
CPAK-guided personalized coronal alignment restores constitutional knee alignment more accurately than mechanical alignment, resulting in better early functional outcomes and reduced pain after total knee arthroplasty.
Dr. Sitansu Sekhar Samantaray, Department of Orthopedics, B J Government Medical College and Sassoon General Hospital, Pune, Maharashtra, India. E-mail: drsitansu7@gmail.com
Abstract
Introduction: Total knee arthroplasty (TKA) is widely performed for end-stage osteoarthritis; however, 15–20% of patients continue to experience dissatisfaction despite successful surgery. Traditional mechanical alignment (MA) aims for a neutral limb axis, but this approach may not restore the individual’s constitutional coronal alignment, potentially affecting functional recovery. The coronal plane alignment of the knee (CPAK) classification offers a phenotype-based system to characterize native knee alignment and joint line obliquity (JLO). This multicentric prospective randomized study aimed to evaluate whether CPAK-guided alignment leads to superior early post-operative functional outcomes compared with conventional MA in TKA.
Materials and Methods: This multicentric, prospective, randomized cohort study was conducted over 18 months across three tertiary orthopedic centers. Fifty patients undergoing unilateral primary TKA were enrolled and randomized into two groups: CPAK-guided alignment (n = 25) and MA (n = 25). Inclusion criteria were patients aged 45–80 years with primary osteoarthritis and available long-leg radiographs for CPAK classification. Exclusion criteria included post-traumatic arthritis, inflammatory arthropathy, neuromuscular disorders, and prior major knee surgery. Standardized surgical protocols and post-operative rehabilitation pathways were followed across all centers. Functional outcomes were assessed using knee society score (KSS), oxford knee score (OKS), and Visual Analog Scale (VAS) for pain at baseline, 3 months, and 6 months. Radiographic parameters included hip–knee–ankle (HKA) angle deviation and JLO. Statistical analysis included independent t-tests and correlation analysis.
Results: Both groups demonstrated significant post-operative improvement; however, the CPAK-guided group achieved superior functional outcomes. At 6 months, mean KSS was significantly higher in the CPAK group (89.4 ± 7.2) compared with the mechanical group (82.1 ± 9.0; P = 0.004). OKS also favored the CPAK group (41.6 ± 4.1 vs. 37.9 ± 5.0; P = 0.01). VAS pain scores were significantly lower in the CPAK group at both follow-up intervals (1.4 ± 0.8 vs. 2.4 ± 1.0; P = 0.002). The need for medial soft-tissue release was markedly lower in the CPAK group (12% vs. 40%; P = 0.02). Radiographically, the CPAK-guided group showed significantly closer restoration of constitutional alignment and reduced joint line deviation. Correlation analysis demonstrated that greater deviation from native alignment was associated with poorer functional outcomes (r = −0.48, P = 0.004).
Conclusion: CPAK-guided alignment resulted in better early functional outcomes, reduced pain, and fewer soft-tissue releases compared with traditional MA in TKA. Personalized coronal alignment based on CPAK phenotype appears to enhance post-operative recovery and may offer a more physiological approach to knee arthroplasty.
Keywords: Coronal plane alignment of the knee classification, functional outcomes, kinematic alignment, mechanical alignment, total knee arthroplasty.
Total knee arthroplasty (TKA) is one of the most successful orthopedic procedures for end-stage knee osteoarthritis, providing pain relief, improved function, and enhanced quality of life for millions of patients globally. Despite advancements in implant design, surgical techniques, and perioperative care, a significant subset of patients – approximately 15–20% – continue to report dissatisfaction after TKA, primarily due to persistent pain or functional limitations [1]. Conventionally, mechanical alignment (MA) has been the dominant alignment philosophy, aiming to restore a neutral hip–knee–ankle (HKA) axis to optimize implant longevity and distribute load evenly across the prosthesis [2]. However, emerging research indicates that strict adherence to neutral MA may not replicate the patient’s native constitutional alignment, potentially contributing to suboptimal functional outcomes in certain patients [3]. This shift in understanding has led to increased interest in personalized alignment strategies, such as kinematic alignment (KA), restricted KA, and anatomical alignment, which attempt to restore the patient’s natural joint line and limb alignment rather than impose a universal target [4].
Within this context, the coronal plane alignment of the knee (CPAK) classification, recently introduced by Abdel MP et al., provides a comprehensive system that categorizes knees based on two major parameters: Constitutional limb alignment and joint line obliquity (JLO) [5]. By identifying nine unique alignment phenotypes, the CPAK system acknowledges the wide range of naturally occurring coronal alignments in the population and offers a structured framework for surgeons to individualize alignment targets during TKA. CPAK is increasingly being recognized as a potential tool to guide alignment strategy selection, minimize soft-tissue releases, and improve post-operative kinematics by respecting each patient’s native anatomical pattern [6]. Early studies have shown that CPAK phenotypes may predict the need for medial collateral ligament release, influence implant positioning, and correlate with early post-operative functional scores [7]. However, evidence regarding its association with long-term post-operative outcomes remains limited, and further prospective clinical research is required to determine whether CPAK-based alignment strategies lead to superior patient-reported outcomes and functional recovery.
