutritional deficiencies [2].
Vitamin D deficiency is highly prevalent worldwide, including in sunny regions, such as India, due to factors, such as inadequate dietary intake, limited sun exposure, darker skin pigmentation, and lifestyle changes. Several studies have reported a high prevalence of hypovitaminosis D among patients presenting with fractures, with estimates ranging from 40% to 80% depending on the population studied [3,4]. Vitamin D exerts its effects on bone through binding to the Vitamin D receptor, which is expressed in osteoblasts, osteoclasts, chondrocytes, and myocytes. Experimental studies have demonstrated that Vitamin D influences osteoblast differentiation, matrix mineralization, and osteoclast-mediated bone resorption, suggesting a direct role in bone repair mechanisms [5].
Fracture healing is an energy- and mineral-intensive process requiring adequate calcium availability and coordinated hormonal regulation. Vitamin D deficiency leads to secondary hyperparathyroidism, increased bone turnover, impaired mineralization, and reduced mechanical strength of the healing callus [6]. Animal models have shown that Vitamin D–deficient states are associated with delayed callus maturation and inferior biomechanical properties of healed bone, while supplementation can partially reverse these effects [7]. In humans, observational studies have suggested associations between low serum 25-hydroxyvitamin D (25[OH]D) levels and delayed fracture healing, increased pain, and poorer functional outcomes [8].
Serum biomarkers play an important role in understanding the biological milieu of fracture healing. Markers, such as calcium, phosphorus, alkaline phosphatase (ALP), parathyroid hormone (PTH), and bone turnover markers reflect different stages of bone formation and resorption. Vitamin D supplementation has been shown to influence these biomarkers by increasing serum calcium and phosphate absorption, reducing PTH levels, and modulating ALP activity, thereby creating a favorable environment for bone repair [9]. However, the optimal dosing regimen of Vitamin D for enhancing fracture healing remains controversial. Various supplementation strategies – including daily low-dose, weekly moderate-dose, and single or intermittent high-dose (bolus) regimens – are currently used in clinical practice, with inconsistent evidence regarding their comparative efficacy and safety [10].
Randomized controlled trials evaluating Vitamin D supplementation in fracture patients have yielded mixed results, partly due to heterogeneity in fracture types, baseline Vitamin D status, dosing regimens, and outcome measures. Some studies have reported improved radiological healing and functional recovery with supplementation, while others have failed to demonstrate significant benefits beyond correction of biochemical deficiency. Moreover, concerns have been raised regarding high-dose bolus Vitamin D therapy, which may cause transient hypercalcemia or paradoxically increase bone resorption if not appropriately monitored [11]. These uncertainties highlight the need for well-designed prospective randomized studies comparing different Vitamin D supplementation regimens in patients with long-bone fractures.
Understanding the impact of Vitamin D supplementation not only on clinical and radiological healing but also on serum biomarker profiles may provide valuable insights into the mechanistic pathways involved in fracture repair. By correlating biochemical changes with healing outcomes, it may be possible to identify optimal supplementation strategies tailored to patient-specific needs. Therefore, a prospective randomized study evaluating the effect of different Vitamin D supplementation regimens on fracture healing and serum biomarkers in long-bone fractures is clinically relevant and timely. Such evidence could inform standardized guidelines, improve patient outcomes, and reduce the burden of delayed fracture healing and its associated complications.
Study design
This study was conducted as a prospective, randomized, interventional clinical study designed to evaluate the effect of different Vitamin D supplementation regimens on fracture healing and serum biomarker profiles in patients with long-bone fractures.
Study setting
The study was carried out in the Department of Orthopaedics in collaboration with the Department of Biochemistry at a tertiary care teaching hospital.
Study duration
The study was conducted over a period of 18 months, which included patient recruitment, intervention, follow-up, and data analysis. Each participant was followed for a minimum duration of 24 weeks from the time of fracture fixation to assess fracture healing and biomarker changes.
Participants
Inclusion criteria
- Patients aged 18–65 years
- Patients with acute long-bone fractures (femur, tibia, humerus, radius, or ulna)
- Patients undergoing operative or conservative management
- Serum 25(OH)D level <30 ng/mL at baseline
- Patients willing to provide written informed consent.
