
Pelvic osteomyelitis should be strongly suspected in a child with an apparent septic hip when intraoperative findings are normal, especially in the presence of aggressive MRSA infection or atypical imaging, and prompt MRI can prevent diagnostic delay and guide appropriate management.
Dr. Anirudh Dwajan, Department of Orthopaedics, All India Institute of Medical Sciences, Bilaspur, Himachal Pradesh, India. E-mail: anirudhdwajan@gmail.com
Abstract
Introduction: Pelvic osteomyelitis is an uncommon but clinically important condition in children, often presenting with symptoms that closely mimic septic arthritis of the hip. Overlapping features, such as fever, severe hip pain, limp, and inability to bear weight, frequently lead to diagnostic delays and, in some cases, to unnecessary hip exploration. Early recognition is essential, particularly with increasingly aggressive presentations associated with methicillin-resistant Staphylococcus aureus (MRSA).
Case Report: An 11-year-old girl presented with fever, acute left hip pain, and refusal to bear weight, raising a strong suspicion of septic arthritis. Hip ultrasonography showed a peri-hip collection, and urgent hip arthrotomy was performed; however, the joint was found to be normal. Further exploration revealed a cortical breach in the iliac bone with pus tracking into the surrounding musculature. Post-operative magnetic resonance imaging (MRI) demonstrated osteomyelitis of the ilium and ischium with multiple intermuscular abscesses. Culture confirmed MRSA. Management was complicated by contrast-induced acute kidney injury and vancomycin-associated rash, necessitating modification of antimicrobial therapy. Surgical drainage and targeted antibiotics resulted in complete functional recovery at 12 months.
Conclusion: Pelvic osteomyelitis can convincingly mimic septic arthritis and may only be recognized when intraoperative findings are discordant with clinical expectations. MRI is indispensable for identifying pelvic sources of infection, particularly after a negative hip arthrotomy. Awareness of atypical features such as cortical breach, aggressive MRSA infection, and potential treatment-related complications is critical for timely diagnosis and optimal outcomes.
Keywords: Pelvic osteomyelitis, septic arthritis of the hip, methicillin-resistant Staphylococcus aureus, ilium, pediatric osteomyelitis.
Pelvic osteomyelitis is an uncommon but clinically significant cause of musculoskeletal infection in children. Its presentation is often subtle and easily misinterpreted because the deep location of the pelvic bones obscures early clinical signs. Children may present with hip or groin pain, fever, limp, abdominal discomfort, or refusal to bear weight – symptoms that closely resemble a range of more common conditions, particularly septic arthritis of the hip. This broad overlap frequently leads to diagnostic uncertainty and delays in instituting appropriate treatment [1,2]. Although pelvic involvement accounts for only a minority of acute hematogenous osteomyelitis cases in children, it is consistently associated with delayed recognition, with several studies reporting an average diagnostic delay of 10–12 days [1,3]. Such delays are clinically important, as progression of infection may result in muscular extension, abscess formation, sacroiliac joint involvement, or systemic complications. Moreover, multiple reports have documented cases in which pelvic osteomyelitis presents almost indistinguishably from septic arthritis, prompting non-therapeutic hip aspirations or arthrotomies before the extra-articular origin of infection is recognized [3]. Traditional imaging modalities contribute further to the diagnostic challenge. Plain radiographs are usually normal in early disease, and ultrasonography may reveal only non-specific soft-tissue changes or reactive hip effusion. Early magnetic resonance imaging (MRI) has therefore been recommended when clinical symptoms persist or when initial findings do not adequately explain the severity of the presentation, as MRI can delineate marrow edema, cortical involvement, and intermuscular abscesses that are otherwise occult [4,5]. In addition, the evolving microbiological pattern of pediatric osteomyelitis – including the increasing prevalence of methicillin-resistant Staphylococcus aureus (MRSA) – has led to more aggressive clinical courses and a greater need for precise diagnosis [6]. In this context, cases of pelvic osteomyelitis masquerading as septic arthritis highlight the limitations of relying solely on classical diagnostic algorithms. When intraoperative findings do not align with pre-operative expectations, re-evaluation of the differential diagnosis becomes essential. We describe the case of an 11-year-old girl who presented with all the hallmarks of septic arthritis of the hip but was ultimately found to have MRSA osteomyelitis of the ilium and ischium with soft-tissue extension. This case illustrates the diagnostic pitfalls associated with pelvic infections in children and reinforces the value of MRI and clinical vigilance when managing atypical or discordant presentations.
