
Using this technique, an acute posterior hip dislocation can be reduced easily without the need for traction, assistants, and any special equipment.
Dr. Aakash Mugalur, 2961/9, CH 6B, 3rd Cross, 1st Main, Bhanavi Hospital, Saraswathipuram, Mysuru - 570 009, Karnataka, India. E-mail: orthoaakash@gmail.com
Abstract
Introduction: Hip dislocations are a result of significant force and trauma and constitute one of the many orthopedic emergencies which require immediate attention. Of the hip dislocations, posterior hip dislocation is more common. Over the years, significant changes have been made with respect to the techniques of reducing hip dislocation. Depending on the technique used and the build of the surgeon and the patient, there is variation with respect to the number of assistants required, the position of the patient, the force required to achieve the traction, and the requirement of additional adjuvants such as a traction table. However, traction still remains the main principle in the reduction of the dislocated hip joint.
Case Report: Two patients presented with post-traumatic posterior dislocation of the hip joint. We used a novel technique which completely eliminates the requirement for traction in the reduction of the hip joint. It can be shortly described as a maneuver encompassing the following: “Hyperflexion-Adduction-Internal rotation-Abduction-External rotation-Extension.”
Conclusion: Despite the improvement in the techniques of reduction for posterior dislocation of the hip, traction remains the mainstay. Our described technique does not require traction. It significantly reduces the strain on the surgeon's back and is ergonomic. It can be done in the supine position, and no assistants are required, saving time and manpower. It is simple, easily replicable, and independent of the build of the surgeon and the patient. Our “no traction” novel technique is a simple, easily replicable and learnable, ergonomic, surgeon-friendly technique which will ease the effort of reducing a posteriorly dislocated hip.
Keywords: Dislocation, hip, reduction, traction, technique
Hip dislocations are a result of significant force and trauma and constitute one of the many orthopaedic emergencies which require immediate attention. Of the hip dislocations, posterior hip dislocation is more common [1]. Timely reduction of the dislocated hip joint is not only important in alleviating the patient’s pain and discomfort but also quintessential in decreasing the chances of avascular necrosis of the femoral head and other complications associated with hip dislocation [2,3].
The technique of closed reduction of the hip joint was first described by Bigelow in 1870 [4]. Over the years that followed, many new and innovative techniques have been described [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,18,19,20]. Most of the techniques require an additional assistant for the reduction of the hip joint. Many techniques aim to decrease the load on the surgeon’s back by use traction table [19] for assisting reduction, by use of hydraulic lifts [20], and by ergonomically modifying the technique [5]. However, most of the techniques still use traction, and the force by the surgeon varies between patients depending on the build of the patient.
We describe a new technique which is easy to perform irrespective of the build of the patient or the surgeon, doesn’t require an assistant and is replicable.
The patient is taken to the operating theatre after signing the informed consent form. The patient is anaesthetised by the anaesthesiologist with spinal anaesthesia for complete relaxation of the bilateral lower limbs. The patient is positioned supine on the operating table or the operating room stretcher. The surgeon stands on the contralateral side of the dislocated hip. The surgeon holds the foot and ankle region of the dislocated lower extremity with his right hand. He holds the knee region of the dislocated extremity with his left hand. The above-described use of hands for holding the extremity is for reducing the left hip dislocation. They need to be interchanged to reduce the right hip of the patient. The dislocated hip is gradually manoeuvred into hyperflexion at the hip with maximum permissible adduction and internal rotation at the hip joint. The knee joint is completely flexed. Maintaining the hyperflexion at the hip joint, the hip joint is gradually dialed into abduction. The hip is then gradually extended and externally rotated with gradual knee extension, leading to the reduction of the dislocated hip (Figs. 1 and 2).

Figure 1: Reduction maneuver. (a) Surgeon holding the left ankle region with right hand and the left knee with the left hand as seen from the foot end of the table, (b) Surgeon holding the left ankle region with right hand and the left knee with the left hand as seen from the side, (c) Hyperflexion, adduction and internal rotation at the hip joint as seen from the foot end of the table, (d) Hyperflexion, adduction, and internal rotation at the hip joint as seen from the side.

Figure 2: Reduction maneuver continuation. (a) Dialing the hip into abduction while maintaining the hyperflexion at the hip joint as seen from the side, (b) Dialing the hip into abduction while maintaining the hyperflexion at the hip joint as seen from the foot end of the table, (c) Gradual external rotation and extension of the hip joint while maintaining the abduction with simultaneous extension of the knee joint as seen from the foot end of the table, (d) Gradual external rotation and extension of the hip joint while maintaining the abduction with simultaneous extension of the knee joint as seen from the side, (e) Completion of the reduction maneuver with gradual extension of the hip and the knee joints as seen from the foot end of the table, (f) Completion of the reduction maneuver with gradual extension of the hip and the knee joints as seen from the side.