Exclusion criteria
- Pathological fractures
- Open fractures of Gustilo–Anderson grade III
- Known metabolic bone disorders (osteomalacia, Paget’s disease)
- Chronic kidney disease, chronic liver disease, or malabsorption syndromes
- Patients on long-term steroids, anticonvulsants, or bisphosphonates
- Hypercalcemia or known hypersensitivity to Vitamin D
- Pregnant or lactating women.
Study sampling
A consecutive sampling technique was used. All eligible patients presenting to the orthopedic department with long-bone fractures during the study period were screened for inclusion. Patients meeting the eligibility criteria were enrolled until the required sample size was achieved.
Study sample size
The total sample size was 50 patients. This sample size was chosen based on feasibility considerations, patient availability during the study period, and similar previously published interventional studies evaluating Vitamin D supplementation in fracture healing. Patients were evenly distributed between study groups to allow comparative analysis.
Study groups
Participants were randomly allocated into two equal groups (n = 25 each) using a computer-generated randomization table:
- Group A (daily supplementation group): Patients received oral Vitamin D3 at a dose of 1,000 IU daily for 12 weeks
- Group B (weekly supplementation group): Patients received oral Vitamin D3 at a dose of 60,000 IU once weekly for 12 weeks.
Both groups received standard fracture management and calcium supplementation as per institutional protocol.
Study parameters
The study parameters included both primary and secondary outcome measures to comprehensively assess the impact of Vitamin D supplementation on fracture healing. The primary outcome measures were the time to radiological fracture union and serum 25(OH)D levels. Secondary outcome measures included serum calcium and phosphorus levels, serum ALP levels, serum PTH levels, and clinical indicators of fracture healing, such as reduction in pain and improvement in weight-bearing or functional use of the affected limb.
Study procedure
After enrollment, baseline demographic data and clinical details were recorded. Blood samples were collected before initiation of Vitamin D supplementation to assess baseline biochemical parameters. Patients were then randomized into respective groups and initiated on the assigned Vitamin D regimen. Fracture management was carried out according to standard orthopedic protocols, independent of group allocation. Follow-up visits were scheduled at 6 weeks, 12 weeks, and 24 weeks, during which clinical assessment, radiological evaluation, and blood sampling were performed.
Study data collection
Data were collected using a structured pro forma. Clinical assessment included evaluation of pain, tenderness at the fracture site, and the ability to bear weight or use the affected limb. Radiological healing was assessed using serial X-rays and graded based on cortical continuity and callus formation. Blood samples were analyzed for Vitamin D and bone-related biomarkers at baseline and follow-up visits. All data were entered into a secured database for analysis.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences software. Continuous variables were expressed as mean ± standard deviation, while categorical variables were expressed as frequencies and percentages. Intergroup comparisons were performed using independent t-tests or Mann–Whitney U tests, while intragroup comparisons were analyzed using paired t-tests. A P < 0.05 was considered statistically significant.
Ethical considerations
The study was conducted after obtaining approval from the Institutional Ethics Committee. Written informed consent was obtained from all participants before enrollment. Confidentiality of patient data was strictly maintained, and participants were free to withdraw from the study at any stage without affecting their standard medical care. No additional financial burden was imposed on participants, and adverse events related to supplementation were monitored throughout the study period.
A total of 50 patients with long-bone fractures were included in the final analysis and were equally randomized into Group A (daily Vitamin D, n = 25) and Group B (weekly Vitamin D, n = 25). All patients completed the scheduled follow-up, and no major protocol deviations were observed (Table 1).
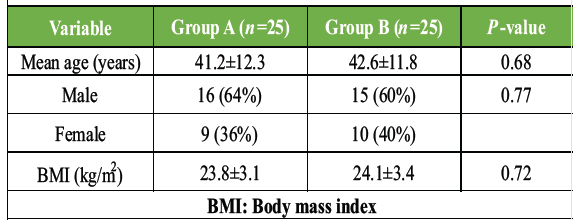
Table 1: Demographic characteristics of study participants. Baseline demographic characteristics of patients in Group A (daily Vitamin D supplementation) and Group B (weekly Vitamin D supplementation), showing comparable age, sex distribution, and body mass index between groups
Both groups were comparable in terms of age, gender distribution, and body mass index (BMI), indicating effective randomization and minimizing demographic confounding Table 2.