An 11-year-old girl, previously developmentally normal and immunized, presented with a 15-day history of progressive pain in the left hip. What began as intermittent discomfort gradually became constant, severe, and radiated down the thigh, eventually preventing her from bearing weight. She had experienced intermittent fever for 5 days and developed noticeable swelling over the left hip region 2 days before admission. Apart from a minor fall while running a month earlier, there was no significant antecedent event, and she had no history of chronic illness or tuberculosis contact. On arrival, she was afebrile and hemodynamically stable. Local examination showed a tender, fluctuant swelling measuring approximately 5–7 cm extending from the left inguinal region to the proximal thigh. The limb was held in a flexed and adducted position, and hip movements were severely restricted due to pain. No significant overlying warmth or erythema was noted. The remainder of the systemic examination was unremarkable.
Investigations:
Initial laboratory workup revealed elevated inflammatory markers, including a leukocyte count of 13,840/mm³ with neutrophilia, erythrocyte sedimentation rate of 97 mm/h, and C-reactive protein (CRP) of 371 mg/L. Renal and liver function tests were normal at baseline. Despite markedly elevated inflammatory markers, the patient remained hemodynamically stable without features of systemic sepsis. A pre-operative anteroposterior radiograph of the pelvis demonstrated preserved hip joint spaces with no cortical irregularity, lytic areas, periosteal reaction, or acetabular changes. The absence of early radiographic abnormalities is consistent with the known limitations of plain radiographs in detecting early pelvic osteomyelitis (Fig. 1).
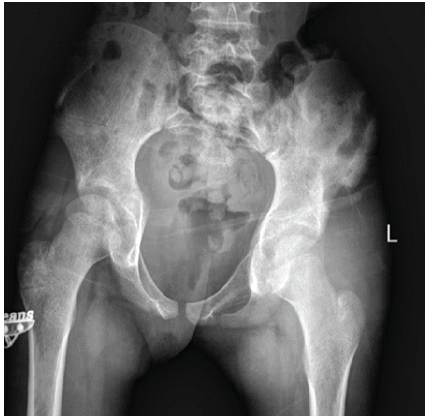
Figure 1: Pre-operative pelvic radiograph showing a normal left hip joint with no radiographic evidence of osteomyelitis or septic arthritis, despite significant clinical symptoms suggestive of a septic hip.
Ultrasonography of the left thigh and hip demonstrated a large, ill-defined, heterogeneously hypoechoic collection (7.2 × 2.7 × 7 cm) within the intermuscular planes of the proximal thigh. The collection appeared to extend superiorly toward the hip joint, although no definite bony involvement was identified. These findings, combined with refusal to bear weight and markedly elevated inflammatory markers, raised a strong suspicion of septic arthritis. Aspiration of the collection yielded frank pus. Given the strong clinical suspicion of septic arthritis, the child underwent urgent left hip arthrotomy. Intraoperatively, the hip joint was found to be normal, prompting reconsideration of the diagnosis. A contrast-enhanced MRI was subsequently performed, which demonstrated multiple peripherally enhancing collections beneath the left gluteus minimus and medius, with extension into intermuscular planes and involvement of the anterior rectus femoris. Marrow edema and enhancement were noted in the left iliac blade and ischial region, extending toward the sacroiliac joint. Significant surrounding muscular edema and mild pelvic free fluid were also observed. Except for a small reactive effusion, the hip joint showed no intra-articular enhancement or cartilage erosion (Fig. 2).
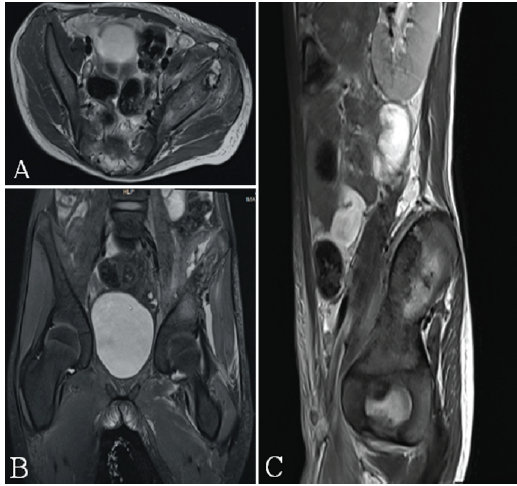
Figure 2: Contrast-enhanced magnetic resonance imaging of the pelvis demonstrating multiloculated abscesses and iliac osteomyelitis mimicking septic arthritis of the hip. (A) Axial image showing peripherally enhancing collections deep to the left gluteus minimus and medius with surrounding muscular edema. (B) Coronal image demonstrating marrow edema and enhancement of the left iliac blade with a cortical breach, through which pus is seen tracking inferiorly into the intermuscular planes around the hip, closely simulating septic arthritis. (C) Sagittal image further delineating the extent of intra- and extra-pelvic spread of infection, whereas the hip joint itself remains preserved without intra-articular enhancement.