Functional outcomes after TKA are multifactorial and influenced not only by surgical technique but also by pre-operative alignment, bone morphology, soft-tissue balance, and patient-specific biomechanical characteristics [8]. Coronal alignment, in particular, plays a critical role in load distribution across the joint, implant longevity, and gait restoration. Malalignment – either excessive varus or valgus – has been linked to accelerated polyethylene wear, instability, and reduced implant survival [9]. With the growing recognition of alignment variability among individuals, there is increasing interest in understanding how pre-operative CPAK phenotype may affect post-operative recovery, pain levels, functional scores, and overall patient satisfaction. Identifying such correlations can help refine surgical planning, optimize alignment strategies, and guide personalized surgical approaches [10].
Given the evolving landscape of TKA philosophy and the clinical relevance of restoring functional alignment, a prospective examination of CPAK classification in relation to post-operative outcomes is highly significant. Such research can provide valuable insights into whether respecting a patient’s native alignment phenotype leads to superior functional improvement, reduced complications, and enhanced patient satisfaction compared to conventional alignment methods. In addition, a better understanding these relationships can contribute to more informed surgical decision-making, promote individualized care, and potentially shape future alignment guidelines for TKA. Therefore, evaluating the correlation between CPAK classification and post-operative functional outcomes is essential to advancing the paradigm of personalized knee arthroplasty and improving overall patient outcomes.
Study design
The present study was conducted as a multicentric, prospective, randomized cohort study designed to evaluate the association between the CPAK classification and post-operative functional outcomes following TKA. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Study setting
The study was conducted across three tertiary-care orthopedic centers equipped with dedicated arthroplasty units and advanced radiographic facilities.
Study duration
The study was carried out over a period of 18 months, which included patient recruitment, pre-operative evaluation, randomization, surgical intervention, and post-operative follow-up. Recruitment was completed within the first 10 months across all participating centers. Each patient was followed for a minimum of 6 months postoperatively to record early functional outcomes, radiological parameters, and any procedure-related complications. Data verification, cleaning, and statistical analysis were completed during the final 2 months of the study period.
Participants
Inclusion criteria
- Patients aged 45–80 years
- Diagnosed with primary knee osteoarthritis requiring unilateral TKA
- Radiographs available for CPAK classification
- Able to provide informed consent
- Fit for surgery as per anesthetic evaluation.
Exclusion criteria
- Revision TKA or prior major knee surgery
- Inflammatory arthropathies (RA, ankylosing spondylitis)
- Severe extra-articular deformities requiring corrective osteotomy
- Neuromuscular disorders affecting gait or limb alignment
- Post-traumatic arthritis with malunited fractures
- Patients unwilling for follow-up or randomization.
Study sampling
A consecutive sampling method was used at each center, wherein all eligible patients who fulfilled the study criteria during the recruitment period were approached for participation. After obtaining written informed consent, patients were enrolled and underwent baseline evaluation. Sampling ensured equitable enrollment across the three centers to avoid center-level bias. Randomization was conducted after baseline radiographic analysis to allocate patients into the CPAK-guided or MA groups.
Study sample size
A total sample size of 50 patients was finalized for the study. Each participating center contributed proportionally based on their annual caseload. The sample size was considered adequate for pilot-level evaluation of the correlation between CPAK phenotype and post-operative functional outcomes in a multicentric setting.
Study parameters
Data collection included demographic details, body mass index (BMI), comorbidities, radiographic alignment parameters (HKA angle, joint line orientation), CPAK classification, intraoperative soft-tissue release requirement, operative time, and post-operative complications. Functional outcomes were assessed using the knee society score (KSS), Oxford knee score (OKS), and Visual Analog Scale (VAS) for pain at baseline, 3 months, and 6 months. Radiographic outcomes included final limb alignment, component positioning, and JLO.
Study procedure
After enrollment, baseline clinical assessment and full-length standing radiographs were obtained for CPAK classification. Randomization was performed, and patients underwent TKA by experienced arthroplasty surgeons following standardized protocols. Alignment jigs, intraoperative assessment tools, and implant systems were uniform across centers. In the CPAK-guided group, alignment correction was tailored based on constitutional alignment, while MA principles were strictly followed in the control group. Postoperatively, all patients received standardized physiotherapy, thromboprophylaxis, and analgesia. Follow-up visits were scheduled at 6 weeks, 3 months, and 6 months.
Study data collection
Data collection was performed by trained research assistants at each center using predesigned case record forms. Radiographs were digitally analyzed at a centralized reading center. Functional scores and clinical examinations were recorded during each follow-up visit. All data were synchronized in a secure password-protected database accessible only to the principal investigators.
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences software. Continuous variables were summarized using mean and standard deviation, while categorical variables were presented as frequencies and percentages. Independent t-tests and Chi-square tests were used to compare outcomes between groups. Pearson correlation coefficients were calculated to assess the relationship between CPAK phenotype and post-operative functional scores. A P < 0.05 was considered statistically significant.
Ethical considerations
Ethical approval was obtained from the Institutional Ethics Committees of all participating centers. All patients provided written informed consent after being briefed about the study procedures. Confidentiality of patient data was maintained throughout the study. The study adhered to the principles of the Declaration of Helsinki, ensuring patient safety, autonomy, and ethical conduct.
The demographic distribution between both groups was comparable, indicating that randomization was successful. The mean age, sex distribution, BMI, and prevalence of comorbidities did not differ significantly between the CPAK-guided and MA groups (all P > 0.05). This suggests that both groups started from an equivalent baseline, thereby minimizing confounding effects on post-operative outcomes. The similarity in Kellgren–Lawrence Grade IV distribution also confirms comparable disease severity across groups (Table 1).