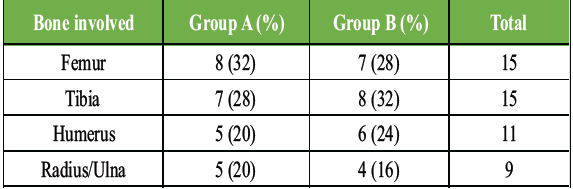
Table 2: Distribution of long-bone fracture types. Distribution of fracture sites among study participants in both groups, demonstrating similar representation of femur, tibia, humerus, and radius/ulna fractures
The distribution of fracture types was similar across both groups, ensuring that fracture location did not bias healing outcomes Table 3.
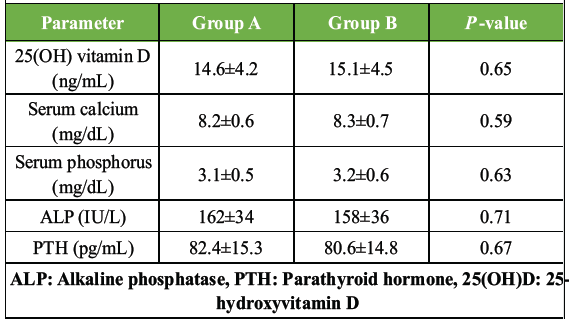
Table 3: Baseline serum biomarker levels. Baseline serum levels of 25(OH)D, calcium, phosphorus, ALP, and PTH in both groups before initiation of Vitamin D supplementation
Baseline biochemical parameters showed no statistically significant differences, confirming comparable Vitamin D deficiency and bone metabolic status at study entry Tables 4 and 5, Fig. 1.
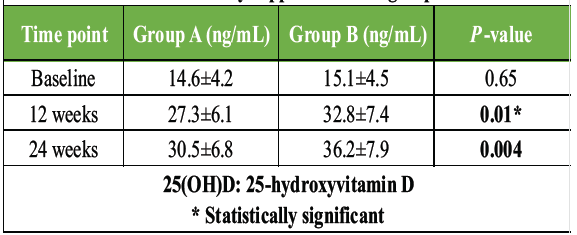
Table 4: Change in serum vitamin D levels over time. Comparison of serum 25(OH)D levels at baseline, 12 weeks, and 24 weeks in daily versus weekly supplementation groups
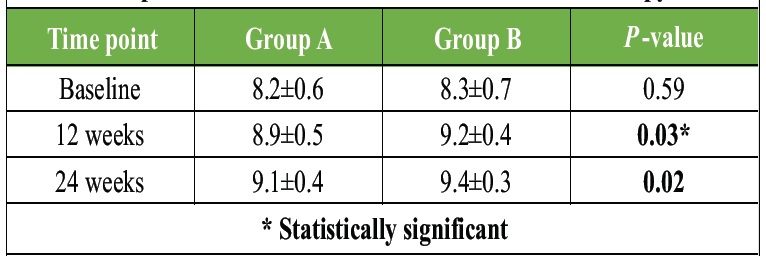
Table 5: Serum calcium levels during follow-up. Serial changes in serum calcium levels in both supplementation groups during follow-up, reflecting improved calcium homeostasis with Vitamin D therapy
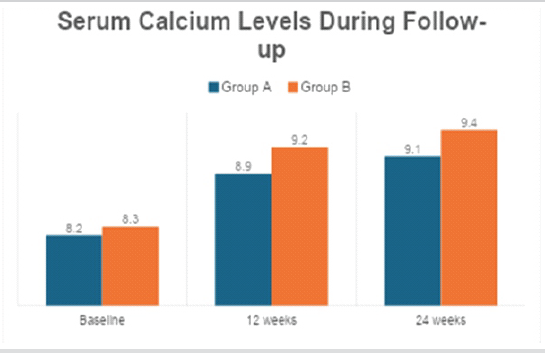
Figure 1: Change in serum vitamin D levels over time. Graphical representation of serum 25-hydroxyvitamin D levels at baseline, 12 weeks, and 24 weeks in daily and weekly supplementation groups.