Case 1:
A 31-year-old male patient presented to the casualty with a history of car accident. The patient was unrestrained at the time of accident. The patient had complaints of left hip pain and inability to straighten the left hip. The left lower limb was in flexion, adduction, and internal rotation deformity consistent with left hip posterior dislocation. Radiographs confirmed the posterior hip dislocation. The patient did not have any other associated injuries. Written informed consent was taken from the patient for the procedure. The patient underwent closed reduction of the left hip with the above-described novel technique under spinal anaesthesia. The congruency of reduction was confirmed in the operating theatre under an image intensifier. Post-procedure radiographs showed congruent reduction with no iatrogenic fractures. There was no neurovascular deficit post-reduction. The patient was discharged the next day. Fig. 3 shows the initial radiograph with left hip dislocation and the post-reduction radiograph.
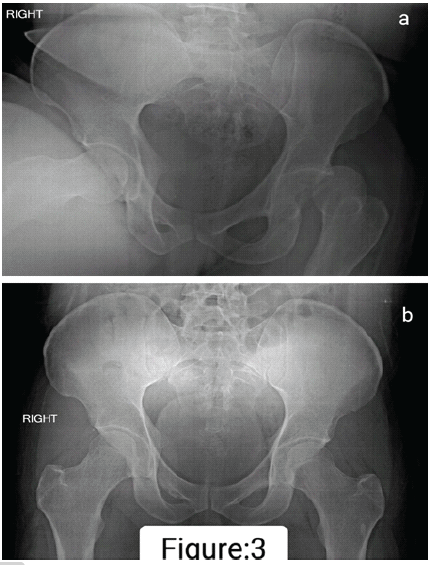
Figure 3: (a) Anteroposterior radiograph of the pelvis with both hips showing posterior dislocation of the left hip, (b) Anteroposterior radiograph of the pelvis with both hips showing congruent reduction of the left hip joint.
Case 2:
A 35-year-old male patient met with a road traffic accident. The patient was traveling by bike and was hit by a car. The patient was diagnosed with left hip dislocation. The patient was initially treated at another hospital for the same. However, despite the multiple attempts at reduction, the hip was still unreduced and was referred for further management. The patient was haemodynamically stable at the time of presentation and did not have any associated injuries. Written informed consent was taken from the patient for the procedure. The patient underwent closed reduction of the left hip utilizing the above-described novel technique of hip reduction under spinal anaesthesia. Fig. 4 shows the initial radiograph with left hip dislocation and the post-reduction radiograph. The patient did not have any neurovascular deficits and was discharged the next day.
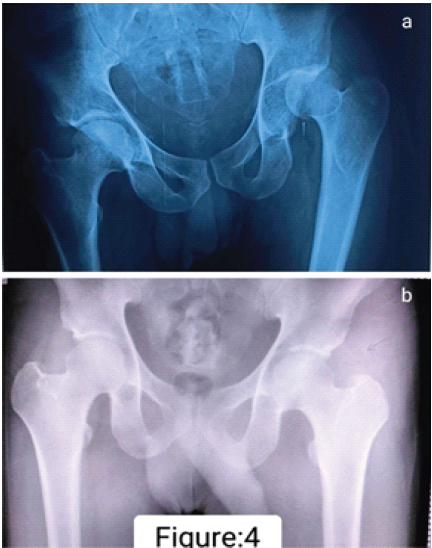
Figure 4: (a) Anteroposterior radiograph of the pelvis with both hips showing posterior dislocation of the left hip, (b) Anteroposterior radiograph of the pelvis with both hips showing congruent reduction of the left hip joint.
Multiple techniques exist for reducing the posterior dislocation of the hip joint. Allis and Bigelow’s technique was one of the earlier described techniques. Over the period of years, many modifications and newer techniques have been described to aid the surgeon in easy reduction of the hip joint.