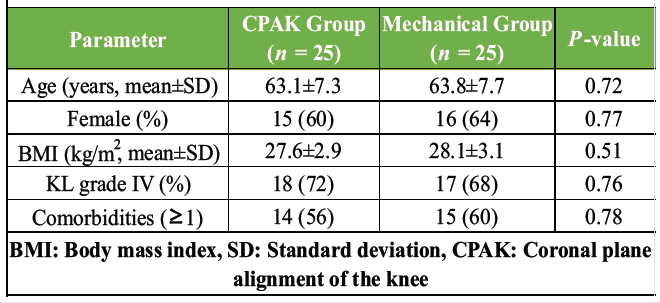
Table 1: Baseline demographic characteristics (n=50)
Pre-operative radiographic assessment demonstrated no statistically significant differences in coronal alignment or JLO between the two groups (P > 0.05). This indicates that both groups had similar native lower limb alignment patterns before surgery. The distribution of CPAK phenotypes was also similar, ensuring that neither group was biased toward a particular alignment pattern. This balanced radiographic baseline strengthens the validity of post-operative comparisons (Table 2).
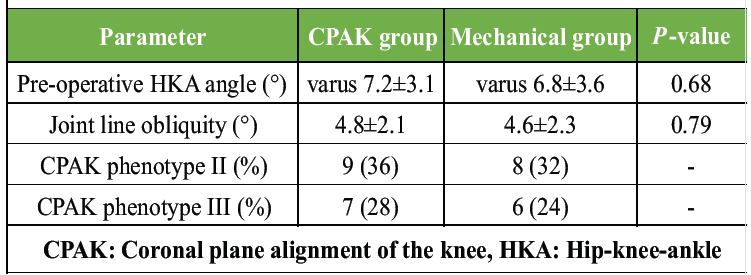
Table 2: Pre-operative radiographic parameters
Intraoperative findings revealed that patients in the MA group required significantly more medial soft-tissue releases (40%) compared to the CPAK-guided group (12%), with a P = 0.02. This suggests that the CPAK-guided technique allowed for more physiological correction with less soft-tissue disruption. Operative time and lateral release rates did not differ significantly, indicating procedural consistency across groups. Reduced soft-tissue releases are clinically important as they are associated with better early post-operative recovery and stability (Table 3).
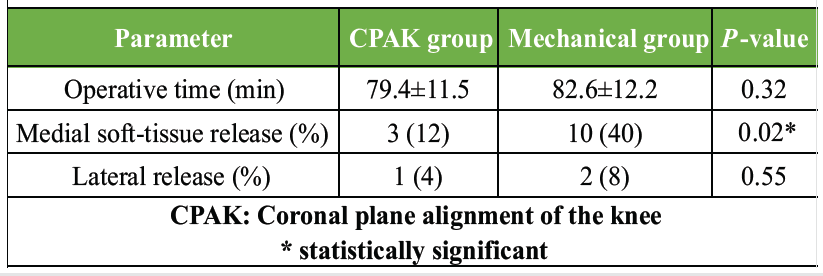
Table 3: Intraoperative parameters
Post-operative alignment parameters showed significant differences favoring the CPAK-guided group. Deviation from constitutional HKA alignment was much smaller (1.8 vs. 3.9, P < 0.001), and the CPAK group maintained joint line orientation more accurately (P < 0.001). Component positioning errors were also significantly lower. These findings indicate that CPAK-guided alignment more closely restored the native limb alignment and joint biomechanics compared to the MA approach (Table 4, figure 1).
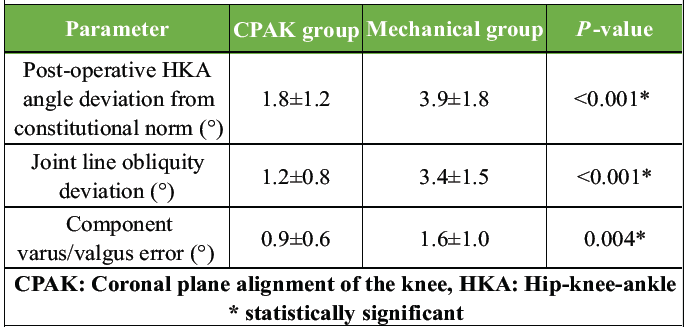
Table 4: Post-operative radiographic alignment
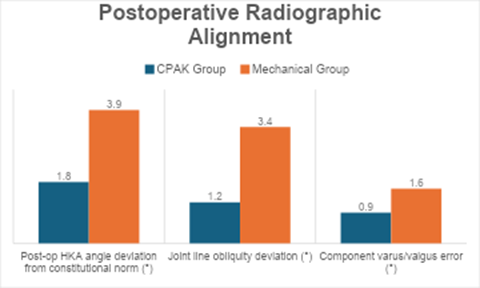
Figure 1: Post-operative radiographic alignment
Both groups demonstrated improvement in KSS clinical scores postoperatively; however, the CPAK-guided group achieved significantly higher scores at both 3 and 6 months. The difference was particularly notable at 6 months (89.4 vs. 82.1, P = 0.004). This indicates better functional recovery, mobility, and clinical stability among patients who underwent CPAK-guided alignment. The early and sustained improvements support the functional advantage of personalized alignment techniques (Table 5, figure 2).