Serum calcium levels increased significantly in both groups, with Group B showing superior normalization, reflecting improved calcium absorption Table 6 and Fig. 2.
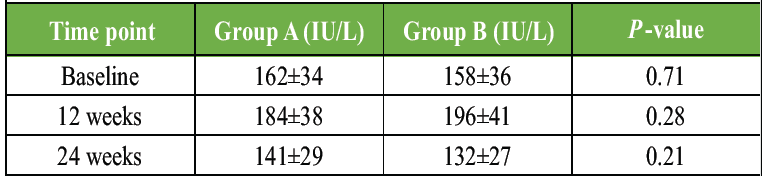
Table 6: Changes in serum alkaline phosphatase (ALP) levels. Variation in serum ALP levels during fracture healing in both groups, indicating bone formation and remodeling activity
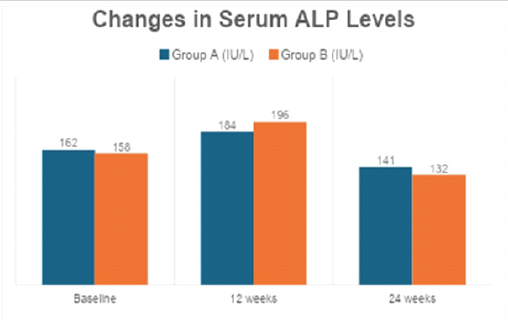
Figure 2: Serum calcium level trends during follow-up. Comparison of serum calcium levels over time between group a and group b, showing superior normalization in the weekly supplementation group.
ALP levels peaked during early healing and declined by 24 weeks, indicating progression from callus formation to remodeling in both groups Tables 7 and 8, Figs. 3 and 4.
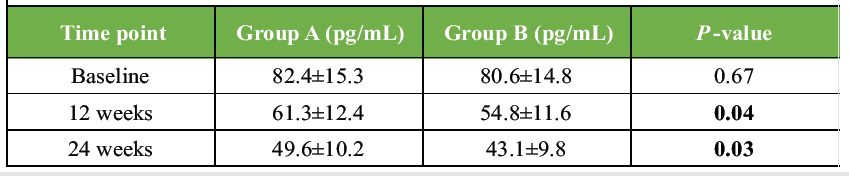
Table 7: Parathyroid hormone (PTH) levels. Changes in serum PTH levels at baseline, 12 weeks, and 24 weeks, demonstrating correction of secondary hyperparathyroidism following Vitamin D supplementation

Table 8: Radiological time to fracture union. Comparison of mean time to radiological fracture union between daily and weekly Vitamin D supplementation groups
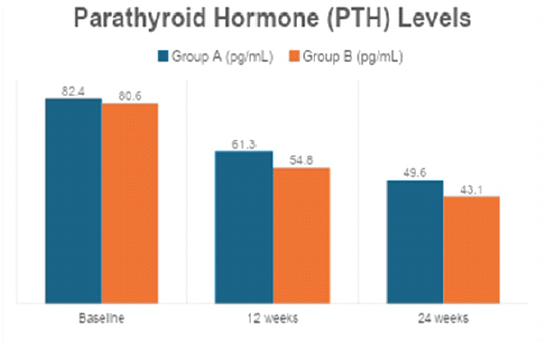
Figure 3: Radiological time to fracture union. Bar diagram comparing mean radiological fracture union time between daily and weekly vitamin D supplementation groups.
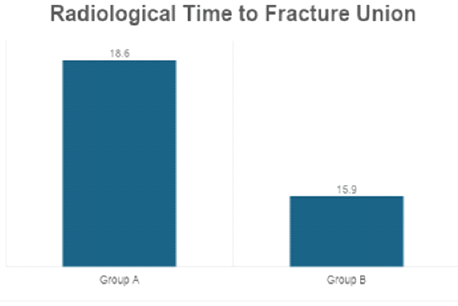
Figure 4: Fracture healing status at 24 weeks. Graphical comparison of radiological union and delayed union rates between the two study groups at final follow-up.
