
Percutaneous hydrotenotomy can be incorporated into an effective operative treatment plan for periligamentous calcification of the MCL in the setting of traumatic knee injury.
Dr. Brigitte Lieu, Department of Orthopedic Surgery, Virginia Commonwealth University Health System, Richmond, Virginia. E-mail: lieuba@vcu.edu
Abstract
Introduction: Periligamentous calcification of the medial collateral ligament (MCL) is a rare condition that is mechanistically similar to calcific tendinitis, resulting from the deposition of calcium hydroxyapatite crystals in periarticular muscular attachments. Whereas most documented cases of periligamentous MCL calcification resolve with conservative therapy, little guidance exists in the orthopedic literature regarding viable operative treatment options for patients with symptoms refractory to conservative management. To our knowledge, this is one of only two case reports reporting the findings of percutaneous hydrotenotomy applied to MCL calcification and the first applied specifically to post-traumatic MCL calcification.
Case Report: The patient in our report presented with trauma-associated periligamentous calcification of the MCL that failed conservative management. The patient underwent percutaneous hydrotenotomy under ultrasound and fluoroscopic guidance, requiring open conversion for complete access and debridement of the deeper calcific deposits. At 1-year follow-up, the knee was non-tender with a full range of motion, and follow-up radiographs confirmed complete resolution of the calcification.
Conclusion: The successful treatment of this patient demonstrates that percutaneous hydrotenotomy can be incorporated into an effective treatment plan for periligamentous calcification of the MCL secondary to traumatic knee injury.
Keywords: Medial collateral ligament, calcific tendinitis, percutaneous hydrotenotomy.
Calcific tendinitis is a well-documented condition resulting from the deposition of calcium hydroxyapatite crystals in periarticular muscular attachments, commonly occurring at sites such as the shoulder [1]. Periligamentous medial collateral ligament (MCL) calcification shares a similar mechanism with calcific tendinitis, but it is more rarely reported in the literature. Given the rarity of calcific deposition at the attachment of the MCL origin in particular, it remains unclear what the best recommendations are for treatment [1]. The majority of cases resolve with thorough conservative treatment consisting of physical therapy, non-steroidal anti-inflammatory drugs, and local corticosteroid injections; however, less literature has been published regarding treatment options for refractory cases [1].
Several operative alternatives have been reported in prior literature, including a handful of studies describing arthroscopic and open excisions [2,3,4]. To our knowledge, only one previous paper reports successful treatment of this condition with the use of a percutaneous hydrotenotomy under ultrasound guidance [5,6]. Whereas this prior research treated a patient with an atraumatic history of calcific knee pain, this case report is the first to apply this treatment approach in the more common setting of traumatic knee injury [5]. As such, future cases of periligamentous calcification of the MCL causing knee pain refractory to conservative treatment might be considered for surgical treatment with fluoroscopic and ultrasound-guided percutaneous hydrotenotomy. The patient was informed that data concerning the case would be submitted for publication; she provided consent.
A 51-year-old female patient with a medical history of type 2 diabetes mellitus presented to the clinic with right knee pain persisting for over 6 years. Her symptoms began following a fall onto the anterior right knee and progressively worsened over time. The patient previously received a series of conservative treatments at an outside orthopedic clinic, including rest, activity modification, home exercises, physical therapy, intra-articular cortisone injections, and non-steroidal anti-inflammatory drugs, without any lasting pain relief. Surgical intervention was not offered by previous providers due to concerns about damaging the integrity of the ligaments with the removal of the calcifications. Initial physical examination revealed no skin lesions, no effusion, and a full range of motion of the right knee. The patient had significant tenderness to palpation around the MCL origin. The knee was stable to valgus and varus stress examinations. There were no neurologic deficits present on examination, and pulses were intact.
Imaging, including X-rays and magnetic resonance imaging of the right knee, confirmed the presence of calcium hydroxyapatite crystal deposition along the femoral attachment of the MCL (Fig. 1 and 2).
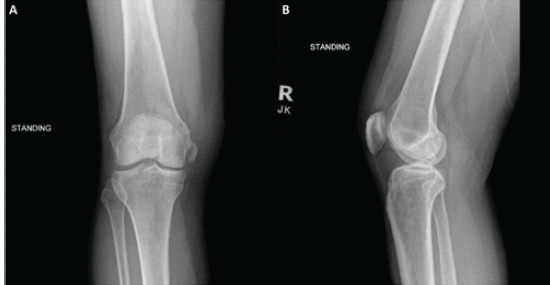
Figure 1: Pre-operative radiographs. Pre-operative anteroposterior and lateral X-rays of the right
knee demonstrating calcification medial to the medial femoral condyle.