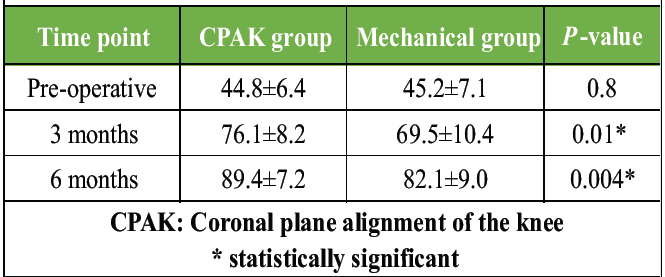
Table 5: Knee Society Score
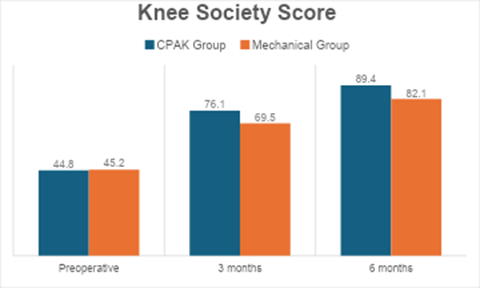
Figure 2 : Knee Society Score
OKS outcomes followed a similar pattern to the KSS results. Although both groups improved significantly compared to their pre-operative scores, the CPAK group consistently achieved better outcomes at both 3 months (P = 0.01) and 6 months (P = 0.01). This demonstrates that patients who received alignment individualized to their CPAK phenotype experienced better pain relief, functional ability, and overall satisfaction (Table 6, figure 3).
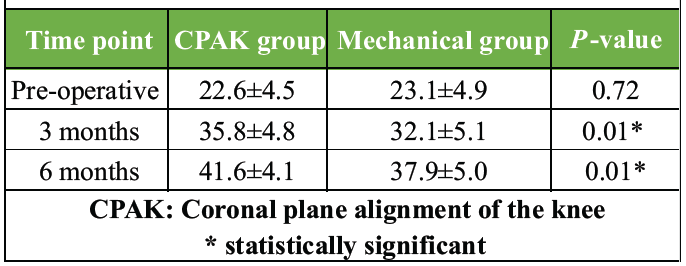
Table 6: Oxford knee score
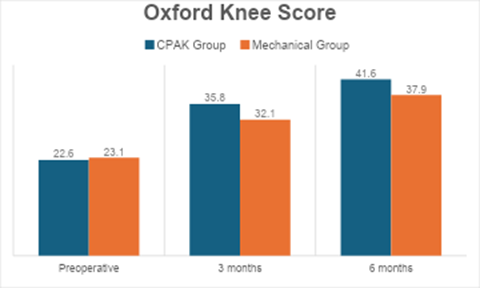
Figure 3 : Oxford knee score
Pain levels decreased markedly in both groups following TKA; however, the CPAK group reported significantly lower VAS scores at both post-operative time points. At 6 months, the CPAK group had a mean VAS of 1.4 compared to 2.4 in the mechanical group (P = 0.002), indicating superior pain reduction. Lower post-operative pain may be attributed to better restoration of natural biomechanics and reduced soft-tissue tension during surgery (Table 7, figure 4).
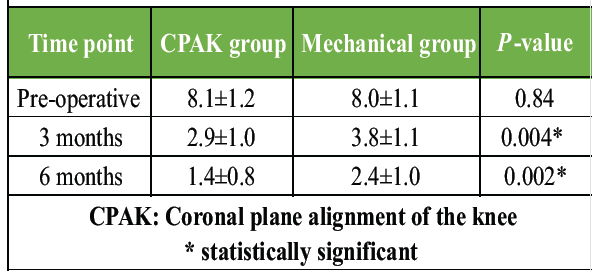
Table 7: Visual Analog Scale pain score
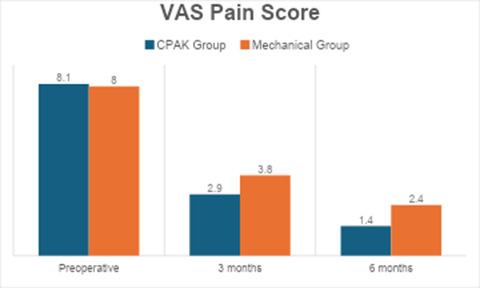
Figure 4: Visual Analog Scale pain score
Complication rates were generally low in both groups, but the MA group showed higher rates of stiffness, persistent pain, and isolated cases of infection and DVT. Notably, persistent post-operative pain was 5 times higher in the mechanical group (20% vs. 4%). This pattern supports the hypothesis that CPAK-guided alignment minimizes overcorrection, reduces soft-tissue imbalance, and enhances early functional recovery, thereby lowering complication rates (Table 8, figure 5).