Patients receiving weekly Vitamin D supplementation demonstrated significantly faster radiological union compared to the daily-dose group.
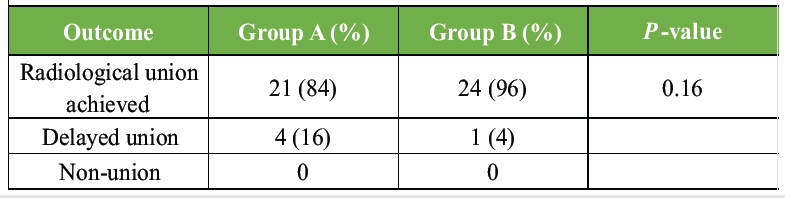
Table 9: Clinical fracture healing outcomes at 24 weeks. Comparison of radiological union, delayed union, and non-union rates between the two study groups at 24 weeks follow-up.
Table 9 Although not statistically significant, a higher proportion of complete fracture union was observed in Group B Table 10. Both supplementation regimens were well tolerated, with no serious adverse events requiring discontinuation of therapy.
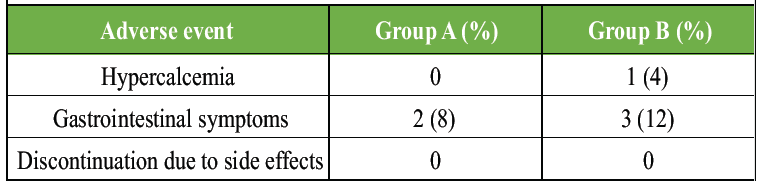
Table 10: Adverse events and safety profile. Incidence of adverse events and treatment tolerability in patients receiving daily versus weekly vitamin D supplementation
The present prospective randomized study evaluated the effect of two Vitamin D supplementation regimens on fracture healing and serum biomarker profiles in patients with long-bone fractures and demonstrated that Vitamin D supplementation favorably influenced biochemical correction and fracture healing outcomes, with weekly high-dose supplementation showing superior results compared to daily low-dose therapy. At baseline, both groups exhibited comparable and deficient Vitamin D levels (Group A: 14.6 ± 4.2 ng/mL; Group B: 15.1 ± 4.5 ng/mL), a finding consistent with the high prevalence of hypovitaminosis D reported in fracture populations by Memon et al., [12] where 45.0% of patients were Vitamin D deficient and only 23.3% had sufficient levels at presentation [5]. Following supplementation, a significant rise in serum 25(OH)D was observed in both groups; however, the weekly 60,000 IU regimen resulted in higher levels at 12 weeks (32.8 ± 7.4 ng/mL vs. 27.3 ± 6.1 ng/mL; P = 0.01) and 24 weeks (36.2 ± 7.9 ng/mL vs. 30.5 ± 6.8 ng/mL; P = 0.004). This enhanced biochemical repletion aligns with the dosing-related effects observed in the Vita Shock trial by Slobogean et al., [13], where higher Vitamin D3 doses demonstrated trends toward improved clinical fracture healing compared to placebo, although pre-specified analyses did not show statistically significant differences. The superior Vitamin D normalization in the weekly group in the present study likely contributed to improved downstream calcium homeostasis and fracture healing dynamics.
Serum calcium levels increased significantly in both groups, with higher values observed in the weekly supplementation group at 12 weeks (9.2 ± 0.4 mg/dL vs. 8.9 ± 0.5 mg/dL; P = 0.03) and 24 weeks (9.4 ± 0.3 mg/dL vs. 9.1 ± 0.4 mg/dL; P = 0.02), reflecting improved intestinal calcium absorption mediated by corrected Vitamin D status. This biochemical improvement was accompanied by a significant decline in serum PTH levels, particularly in Group B at 24 weeks (43.1 ± 9.8 pg/mL vs. 49.6 ± 10.2 pg/mL; P = 0.03), suggesting reversal of secondary hyperparathyroidism. Although Gatt et al. [11] reported that Vitamin D supplementation had no demonstrable effect on ultimate fracture union when assessed by clinical examination and plain radiographs, their systematic review acknowledged that biochemical deficiency correction did not consistently translate into measurable clinical endpoints in heterogeneous adult fracture populations. In contrast, the present study demonstrated that correction of Vitamin D deficiency was associated with measurable improvements in healing time, suggesting that biochemical normalization may be more relevant when baseline deficiency is pronounced and supplementation is initiated early.