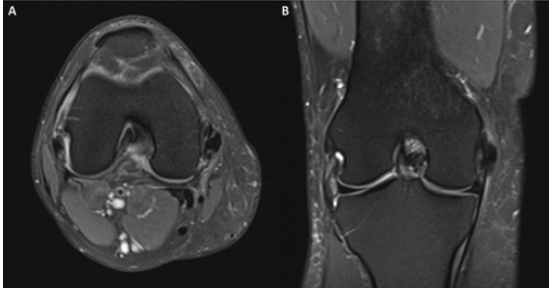
Figure 2: Pre-operative magnetic resonance imaging. T2-weighted axial and coronal views of the right knee demonstrate calcification within the medial collateral ligament near the femoral attachment.
There were no findings of ligamentous or meniscal pathology.
Given continued symptoms despite failed conservative management, she was recommended and consented to undergo percutaneous hydrotenotomy debridement under fluoroscopic and/or ultrasound guidance of the right knee to remove the calcific deposition on the MCL [6].
Surgical procedure:
The patient underwent the planned procedure under general anesthesia at an ambulatory surgical center. With the patient supine, the calcification was localized using fluoroscopy and ultrasound. After a 20 mL local lidocaine injection, a small stab incision was made proximally, and the Tenjet device (HydroCision, Inc., North Billerica, MA) was used to evacuate calcification within the proximal MCL. A similar stab incision was made distally, and the removal process was repeated. Significant calcification was disrupted, but there remained some calcification noted on intraoperative fluoroscopy (Fig. 3).
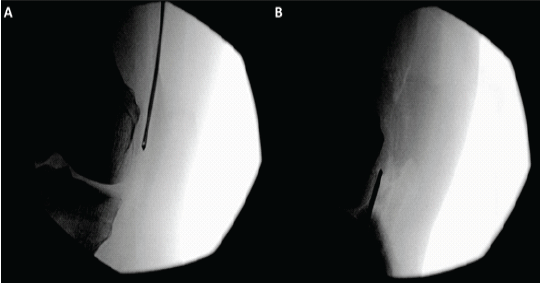
Figure 3: Intraoperative fluoroscopy pre-debridement. Intraoperative fluoroscopy demonstrating localization of the periligamentous medial collateral ligament calcification before completion of debridement.
The surgeon then elected to make a small mini-open incision and dissect down through the sartorial fascia to the proximal MCL, which allowed for further localization of calcification at this location. At that point, the Tenjet device was again used to disrupt the significant calcium found at this location with success (Fig. 4).
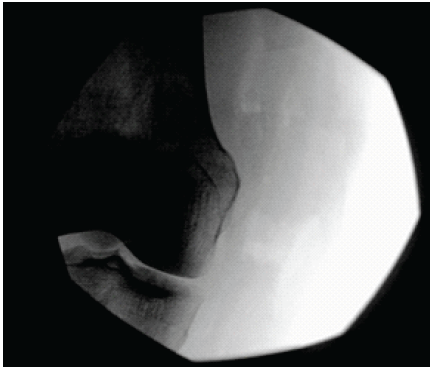
Figure 4: Intraoperative fluoroscopy post-debridement. Intraoperative fluoroscopy demonstrating complete resolution of the periligamentous medial collateral ligament calcification following percutaneous hydrotenotomy.
The integrity of the MCL was confirmed by performing a valgus stress test intraoperatively. The surgical site was then irrigated, the incision was closed in layered fashion with 0 Vicryl, 2-0 Monocryl, and 3-0 Monocryl sutures, and sterile dressings were placed. Post-procedure radiographs demonstrated interval removal of the calcification. In the immediate post-operative period, the patient was allowed to weight bear as tolerated with crutches and instructed to avoid strenuous activity.
Post-operative course:
The post-operative protocol for this patient was range of motion as tolerated and weight bearing as tolerated with the assistance of crutches. Physical therapy was initiated on post-operative day 1. At her 2-week post-operative visit, she reported medial knee pain and localized numbness over the anteromedial leg, consistent with likely iatrogenic saphenous nerve injury. Her incision was well healed, and there were no signs of infection. She was advised to continue weight-bearing with crutches for an additional 2 weeks and then gradually wean off, while continuing physical therapy and range of motion exercises with close monitoring of saphenous nerve-type symptoms.