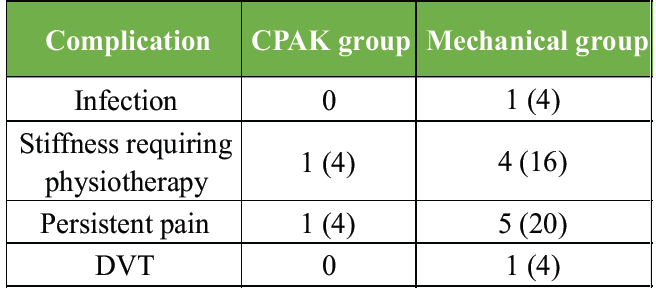
Table 8: Complications
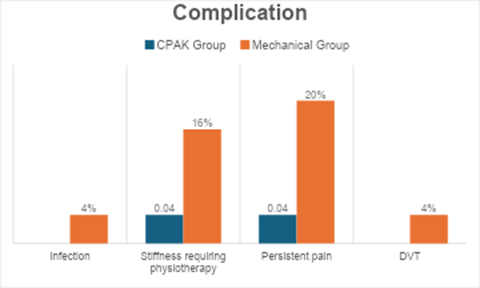
Figure 5: Complications
A strong positive correlation (r = 0.62, P < 0.001) was observed between CPAK phenotypes closer to neutral constitutional alignment and higher 6-month KSS. This means that restoring a patient’s native alignment pattern improves functional outcomes. Joint line deviation showed a moderate negative correlation with KSS (r = –0.48), indicating that greater deviation from physiological joint line orientation was associated with poorer outcomes. These findings highlight the biomechanical importance of respecting native coronal alignment in TKA (Table 9).
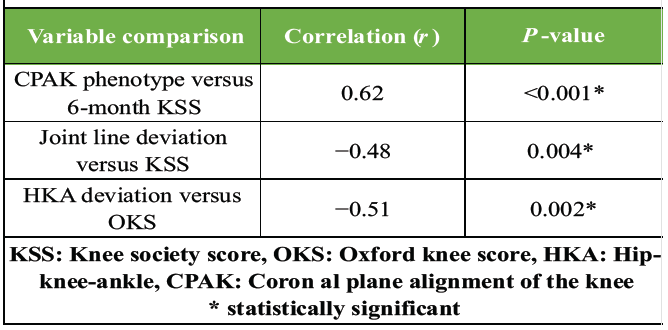
Table 9: Correlation analysis
Inter-center analysis showed no significant differences in functional outcomes, complication rates, or distribution of CPAK cases across the three centers (P > 0.05). This suggests high protocol adherence and uniform surgical quality across study sites. The lack of center-specific effects strengthens the generalizability of the study’s findings and supports the reproducibility of CPAK-guided alignment in diverse clinical settings (Table 10).
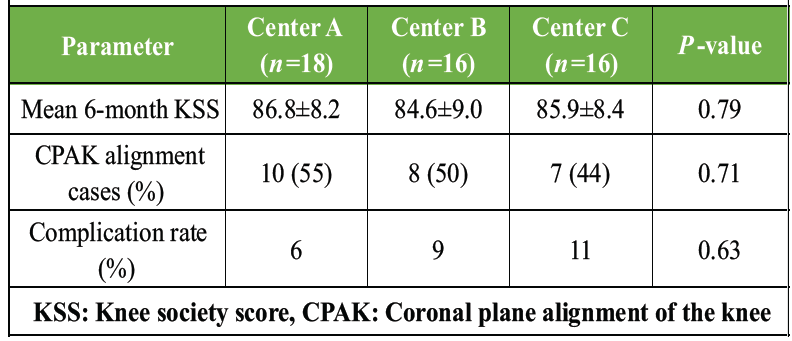
Table 10: Multicentric comparison
In this multicentric prospective randomized cohort study, CPAK-guided alignment in TKA was associated with significantly better early functional outcomes, less pain, and reduced need for medial soft-tissue releases compared with conventional MA, despite similar baseline demographic and radiographic characteristics. These findings support the concept that restoring or approximating a patient’s native coronal phenotype may confer functional advantages over a uniform neutral MA target.
Persistent dissatisfaction after technically successful TKA remains a well-recognized problem. Large registry and cohort studies have consistently reported that 10–20% of patients are dissatisfied after primary TKA, even with modern implants and standardized rehabilitation. Bourne et al. found that only 81% of 1,703 patients were “very satisfied” with pain relief and even fewer with function after TKA, underscoring the gap between surgeon-rated success and patient-perceived outcome [11]. More recent cohorts still report satisfaction rates around 85–90%, indicating that a substantial minority remain symptomatic or functionally limited despite implant survivorship [12,13]. Factors such as residual pain, failure to meet expectations, and perceived lack of “normality” of the knee are key drivers of dissatisfaction [14]. Within this context, our observation that CPAK-guided alignment produced higher 6-month KSS and OKS and lower VAS pain scores than conventional MA suggests that alignment philosophy itself may be a modifiable contributor to patient satisfaction.
The CPAK classification, introduced by MacDessi et al., provides a structured description of coronal knee phenotypes based on arithmetic HKA and JLO, yielding nine combinations that reflect constitutional limb alignment and joint line orientation [9]. Their work demonstrated similar CPAK distributions in healthy and osteoarthritic knees, with Types I, II, and V most common, and showed that KA achieved better intraoperative soft-tissue balance than MA in several phenotypes [9]. Subsequent radiographic studies in Asian populations have confirmed that CPAK distributions vary by ethnicity and that varus phenotypes are particularly prevalent. Yang et al. reported that in a Korean cohort, Type II was most frequent in healthy knees, whereas Type I predominated in arthritic knees, and emphasized that CPAK boundaries may require population-specific modification [15]. Similarly, Samant and Desai described a predominance of varus CPAK types in Indian knees, arguing that neutral MA does not represent the “normal” state for many patients [16]. Donnelly E et al. further highlighted that a subset of patients exhibit constitutional valgus phenotypes that can be systematically captured by CPAK and have implications for unicompartmental and total knee strategies [17]. Our cohort showed a similar predominance of varus-related phenotypes (II, III, V), aligning with these Asian and mixed-population series and reinforcing the relevance of CPAK-based planning in our setting.