Overall, the findings were consistent with osteomyelitis of the left ilium and ischium with associated soft-tissue abscesses, rather than septic arthritis. A post-operative ultrasound of the abdomen and pelvis revealed no intra-abdominal or pelvic collections. The culture of operative material grew methicillin-resistant Staphylococcus aureus (MRSA), sensitive to vancomycin, linezolid, and teicoplanin.
Treatment:
Based on the initial clinical picture, the child was started on empirical intravenous vancomycin and ceftriaxone. Surgical exploration revealed purulent material tracking through the subcutaneous and muscular layers lateral to the hip. Further exploration identified a cortical defect with bony erosion of the iliac/ischial region, from which pus was originating (Fig. 3).
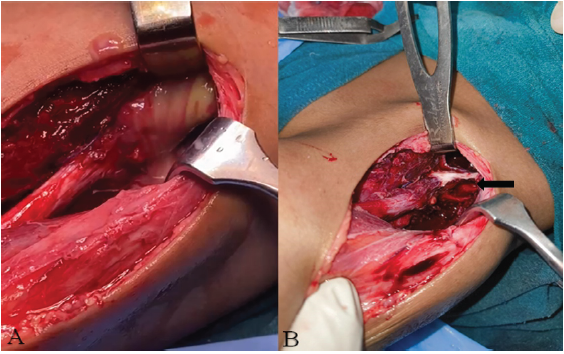
Figure 3: Intraoperative findings during surgical drainage. (A) Purulent material showed tracking from the pelvic cavity into the proximal thigh, indicating a communicating abscess extending from
the ilium. (B) Intraoperative exposure demonstrating the cortical defect in the ilium (arrow), consistent with underlying iliac osteomyelitis.
No intrapelvic abscess was identified on exploration performed with assistance from the pediatric surgery team. Following culture confirmation of MRSA, vancomycin was continued in adjusted doses. Within 48 hours, however, the child developed a diffuse erythematous rash along with rising creatinine levels (peaking at 2.8 mg/dL), suggesting multifactorial acute kidney injury, likely related to recent contrast exposure and concurrent vancomycin therapy. Vancomycin was discontinued and replaced with intravenous linezolid.
Outcome:
The child showed steady improvement during her hospital stay. Her pain reduced significantly, CRP dropped from 371 mg/L to 17 mg/L, and interval ultrasonography demonstrated decreasing soft-tissue collections. She gradually progressed to support ambulation and was able to walk short distances comfortably by discharge. Renal function was normalized with conservative care, and the drug-related rash resolved fully after switching to linezolid. In the weeks following discharge, she continued to recover without any recurrence of fever, swelling, or restriction of movement. The surgical site healed well, and serial clinical examinations showed no residual tenderness. Follow-up blood tests demonstrated normal inflammatory markers, and pelvic radiographs showed no new abnormalities, supporting good resolution of the infection. At her 12-month follow-up, the child had returned to full daily activities. She was able to walk, run, climb stairs, squat, and play outdoors without discomfort or limp (Fig. 4).

Figure 4: Post-operative clinical photograph showing the child walking comfortably without support, demonstrating resolution of pain and restoration of functional mobility following surgical drainage and appropriate antibiotic therapy.
Her parents reported no further episodes of pain or swelling. On examination, hip movements were full and painless, and both radiographs and blood tests showed no evidence of recurrence (Fig. 5). Overall, she achieved complete functional recovery.
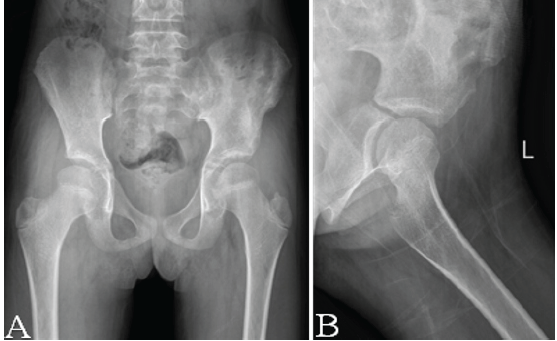
Figure 5: Follow-up radiographs of the pelvis showing interval recovery without recurrence of osteomyelitis. (A) Anteroposterior pelvic radiograph demonstrating maintained joint spaces,
intact cortical contours of the left ilium and acetabulum, and no new lytic lesions or periosteal reaction. (B) Lateral view of the left hip confirming preserved femoral head morphology and absence of soft-tissue swelling or osseous destruction. Overall, the images indicate satisfactory healing following treatment of iliac osteomyelitis.