The Allis and Bigelow techniques were the workhorse [4,6]. But it puts a lot of strain on the surgeon’s back and can be quite difficult in a hefty patient. Average-built surgeons may face more difficulty in employing these techniques. Lefkowitz [7], Captain Morgan [8], Tulsa, Rochester, Whislter [4,5,13,14], East-Baltimore lift [9], Piggy Back [12] techniques are modifications with an aim to reduce the strain on the surgeons’ back. Skoff [15] and traction-countertraction [17] maneuvers place the patient in the lateral decubitus position. Stimson’s gravity-assisted reduction [16] utilizes the prone position. Howard and lateral traction methods utilize an additional lateral traction to aid in the reduction [5,10]. The flexion-adduction method [18] advocates traction in the flexed adducted position of the lower limb, and an assistant guides the femoral head, aiding the reduction. The foot fulcrum method [5] decreases the strain on the surgeon’s back and decreases the force of reduction and the impact on the femoral head. The Wadell technique [5] has been recommended as it conforms to the Occupational Safety and Health Administration principles, decreasing the force and strain on the surgeon’s back. The Shigemura et al. technique utilizes the traction table to reduce the dislocation [19]. Zwank and Kumasaka describe the utilization of hydraulic lifts to aid in the reduction [20]. Utilizing the traction table and hydraulic lifts definitely reduces the force exerted by the surgeon. But increase the time and the armamentarium required for reducing the hip. They may be reserved for difficult reductions, but routine use of the techniques is not very practical. Although multiple changes have been made to the original technique over the period of years, the principle of reduction across the techniques remains “traction”. The force required to generate the traction has been reduced using the fulcrum principle, using assistants, using gravity-assisted reduction, changing the position of the patient and the surgeon, modifying the techniques to decrease the strain on the surgeon’s back, utilizing a traction table, and using hydraulic lifts. However, “traction” is still required across all the techniques and is the mainstay of reducing the hip. Despite the improvisation in techniques, it still might be difficult to generate enough traction in a heavily built patient, especially for an average-sized surgeon. Our novel technique is different in that no traction is required. It is a gentle, easily replicable, and learnable manoeuvre. It can be achieved by a surgeon of any build or sex. The build of the patient does not interfere with the manoeuvre, as force is not required. It does not put the surgeon’s back at risk. It is advantageous since there is no requirement for an assistant. The hip is reduced in the supine position, and hence, there is no requirement for specific positioning. It does not require any special equipment or armamentarium. We in our institute use spinal anaesthesia or a sub-arachnoid block as a protocol for hip dislocations, as it provides us with complete muscle relaxation and it has the advantage of post-operative pain relief. However, this procedure can also be used with sedation or short general anaesthesia.
Our technique is simple and efficient with respect to the following factors: (a) Energy or force exerted by the surgeon is very minimal; (b) the surgeon’s back is not at risk; (c) the workforce since no assistant is required; (d) time, since there is no specific positioning or armamentarium requirement and can as well be done on the patient trolley; and (e) easy irrespective of the build of the patient or the surgeon.
We have used this technique successfully in two patients with acute posterior dislocation of the hip joint. One patient was well built, and the other patient was of medium build. We have not evaluated this technique in delayed presentations of the dislocation, fracture dislocations of the hip, and prosthetic dislocations of the hip joint. However, perusal of this technique in multiple patients in the future will help us to evaluate the difficulties associated with this technique, if any. At present, this is a simple technique for reducing the posterior hip dislocations, and the same principle can also be applied for reducing the anterior hip dislocations too.
Our “no traction” novel technique is a simple, easily replicable and learnable, ergonomic, surgeon-friendly technique which will ease the effort of reducing a posteriorly dislocated hip.
Techniques for the reduction of a posteriorly dislocated hip joint have evolved over the period of time. However, in all the techniques hitherto described, “traction” is the keystone. Our technique described above eliminates the need for traction and assistants. It is a simple, ergonomic, surgeon-friendly technique which is easily learnable and reproducible. We have tried this technique successfully in two patients with acute isolated posterior hip dislocation. We have not used it in fracture dislocations, neglected dislocations, and prosthetic dislocations. Perusal of this technique in the future will shed more light on the difficulties and possible limitations associated with this technique.