ALP levels in the present study followed a predictable fracture-healing pattern, increasing at 12 weeks (Group A: 184 ± 38 IU/L; Group B: 196 ± 41 IU/L) and declining by 24 weeks (Group A: 141 ± 29 IU/L; Group B: 132 ± 27 IU/L), indicating progression from active osteoblastic callus formation to remodeling. While intergroup differences were not statistically significant, this pattern supports physiological fracture healing in both regimens. These findings align with the conclusions of Gatt et al., [11] noted that while Vitamin D supplementation did not alter final union rates, it did not adversely affect healing biology either. Importantly, the biochemical improvements observed in the present study translated into clinically meaningful differences in fracture healing time. The mean radiological time to union was significantly shorter in the weekly supplementation group (15.9 ± 2.8 weeks) compared to the daily group (18.6 ± 3.2 weeks; P = 0.002). This finding is particularly relevant when interpreted alongside the observational data from Memon et al., [12] demonstrated that patients with sufficient baseline Vitamin D levels healed significantly faster (14.8 ± 2.9 weeks) than those who were insufficient (16.7 ± 3.2 weeks) or deficient (17.9 ± 3.9 weeks), with Vitamin D levels emerging as an independent predictor of healing time (β = −0.41; P < 0.001) [5]. The healing times observed in the weekly supplementation group in the present study closely approximate those reported in Vitamin D–sufficient patients in Memon et al.’s cohort, further supporting the role of adequate Vitamin D status in accelerating fracture repair.
At 24 weeks, radiological union was achieved in 96% of patients in the weekly supplementation group compared to 84% in the daily group, with fewer cases of delayed union (4% vs. 16%). Although this difference did not reach statistical significance, likely due to the limited sample size, the observed trend is consistent with the post hoc findings of Slobogean et al., [13] where high-dose Vitamin D3 supplementation was associated with modest improvements in clinical fracture healing scores compared to placebo at 3 months and over 12 months. The lack of statistically significant differences in pre-specified outcomes in the Vita Shock trial and in the systematic review by Gatt et al. [11] highlights the complexity of demonstrating fracture healing benefits in randomized trials, particularly when fracture healing is influenced by multiple mechanical, biological, and patient-related factors. However, the present study differs in that it specifically targeted a Vitamin D–deficient population and compared two active supplementation regimens rather than a placebo, which may explain the clearer differences observed in healing time.
When compared with broader skeletal outcomes, the findings of the present study are also consistent with the conclusions of LeBoff et al. [14] from the VITAL trial, which demonstrated that Vitamin D3 supplementation at 2000 IU/day did not improve bone mineral density or structure in generally healthy adults not selected for Vitamin D insufficiency. This underscores the importance of baseline Vitamin D status in determining the potential benefit of supplementation. In contrast, the present study enrolled patients with confirmed Vitamin D deficiency and demonstrated improvements in fracture healing parameters, supporting the notion that targeted supplementation in deficient individuals may yield clinical benefits not observed in unselected populations. Furthermore, Kong et al.’s [15] meta-analysis reported that daily Vitamin D doses of 800–1000 IU were most effective in reducing fracture and fall risk, while intermittent dosing was not beneficial for fall prevention. While this contrasts with the present study’s finding of superior outcomes with weekly dosing, it is important to note that Kong et al. focused on fracture prevention and falls rather than fracture healing, and their conclusions pertain to population-level risk reduction rather than post-fracture biological repair processes.