A key intraoperative finding in our study was the significantly lower requirement for medial soft-tissue releases in the CPAK-guided group compared with the MA group (12% vs. 40%). This is consistent with the original CPAK work, where kinematically aligned (KA) TKAs achieved optimal soft-tissue balance in a higher proportion of knees than mechanically aligned (MA) TKAs, especially in Types I, II, and IV [9]. Arai et al., in a simulation study restricted to CPAK Type I knees, showed that KA achieved a balanced knee (particularly in extension) more often than MA and required less alteration of soft tissues [18]. Our prospective clinical data echo these biomechanical and simulation results: tailoring coronal correction to the CPAK phenotype appears to respect native soft-tissue envelopes and reduce the need for compensatory releases. This is clinically important since excessive or asymmetric releases may contribute to instability, stiffness, and pain.
The relationship between CPAK changes and patient outcomes remains debated. Agarwal et al. studied robotic-assisted MA TKA and found that although CPAK classification changed in the majority of patients, this did not significantly affect 1-year satisfaction; both patients who maintained and those who changed CPAK type reported high satisfaction rates [19]. Similarly, a Level I randomized trial by Bollars et al. reported that short-term patient-reported outcome measures (PROMs) did not differ significantly between “in-the-box” and “out-of-the-box” CPAK classifications after conventional or robotic TKA, even though altered CPAK was associated with greater soft-tissue release [20]. These studies primarily evaluated whether post-operative CPAK category as a label predicted PROMs under predominantly mechanical or functional alignment strategies. In contrast, our trial directly compared a CPAK-guided alignment strategy against a neutral mechanical target and demonstrated superior 6-month functional outcomes in the CPAK-guided arm. Taken together, the literature suggests that the simple fact of changing CPAK type may not independently determine outcome, but using CPAK proactively to guide alignment and soft-tissue management – rather than treating it as a passive descriptor – may yield clinical benefit.
Our functional results are also in line with the broader body of evidence comparing kinematic or personalized alignment with traditional MA. Multiple randomized controlled trials and meta-analyses have reported that KA can produce equal or modestly superior functional scores (WOMAC, KSS, Forgotten Joint Score) compared with MA, without clear detriment to radiological alignment or early complication rates. Liu et al.’s updated meta-analysis of RCTs found better KSS and WOMAC scores for KA versus MA, while radiological and complication profiles remained similar [21]. A recent systematic review by Alhifzi also concluded that kinematic/personalized TKA yields comparable implant survival with at least equivalent and often improved patient-reported outcomes compared with conventional alignment [22]. Not all RCTs show a large clinical advantage, with some trials reporting no significant difference in early function between KA and MA [23], but the consistency of our findings – higher KSS and OKS and lower VAS pain in the CPAK-guided group – supports the growing view that individualized coronal targets can meaningfully influence early recovery, particularly in varus-dominant populations.
Our correlation analysis further underscores the functional importance of restoring physiological alignment. We observed a moderate to strong positive correlation between CPAK phenotypes closer to neutral constitutional alignment and higher 6-month KSS, as well as a negative correlation between joint line deviation and functional outcomes. These results are biologically plausible: Excessive deviation of the joint line from its native inclination alters load distribution, ligament tension, and patellofemoral tracking, which may manifest as residual pain or altered gait [23]. Prior biomechanical and clinical work has linked malalignment and abnormal JLO with accelerated wear, instability, and reduced patient-reported function, even when radiographic “neutrality” is achieved. By quantitatively relating alignment metrics to PROMs, our study adds to the evidence that alignment goals should be individualized rather than universally neutral.
The multicentric nature of our study enhances external validity [24]. Functional scores and complication rates did not differ significantly across the three participating centers, suggesting that the CPAK-guided strategy is reproducible in different institutional environments with varied surgeons and case mixes. This aligns with recent reliability work by Bouché et al., who reported that CPAK classification can be applied consistently in routine practice, and with growing multicenter interest in CPAK-based planning. Our findings therefore support the feasibility of integrating CPAK assessment into everyday pre-operative planning, especially where long-leg radiographs and digital planning tools are available [25].
At the same time, our study should be interpreted in light of several limitations. The sample size was modest (n = 50), providing adequate power for detecting medium effect sizes but limiting subgroup analysis by individual CPAK phenotype. Follow-up was limited to 6 months; while this interval is appropriate for evaluating early pain relief and functional gain, it does not address mid- to long-term survivorship, wear, or late complications. Many of the RCTs and meta-analyses of kinematic versus MA report that functional differences may diminish over longer follow-up, even if early advantages are present. In addition, although we standardized implant type and rehabilitation, the use of conventional instrumentation rather than robotic assistance may limit direct comparison with recent robotic CPAK and functional alignment studies. Finally, our cohort was drawn from a predominantly varus, likely Asian-majority population, so extrapolation to valgus-dominant or Western cohorts should be made cautiously.