Pelvic osteomyelitis in children poses a significant diagnostic challenge because its clinical presentation closely resembles that of septic arthritis of the hip. Fever, severe hip pain, limp, and inability to bear weight – features classically used to diagnose septic arthritis – are equally common in pelvic infections [1,2]. Other differential diagnoses, such as transient synovitis, pyomyositis, and deep pelvic abscesses, should also be considered in similar presentations. In our case, the child fulfilled nearly all classical criteria for septic arthritis, prompting urgent hip arthrotomy. The discovery of a completely normal hip joint intraoperatively underscores a phenomenon described in previous reports: pelvic osteomyelitis can convincingly mimic septic hip to the point of leading to non-therapeutic hip exploration [3]. This reinforces the need to re-evaluate the diagnosis when operative findings contradict clinical expectations. In retrospect, early MRI before surgical intervention may have helped identify the extra-articular source of infection and potentially avoided arthrotomy. Delayed diagnosis remains a hallmark of pelvic osteomyelitis, with earlier studies reporting delays ranging from 10 to 25 days due to non-specific symptoms and inconclusive early investigations [1,2,7]. Our case initially appeared typical for septic arthritis, but the rapid recurrence of symptoms and persistently elevated inflammatory markers compelled further evaluation. Although ultrasonography demonstrated a peri-hip collection, its inability to clearly identify the extra-articular origin may have contributed to diagnostic ambiguity, highlighting its limitations in deep pelvic infections. MRI ultimately revealed osteomyelitis of the ilium and ischium with adjacent soft-tissue abscesses – findings that are frequently occult on plain radiographs or ultrasound. MRI remains the most sensitive and specific modality for diagnosing pelvic osteomyelitis, enabling clear differentiation from intra-articular disease and identifying the full extent of infection [4,5,8]. However, access to MRI may be limited in resource-constrained settings, where careful clinical assessment and interpretation of initial investigations remain essential. An especially distinctive aspect of this case was the identification of a cortical breach in the iliac bone with pus tracking externally into the subcutaneous and muscular layers. While pelvic osteomyelitis can extend into surrounding tissues, frank cortical disruption visualized at surgery is uncommon because the rich cancellous blood supply of the pelvis typically limits sequestration [5,9]. This unusual morphological finding, combined with the child’s intense systemic inflammatory response, aligns with the increasingly recognized aggressive pattern of infections caused by MRSA [6,10]. Elevated CRP values approaching 400 mg/L, as observed in this case, are consistent with the more severe inflammatory phenotype associated with MRSA. Serial inflammatory markers showed a clear downward trend following intervention, correlating with clinical improvement. Management in this case was guided by dynamic clinical assessment rather than a fixed protocol, reflecting the complexity of atypical musculoskeletal infections and the need for individualized decision-making. Microbiological confirmation of MRSA guided targeted therapy; however, further characterization, such as strain typing and epidemiological profiling, was beyond the clinical scope of this case. However, management was further complicated by two additional factors that are rarely discussed in the context of pelvic osteomyelitis. First, the child developed contrast-induced acute kidney injury after MRI, necessitating careful renal monitoring and adjustment of nephrotoxic medications [11]. Second, during empiric therapy, she developed a vancomycin-induced rash, a recognized hypersensitivity reaction, requiring discontinuation of vancomycin and transition to linezolid [12]. This highlights the balance required between diagnostic necessity and treatment-related risks, particularly when managing deep-seated infections requiring both contrast imaging and potent antimicrobial therapy. Despite these complexities, the child improved with surgical drainage and targeted antibiotic therapy, achieving full functional recovery. This outcome highlights the importance of early recognition, timely imaging, and accurate microbiological diagnosis in reducing morbidity. It also underscores the need for heightened clinical vigilance when a child presents with features suggestive of septic arthritis but demonstrates discordant operative findings or an atypical clinical course. The patient remained asymptomatic at 1-year follow-up, with no evidence of recurrence, functional limitation, or radiological abnormality, supporting sustained resolution of infection. As this report describes a single patient, variability in presentation, organism virulence, and host response may limit broader applicability. Rather than advocating routine reliance on advanced imaging, this case emphasizes the importance of maintaining diagnostic flexibility, with continuous clinical reassessment when evolving findings do not align with initial assumptions.