Overall, the findings of the present study suggest that correction of Vitamin D deficiency, particularly using a weekly high-dose regimen, is associated with faster radiological fracture union, improved biochemical profiles, and a lower incidence of delayed healing in patients with long-bone fractures. While previous randomized trials and systematic reviews have reported mixed or inconclusive results regarding Vitamin D supplementation and fracture healing, the present study supports the growing body of observational evidence demonstrating a strong association between Vitamin D status and healing time. These results emphasize the importance of routine screening for Vitamin D deficiency in fracture patients and suggest that appropriately dosed supplementation may serve as a valuable adjunct to standard orthopedic management. Larger multicenter trials with sufficient power are warranted to confirm these findings and to establish evidence-based supplementation protocols tailored to fracture patients with documented Vitamin D deficiency.
The present study has certain limitations that must be acknowledged. The relatively small sample size (n = 50) limits statistical power and may restrict the generalizability of the findings, particularly for subgroup analyses, such as delayed union rates. Being a single-center study conducted at a tertiary care institution, the results may not be fully representative of diverse geographic, ethnic, or healthcare settings. The follow-up duration of 24 weeks, although adequate for early union assessment, may not capture long-term remodeling outcomes or late complications. Inclusion of heterogeneous long-bone fractures (femur, tibia, humerus, radius, and ulna) and variation in management modalities (operative and conservative) could introduce biological and mechanical variability influencing healing dynamics. The absence of double blinding raises the possibility of performance and assessment bias, and the lack of a true placebo or non-supplemented control group precludes evaluation of the independent effect of Vitamin D versus no supplementation. Functional outcome measures, such as disabilities of the arm, shoulder, and hand, lower extremity functional scale, or SF-36 (Short Form (36) Health Survey) were not incorporated, limiting assessment of patient-reported recovery. In addition, advanced bone turnover markers (e.g., osteocalcin, CTX (C-terminal telopeptide), P1NP (Procollagen type I N-terminal propeptide)) were not evaluated, and compliance with supplementation was not objectively verified through pill counts or interim serum monitoring. Concomitant calcium supplementation may have acted as a confounder, and baseline nutritional factors, BMI stratification, and sunlight exposure were not rigorously quantified. Radiological union was assessed using plain radiographs without advanced imaging, such as computed tomography scan, which may introduce interobserver variability. Finally, although no serious adverse events were observed, longer-term safety evaluation of high-dose Vitamin D regimens, including monitoring for hypercalcemia and altered bone turnover, would strengthen future research.
This prospective randomized study demonstrated that correction of Vitamin D deficiency plays a meaningful role in optimizing fracture healing in patients with long-bone fractures. Both daily low-dose and weekly high-dose Vitamin D supplementation significantly improved serum Vitamin D levels and bone-related biochemical markers; however, weekly high-dose supplementation achieved superior biochemical correction and was associated with a significantly shorter time to radiological fracture union. The observed improvements in serum calcium levels and suppression of PTH further indicate enhanced bone metabolic balance in patients receiving weekly supplementation. Importantly, the weekly regimen was well tolerated and did not result in clinically significant adverse effects. These findings support the routine screening for Vitamin D deficiency in fracture patients and suggest that a weekly high-dose Vitamin D supplementation strategy may be a more effective adjunct to standard fracture management in Vitamin D–deficient individuals, with the potential to accelerate healing and improve overall clinical outcomes.
Routine screening and correction of Vitamin D deficiency should be considered in patients with long-bone fractures. Weekly high-dose Vitamin D supplementation may accelerate fracture healing and improve biochemical recovery when used as an adjunct to standard fracture management.