Around 6 weeks postoperatively, she experienced an increase in diffuse knee pain and reported persistent numbness along the anterior tibia. A physical examination revealed tenderness beyond the medial knee and along the anterior tibial region. A Medrol dosepak was prescribed for the acute onset of pain.
At her 10-week follow-up visit, the patient noted significant improvement. Her pain had resolved to a 0/10 at rest, and her numbness had also decreased. However, she still experienced some altered levels of sensation over the anterior tibial and lateral patella regions. She also reported occasional nighttime discomfort and continued physical therapy with good tolerance, experiencing pain only with heavier resistance exercises.
At her 5-month follow-up visit, the patient reported complete resolution of her right medial knee pain and full return to daily activities, including long-distance walking. Physical examination demonstrated a full range of motion, no tenderness, and only minimal residual numbness. At 1-year follow-up, her physical examination remained benign with a full range of motion and no tenderness medially. She had normal sensation along her lower leg at this time without any neurologic complaints. Repeat right knee radiographs confirmed no calcification remaining at the femoral MCL origin.
Percutaneous hydrotenotomy is achieved using a high-pressure, dual-lumen fluid jet device to remove periligamentous calcification of the MCL. Although this technique has been used to treat calcific tendinitis in a variety of joints, its application in the treatment of MCL pathology is not yet well-documented, with only one prior report by Dakkak describing successful ultrasound-guided percutaneous hydrotenotomy of atraumatic periligamentous calcification of the MCL [6]. Although MCL calcifications are a novel indication for percutaneous hydrotenotomy, this procedure has been applied to several other indications in prior literature, especially in the setting of upper extremity pathologies. Lateral epicondylitis has been successfully treated with minimally invasive percutaneous hydrotenotomy, as reported by Dakkak et al. in a case series of 100 patients, demonstrating statistically significant improvements in 1-year functional outcomes (i.e., Oxford Elbow Score) and zero complications among their sample [7]. Yet another study investigated percutaneous hydrotenotomy as applied to medial and lateral epicondylitis, reporting significant improvements from baseline in both pain and function metrics 2 weeks after percutaneous hydrotenotomy, exhibiting continued improvement through the 12-month mark [8]. Percutaneous ultrasonic tenotomy, as a broader technique, has demonstrated efficacy in other studies in providing symptomatic relief from Achilles tendinopathy and plantar fasciitis. However, research has yet to be conducted utilizing percutaneous hydrotenotomy to treat these specific conditions [9]. Traditionally, treatment for MCL calcifications favours conservative measures, including non-steroidal anti-inflammatory drugs, among other analgesics [1,10]. Prior research has also reported successful management of symptomatic MCL calcification with a shockwave therapy-dry needling-local corticosteroid injection regimen [10]. If conservative measures are trialed and fail, arthroscopic or open resection is then considered a last line to remove the calcific mass [1]. Within this current treatment paradigm, there remains a role for additional minimally invasive procedures to address MCL calcifications, such as percutaneous hydrotenotomy. The patient in our report presented with trauma-associated periligamentous calcification of the MCL, then underwent percutaneous hydrotenotomy under both ultrasound and fluoroscopic guidance with complete evacuation of calcification. At her 1-year follow-up, the patient demonstrated complete resolution of medial knee pain, full return to daily activities, and full range of motion on physical examination. Follow-up radiographs confirmed complete resolution of the calcifications at the femoral MCL origin (Fig. 5). These findings highlight the overall success of the procedure in both symptom relief and radiographic improvement. Another consideration in the case was the post-operative development of saphenous neuritis, most likely due to the proximity of the incision and debridement zone to the infrapatellar branch of the saphenous nerve. This transient complication may have been avoided with an alternative incision placement or if open conversion had not been required. This is a possible complication that should be discussed with patients at length before this procedure. Conversion to open is always an option and must be discussed with patients preoperatively, as well as if there is an inability to completely remove the calcification through the percutaneous.
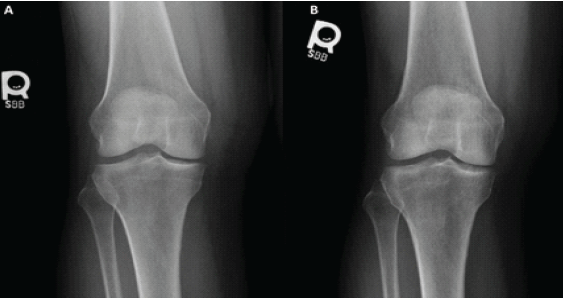
Figure 5: Post-operative radiographs. Post-operative anteroposterior X-rays of the right knee obtained at (A) 2 weeks post-operative and (B) approximately 1 year post-operative, demonstrating
complete resolution and no subsequent recurrence of calcification within the medial collateral ligament. technique.