Pelvic osteomyelitis in children remains a challenging diagnosis because its presentation often mirrors septic arthritis of the hip. This case demonstrates how convincingly pelvic infection can mimic intra-articular pathology, even leading to hip arthrotomy despite a normal joint. The presence of MRSA, a rare cortical breach with extrapelvic pus tracking, and additional complications such as contrast-induced acute kidney injury and vancomycin hypersensitivity further highlight the complex and unpredictable nature of pelvic infections in children. Early reconsideration of diagnosis when intraoperative findings are discordant, together with timely MRI and targeted antimicrobial therapy, is essential for preventing delayed treatment. Awareness of these atypical features can guide clinicians toward earlier recognition and improved outcomes in similar cases. As a single case report, these observations should be interpreted as a clinical illustration rather than a generalizable recommendation.
Pelvic osteomyelitis can closely mimic septic arthritis of the hip and may only be uncovered when intraoperative findings are incongruent with the initial diagnosis. A normal hip arthrotomy should prompt immediate evaluation for pelvic sources of infection, with MRI serving as the most reliable tool for early identification of deep pelvic involvement. Awareness of aggressive MRSA patterns and potential treatment-related complications is crucial for timely, effective management.
References
- 1. Kumar J, Ramachandran M, Little D, Zenios M. Pelvic osteomyelitis in children. J Pediatr Orthop B 2010;19:38-41. [Google Scholar] [PubMed]
- 2. Klein JD, Leach KA. Pediatric pelvic osteomyelitis. Clin Pediatr (Phila) 2007;46:787-90. [Google Scholar] [PubMed]
- 3. Kocialkowski C, Ryan W, Davis N. Case report of iliac osteomyelitis in a child, presenting as septic arthritis of the hip. J Orthop Case Rep 2014;4:19-21. [Google Scholar] [PubMed]
- 4. Takemoto RC, Strongwater AM. Pelvic osteomyelitis mimicking septic hip arthritis: A case report. J Pediatr Orthop B 2009;18:248-51. [Google Scholar] [PubMed]
- 5. Deore S, Bansal M. Pelvic osteomyelitis in a child – a diagnostic dilemma. J Orthop Case Rep 2018;8:86-8. [Google Scholar] [PubMed]
- 6. Kumar V, Barik S, Garg V, Raj V, Arora SS. A systematic review of pelvic infective osteomyelitis in children: Current state of evidence. J Trop Pediatr 2024;70:fmae043. [Google Scholar] [PubMed]
- 7. Tolley M, Morris A, Williams N. Pelvic osteomyelitis: Three unusual cases with predominantly abdominal symptoms. J Paediatr Child Health 2017;53:614. [Google Scholar] [PubMed]
- 8. Song KS, Lee SW, Bae KC. Key role of magnetic resonance imaging in the diagnosis of infections around the hip and pelvic girdle mimicking septic arthritis of the hip in children. J Pediatr Orthop B 2016;25:234-40. [Google Scholar] [PubMed]
- 9. Sun X, Lou Y, Wang X. The diagnosis of iliac bone destruction in children: 22 cases from two centres. Biomed Res Int 2016;2016:2131859. [Google Scholar] [PubMed]
- 10. Weber-Chrysochoou C, Corti N, Goetschel P, Altermatt S, Huisman TA, Berger C. Pelvic osteomyelitis: A diagnostic challenge in children. J Pediatr Surg 2007;42:553-7. [Google Scholar] [PubMed]
- 11. Wang C, Zhang C, Sun J, Yan R, Liu X, Jia L, et al. Risk of acute kidney injury following contrast-enhanced CT or MRI in a cohort of 3061 hospitalized children in China. BMC Pediatr 2024;24:400. [Google Scholar] [PubMed]
- 12. Martel TJ, Jamil RT, Afzal M. Vancomycin Infusion Reaction. [Updated 2025 Feb 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482506/ [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult
July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult June 1, 2026 Cortical Window Osteotomy for Diagnostic Biopsy in Iliac Osteomyelitis: A Case Report and Technical Note
June 1, 2026 Cortical Window Osteotomy for Diagnostic Biopsy in Iliac Osteomyelitis: A Case Report and Technical Note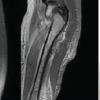 May 1, 2026 Acute Osteomyelitis with Deep Vein Thrombosis in Children: A Case Series of MRSA-Associated Infections
May 1, 2026 Acute Osteomyelitis with Deep Vein Thrombosis in Children: A Case Series of MRSA-Associated Infections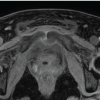 February 1, 2026 When MRSA Misleads: Tuberculous Osteomyelitis of the Anterior Pelvic Bones
February 1, 2026 When MRSA Misleads: Tuberculous Osteomyelitis of the Anterior Pelvic Bones