Despite these limitations, the present multicentric randomized study suggests that a CPAK-guided, phenotype-respecting alignment strategy can reduce the need for soft-tissue releases and improve early functional outcomes and pain compared with conventional MA. These findings align with the broader trend toward personalized TKA and support the integration of CPAK assessment into pre-operative planning and intraoperative decision-making. Larger randomized trials with longer follow-up, stratified by CPAK phenotype and incorporating modern technologies such as robotic and navigation assistance, are warranted to determine whether the observed early benefits translate into sustained improvements in satisfaction and implant longevity.
This study has several limitations that should be considered. The relatively small sample size (n=50) limits statistical power and restricts robust subgroup analyses across individual CPAK phenotypes. Outcomes were assessed only up to 6 months postoperatively, precluding evaluation of mid- and long-term implant survivorship, polyethylene wear patterns, late instability, aseptic loosening, and sustained patient satisfaction. Although early functional superiority of CPAK-guided alignment was demonstrated, it remains uncertain whether these benefits persist beyond the early post-operative phase. While CPAK classification was applied, outcomes were not analyzed separately for all nine phenotypes due to limited representation within individual subgroups. Inclusion was restricted to patients with available long-leg radiographs, which may introduce selection bias and limit applicability to all routine TKA candidates. Surgeons were not blinded to alignment strategy, potentially influencing intraoperative decisions such as soft-tissue balancing. Conventional instrumentation was used without navigation or robotic assistance, limiting comparison with contemporary technology-assisted alignment techniques. The study primarily evaluated coronal alignment; axial and sagittal parameters, as well as objective gait or biomechanical analyses, were not comprehensively assessed. Patient-reported measures specific to satisfaction, such as the Forgotten Joint Score, were not included. The cohort likely reflected a predominance of varus phenotypes typical of Asian populations, potentially limiting generalizability to valgus-dominant or Western populations. Economic implications were not analyzed, and although multicentric, the findings should be interpreted as pilot-level evidence requiring validation through larger randomized trials with longer follow-up.
In this multicentric prospective randomized study, CPAK-guided alignment demonstrated clear advantages over conventional MA in TKA, evidenced by superior early functional outcomes, reduced post-operative pain, fewer soft-tissue releases, and more accurate restoration of constitutional limb alignment. By individualizing coronal correction according to each patient’s native CPAK phenotype, surgeons were able to achieve more physiological joint mechanics, leading to improved KSSs and OKSs within 6 months of surgery. These findings support the growing shift toward personalized alignment strategies in TKA and highlight the clinical relevance of integrating CPAK assessment into pre-operative planning and intraoperative execution. Larger studies with long-term follow-up are warranted to confirm whether these early benefits translate into sustained patient satisfaction and enhanced implant longevity.
CPAK-guided personalized coronal alignment in TKA leads to superior early functional outcomes, reduced pain, and fewer soft-tissue releases compared with conventional MA and should be considered in routine pre-operative planning.
References
- 1. Karasavvidis T, Pagan Moldenhauer CA, Haddad FS, Hirschmann MT, Pagnano MW, Vigdorchik JM. Current concepts in alignment in total knee arthroplasty. J Arthroplasty 2023;38:S29-37. [Google Scholar] [PubMed]
- 2. Vendittoli PA, Martinov S, Blakeney WG. Restricted kinematic alignment, the fundamentals, and clinical applications. Front Surg 2021;8:8697020. [Google Scholar] [PubMed]
- 3. Thienpont E, Klasan A. The dissatisfied total knee arthroplasty patient. New technologies-the white knight in shining armor coming to their rescue? Arch Orthop Trauma Surg 2021;141:2021-5. [Google Scholar] [PubMed]
- 4. Winnock De Grave P, Luyckx T, Claeys K, Tampere T, Kellens J, Müller J, et al. Higher satisfaction after total knee arthroplasty using restricted inverse kinematic alignment compared to adjusted mechanical alignment. Knee Surg Sports Traumatol Arthrosc 2022;30:488-99. [Google Scholar] [PubMed]
- 5. Abdel MP, Ollivier M, Parratte S, Trousdale RT, Berry DJ, Pagnano MW. Effect of post-operative mechanical axis alignment on survival and functional outcomes of modern total knee arthroplasties with cement: A concise follow-up at 20 years. J Bone Joint Surg Am 2018;100:472-8. [Google Scholar] [PubMed]
- 6. Hess S, Moser LB, Amsler F, Behrend H, Hirschmann MT. Highly variable coronal tibial and femoral alignment in osteoarthritic knees: A systematic review. Knee Surg Sports Traumatol Arthrosc 2019;27:1368-77. [Google Scholar] [PubMed]
- 7. Hirschmann MT, Moser LB, Amsler F, Behrend H, Leclercq V, Hess S. Phenotyping the knee in young non-osteoarthritic knees shows a wide distribution of femoral and tibial coronal alignment. Knee Surg Sports Traumatol Arthrosc 2019;27:1385-93. [Google Scholar] [PubMed]