References
- 1. Dodd AC, Salib CG, Lakomkin N, Obremskey WT, Sethi MK. Increased risk of adverse events in management of femur and tibial shaft fractures with plating: An analysis of NSQIP data. J Clin Orthop Trauma 2016;7:80-5. [Google Scholar] [PubMed]
- 2. SPRINT Investigators, Bhandari M, Guyatt G, Tornetta P 3rd, Schemitsch E, Swiontkowski M, et al. Study to prospectively evaluate reamed intramedually nails in patients with tibial fractures (S.P.R.I.N.T.): Study rationale and design. BMC Musculoskelet Disord 2008;9:91. [Google Scholar] [PubMed]
- 3. Forster MC, Aster AS, Ahmed S. Reaming during anterograde femoral nailing: Is it worth it? Injury 2005;36:445-9. [Google Scholar] [PubMed]
- 4. Lin CA, Swiontkowski M, Bhandari M, Walter SD, Schemitsch EH, Sanders D, et al. Reaming does not affect functional outcomes after open and closed tibial shaft fractures: The results of a randomized controlled trial. J Orthop Trauma 2016;30:142-8. [Google Scholar] [PubMed]
- 5. Sprague S, Petrisor B, Scott T, Devji T, Phillips M, Spurr H, et al. What is the role of vitamin D supplementation in acute fracture patients? A systematic review and meta-analysis of the prevalence of hypovitaminosis D and supplementation efficacy. J Orthop Trauma 2016;30:53-63. [Google Scholar] [PubMed]
- 6. Sprague S, Bzovsky S, Scott T, Slobogean G. Vitamin D use in orthopaedics. COA Bull 2017;118:32-5. [Google Scholar] [PubMed]
- 7. Lidor C, Dekel S, Hallel T, Edelstein S. Levels of active metabolites of vitamin D3 in the callus of fracture repair in chicks. J Bone Jt Surg Br 1987;69:132-6. [Google Scholar] [PubMed]
- 8. Omeroğlu H, Ateş Y, Akkuş O, Korkusuz F, Biçimoğlu A, Akkaş N. Biomechanical analysis of the effects of single high-dose vitamin D3 on fracture healing in a healthy rabbit model. Arch Orthop Trauma Surg 1997;116:271-4. [Google Scholar] [PubMed]
- 9. Omeroğlu S, Erdoğan D, Omeroğlu H. Effects of single high-dose vitamin D3 on fracture healing. An ultrastructural study in healthy Guinea pigs. Arch Orthop Trauma Surg 1997;116:37-40. [Google Scholar] [PubMed]
- 10. Bee CR, Sheerin DV, Wuest TK, Fitzpatrick DC. Serum vitamin D levels in orthopaedic trauma patients living in the northwestern United States. J Orthop Trauma 2013;27:e103-6. [Google Scholar] [PubMed]
- 11. Gatt T, Grech A, Arshad H. The effect of vitamin D supplementation for bone healing in fracture patients: A systematic review. Adv Orthop 2023;2023:6236045. [Google Scholar] [PubMed]
- 12. Memon R, Raj P, Sheoran M, Singh SK, Kamra P. Correlation between vitamin D levels and healing time in lower limb fractures. J Orthop Case Rep 2025;15:379-85. [Google Scholar] [PubMed]
- 13. Slobogean GP, Bzovsky S, O’Hara NN, Marchand LS, Hannan ZD, Demyanovich HK, et al. Effect of vitamin D3 supplementation on acute fracture healing: A phase II screening randomized double-blind controlled trial. JBMR Plus 2023;7:e10705. [Google Scholar] [PubMed]
- 14. LeBoff MS, Chou SH, Murata EM, Donlon CM, Cook NR, Mora S, et al. Effects of supplemental vitamin D on bone health outcomes in women and men in the VITamin D and OmegAd OTriaL (VITAL). J Bone Miner Res 2020;35:883-93. [Google Scholar] [PubMed]
- 15. Kong SH, Jang HN, Kim JH, Kim SW, Shin CS. Effect of vitamin D supplementation on risk of fractures and falls according to dosage and interval: A meta-analysis. Endocrinol Metab (Seoul) 2022;37:344-58. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures
May 1, 2026 The Impact of Medial Cortical Reduction on the Outcomes of Fixation in Unstable Intertrochanteric Fractures October 1, 2025 Correlation between Vitamin D Levels and Healing Time in Lower Limb Fractures
October 1, 2025 Correlation between Vitamin D Levels and Healing Time in Lower Limb Fractures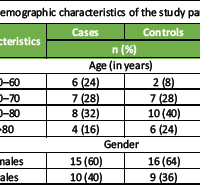 September 1, 2025 Effect of Teriparatide in Fracture Healing in Elderly
September 1, 2025 Effect of Teriparatide in Fracture Healing in Elderly