References
- 1. Clegg TE, Roberts CS, Greene JW, Prather BA. Hip dislocations-epidemiology, treatment, and outcomes. Injury 2010;41:329-34. [Google Scholar] [PubMed]
- 2. Dwyer AJ, John B, Singh SA, Mam MK. Complications after posterior dislocation of the hip. Int Orthop 2006;30:224-7. [Google Scholar] [PubMed]
- 3. Dreinhöfer KE, Schwarzkopf SR, Haas NP, Tscherne H. Isolated traumatic dislocation of the hip. Long-term results in 50 patients. J Bone Joint Surg Br 1994;76:6-12. [Google Scholar] [PubMed]
- 4. Dawson-Amoah K, Raszewski J, Duplantier N, Waddell BS. Dislocation of the hip: A review of types, causes, and treatment. Ochsner J 2018;18:242-52. [Google Scholar] [PubMed]
- 5. Waddell BS, Mohamed S, Glomset JT, Meyer MS. A detailed review of hip reduction maneuvers: A focus on physician safety and introduction of the waddell technique. Orthop Rev (Pavia) 2016;8:6253. [Google Scholar] [PubMed]
- 6. Allis OH. The Hip. Philadelphia, PA: Dorman Printer; 1895. p. 14-26. [Google Scholar] [PubMed]
- 7. Lefkowitz M. A new method for reduction of hip dislocations. Orthop Rev 1993;22:253-6. [Google Scholar] [PubMed]
- 8. Hendey GW, Avila A. The captain morgan technique for the reduction of the dislocated hip. Ann Emerg Med 2011;58:536-40. [Google Scholar] [PubMed]
- 9. Schafer SJ, Anglen JO. The east baltimore lift: A simple and effective method for reduction of posterior hip dislocations. J Orthop Trauma 1999;13:56-7. [Google Scholar] [PubMed]
- 10. Howard CB. A gentle method of reducing traumatic dislocation of the hip. Injury1992;23:481-2. [Google Scholar] [PubMed]
- 11. Nordt WE, 3rd. Maneuvers for reducing dislocated hips. A new technique and a literature review. Clin Orthop Relat Res 1999;360:260-4. [Google Scholar] [PubMed]
- 12. Marya SK, Samuel AW. Piggy back technique for relocation of posterior dislocation of the hip. Injury1994;25:483-4. [Google Scholar] [PubMed]
- 13. Vosburgh CL, Vosburgh JB. Closed reduction for total hip arthroplasty dislocation. The Tulsa technique. J Arthroplasty 1995;10:693-4. [Google Scholar] [PubMed]
- 14. Stefanich RJ. Closed reduction of posterior hip dislocation: The Rochester method. Am J Orthop (Belle Mead NJ) 1999;28:64-5. [Google Scholar] [PubMed]
- 15. Skoff HD. Posterior hip dislocation, a new technique for reduction. Orthop Rev 1986;15:405-9. [Google Scholar] [PubMed]
- 16. Stimson LA. A Practical Treatise on Fractures and Dislocations. New York, Philadelphia, PA: Lea Brothers and Company; 1905. Available from: https://archive.org/details/practicaltreat00stim [Last accessed on 2018 Jul 17]. [Google Scholar] [PubMed]
- 17. Dahners LE, Hundley JD. Reduction of posterior hip dislocations in the lateral position using traction-countertraction: safer for the surgeon? J Orthop Trauma 1999;13:373-4. [Google Scholar] [PubMed]
- 18. Bassi JL, Ahuja SC, Singh H. A flexion adduction method for the reduction of posterior dislocation of the hip. J Bone Joint Surg Br 1992;74:157-8. [Google Scholar] [PubMed]
- 19. Shigemura T, Miura M, Murata Y, Yamamoto Y, Maruyama J, Wada Y. A new closed reduction technique using a traction table to treat a traumatic posterior dislocation of the hip joint. Orthop Traumatol Surg Res 2020;106:881-4. [Google Scholar] [PubMed]
- 20. Zwank MD, Kumasaka PG. A new technique for reduction of a posteriorly dislocated hip joint. Am J Emerg Med 2024;84:191.e1-3. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Novel Lag Screw Application In The Reduction Of Neer Type V Distal Clavicle Fracture: A Case Report And Technical Note
December 1, 2025 Novel Lag Screw Application In The Reduction Of Neer Type V Distal Clavicle Fracture: A Case Report And Technical Note October 1, 2025 Bilateral Simultaneous Anterior Obturator and Pubic Dislocation of the Hip: A Case Report and Literature Review
October 1, 2025 Bilateral Simultaneous Anterior Obturator and Pubic Dislocation of the Hip: A Case Report and Literature Review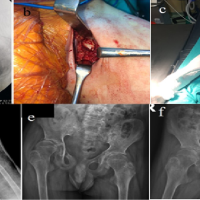 March 10, 2024 Treatment of Posterior Hip Dislocation due to Juvenile Idiopathic Arthritis. Report of Two Cases
March 10, 2024 Treatment of Posterior Hip Dislocation due to Juvenile Idiopathic Arthritis. Report of Two Cases February 10, 2024 Use of Mini TightRope® for Delayed Presentation of a Fifth Carpometacarpal Joint Dislocation
February 10, 2024 Use of Mini TightRope® for Delayed Presentation of a Fifth Carpometacarpal Joint Dislocation