- 8. Graichen H, Lekkreusuwan K, Eller K, Grau T, Hirschmann MT, Scior W. A single type of varus knee does not exist: Morphotyping and gap analysis in varus OA. Knee Surg Sports Traumatol Arthrosc 2022;30:2600-8. [Google Scholar] [PubMed]
- 9. MacDessi SJ, Griffiths-Jones W, Harris IA, Bellemans J, Chen DB. Coronal plane alignment of the knee (CPAK) classification. Bone Joint J 2021;103-B:329-37. [Google Scholar] [PubMed]
- 10. Sappey-Marinier E, Batailler C, Swan J, Schmidt A, Cheze L, MacDessi SJ, et al. Mechanical alignment for primary TKA may change both knee phenotype and joint line obliquity without influencing clinical outcomes: A study comparing restored and unrestored joint line obliquity. Knee Surg Sports Traumatol Arthrosc 2021;30:2806-14. [Google Scholar] [PubMed]
- 11. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not? Clin Orthop Relat Res 2010;468:57-63. [Google Scholar] [PubMed]
- 12. Klem NR, Kent P, Smith A, Dowsey MM, Fary R, Choong P, et al. Satisfaction after total knee replacement for osteoarthritis is usually high, but what are we measuring? A systematic review. OARSI Open 2020;2:100036. [Google Scholar] [PubMed]
- 13. Singh M, Harary J, Schilling PL, Moschetti WE. Patient satisfaction is nearly 90% after total knee arthroplasty; we are better than we were. J Arthroplasty 2024;40:1521-5.e1. [Google Scholar] [PubMed]
- 14. Choi YJ, Ra HJ. Patient satisfaction after total knee arthroplasty. Knee Surg Relat Res 2016;28:1-15. [Google Scholar] [PubMed]
- 15. Yang HY, Yoon TW, Kim JY, Seon JK. Radiologic assessment of knee phenotypes based on the coronal plane alignment of the knee classification in a Korean population. Clin Orthop Surg 2024;16:422-9. [Google Scholar] [PubMed]
- 16. Samant V, Desai M. Coronal plane alignment of knee joint (C.P.A.K.) classification in Indian population-study of a new classification system in Indian knees. J Orthop Rep 2024;3:100277. [Google Scholar] [PubMed]
- 17. Donnelly E. In Vitro Investigations of Conventional vs. Robotic-Assisted Total Knee Arthroplasty; [Doctoral Dissertation, The University of Western Ontario]. [Google Scholar] [PubMed]
- 18. Arai N, Toyooka S, Masuda H, Kawano H, Nakagawa T. Kinematic alignment achieves a more balanced total knee arthroplasty than mechanical alignment among CPAK type I patients: A simulation study. J Clin Med 2024;13:3596. [Google Scholar] [PubMed]
- 19. Agarwal S, Ayeni FE, Sorial R. Impact of change in coronal plane alignment of Knee (CPAK) classification on outcomes of robotic-assisted TKA. Arthroplasty 2024;6:15. [Google Scholar] [PubMed]
- 20. Bollars P, Feyen H, Nathwani D, Albelooshi A, Ettinger M, De Corte R, et al. Postoperative changes in CPAK-classification do not significantly influence patient-reported outcome measures following conventional or robotic-assisted total knee arthroplasty: A randomised controlled trial. Knee Surg Sports Traumatol Arthrosc 2025;33:3333-40. [Google Scholar] [PubMed]
- 21. Liu B, Feng C, Tu C. Kinematic alignment versus mechanical alignment in primary total knee arthroplasty: An updated meta-analysis of randomized controlled trials. J Orthop Surg Res 2022;17:201. [Google Scholar] [PubMed]
- 22. Alhifzi Z. Systematic review and meta-analysis of long term outcomes and innovations in total knee arthroplasty: KINEMATIC, PERSONALIZED KNEE vs. CONVENTIONAL. Orthop Rev (Pavia) 2024;16:122318. [Google Scholar] [PubMed]
- 23. Waterson HB, Clement ND, Eyres KS, Mandalia VI, Toms AD. The early outcome of kinematic versus mechanical alignment in total knee arthroplasty: A prospective randomised control trial. Bone Joint J 2016;98:1360-8. [Google Scholar] [PubMed]
- 24. Ram Sudhan S, Balemane S, Mancheri MN, Gopinath NP. The CPAK paradigm in total knee arthroplasty: A critical review of its theoretical rationale and clinical applicability. J Orthop Rep 2025 12(3):100824. [Google Scholar] [PubMed]
- 25. Bouché PA, Kutaish H, Gasparutto X, Lubbeke A, Miozzari HH, Hannouche D. Coronal plane alignment of the knee classification in osteoarthritic knees: Poor to moderate reliability and implications for imaging choice. J Arthroplasty 2025;41:725-32. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes February 1, 2026 Assessment of Bone Resection Accuracy in Robotic-Arm-Assisted Total Knee Arthroplasty: A Prospective Observational Study
February 1, 2026 Assessment of Bone Resection Accuracy in Robotic-Arm-Assisted Total Knee Arthroplasty: A Prospective Observational Study October 1, 2025 How Old is Too Old? Outcomes of Primary Total Knee Arthroplasty in Patients 70 Years or Older
October 1, 2025 How Old is Too Old? Outcomes of Primary Total Knee Arthroplasty in Patients 70 Years or Older March 1, 2025 Does Multiple Intravenous Tranexamic Acid Doses in Patients Undergoing Total Knee Arthroplasty using Kinematic Alignment without Tourniquet Application show any Difference in Blood Loss, Transfusion Requirements and Hospital Stays: A Randomized Controlled Study
March 1, 2025 Does Multiple Intravenous Tranexamic Acid Doses in Patients Undergoing Total Knee Arthroplasty using Kinematic Alignment without Tourniquet Application show any Difference in Blood Loss, Transfusion Requirements and Hospital Stays: A Randomized Controlled Study