In select patients with persistent, localized medial knee pain and radiographic evidence of calcification at a rare site such as the MCL, percutaneous hydrotenotomy with optional open access harbours potential as an effective and safe treatment option.
This case illustrates the feasibility of using percutaneous hydrotenotomy for periligamentous calcification of the medial collateral ligament, as well as the importance of maintaining a flexible operative strategy in treating rare orthopaedic presentations.
References
- 1. You Y, Li Z, Guo J, Zhang T. Case report: Surgical management of medial collateral ligament calcification. Front Surg 2024;11:1506867. [Google Scholar] [PubMed]
- 2. Song K, Dong J, Zhang Y, Chen B, Wang F, Zhao J, et al. Arthroscopic management of calcific tendonitis of the medial collateral ligament. Knee 2013;20:63-5. [Google Scholar] [PubMed]
- 3. Kamawal Y, Steinert AF, Holzapfel BM, Rudert M, Barthel T. Case report – calcification of the medial collateral ligament of the knee with simultaneous calcifying tendinitis of the rotator cuff. BMC Musculoskelet Disord 2016;17:283. [Google Scholar] [PubMed]
- 4. White WJ, Sarraf KM, Schranz P. Acute calcific deposition in the lateral collateral ligament of the knee. J Knee Surg 2013;26 Suppl 1:S116-9. [Google Scholar] [PubMed]
- 5. Majewski M, Susanne H, Klaus S. Epidemiology of athletic knee injuries: A 10-year study. Knee 2006;13:184-8. [Google Scholar] [PubMed]
- 6. Dakkak M. Ultrasound-guided treatment of medial collateral ligament calcification of the knee with TenjetTM: A case report. Pain Manag 2024;14:29-33. [Google Scholar] [PubMed]
- 7. Dakkak M, Patel V, King D, Genin J. Ultrasound-guided tenotomy for lateral epicondylitis with TenJet improves physical functional and decreased pain outcomes at 1 year: A case series review. JSES Int 2023;7:872-6. [Google Scholar] [PubMed]
- 8. Strauser-Curtis K, Varacallo CP, Voss TT, Stephens CB, Kapteyn RW. Ultrasound-guided tenotomy via a hydrosurgery resection device improves symptoms of chronic elbow tendinopathy: A multi-center prospective study. J Orthop Exp Innov 2022;3:1. [Google Scholar] [PubMed]
- 9. Vajapey S, Ghenbot S, Baria MR, Magnussen RA, Vasileff WK. Utility of percutaneous ultrasonic tenotomy for tendinopathies: A systematic review. Sports Health 2021;13:258-64. [Google Scholar] [PubMed]
- 10. Siddiq MA, Jahan I. Medial collateral ligament calcification: A rare knee pain entity with literature review. Acta Radiol Open 2017;6:2058460117738549. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2023 Atraumatic Calcific Tendinitis in Medial Collateral Ligament: A Case Report
November 10, 2023 Atraumatic Calcific Tendinitis in Medial Collateral Ligament: A Case Report March 1, 2026 A Rare Case of Calcific Tendinitis of the Elbow Mimicking Lateral Epicondylitis: Diagnostic Challenges and Surgical Management
March 1, 2026 A Rare Case of Calcific Tendinitis of the Elbow Mimicking Lateral Epicondylitis: Diagnostic Challenges and Surgical Management February 1, 2026 A Novel Technique of Rerouting Semitendinosus Graft for Medial Collateral Ligament and Medial Patellofemoral Ligament Reconstruction – In a Polytrauma Patient with Multiligament Injury: Kakran et al. Technique
February 1, 2026 A Novel Technique of Rerouting Semitendinosus Graft for Medial Collateral Ligament and Medial Patellofemoral Ligament Reconstruction – In a Polytrauma Patient with Multiligament Injury: Kakran et al. Technique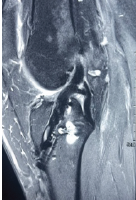 September 1, 2025 Simultaneous ACL Reconstruction and MCL Reconstruction in Patients with High BMI using Modified Lind Technique
September 1, 2025 Simultaneous ACL Reconstruction and MCL Reconstruction in Patients with High BMI using Modified Lind Technique