
Osteotomy-assisted open reduction and internal fixation through an anterolateral approach can restore articular congruity and achieve excellent functional outcomes even in delayed McKee Type IV capitellum–trochlea malunions.
Dr. Rajath S Shetty, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: shettyrajath22@gmail.com
Abstract
Introduction: Coronal shear fractures of the distal humerus are rare, comprising <1% of elbow fractures. McKee Type IV fractures involve both the capitellum and lateral trochlea. These injuries are uncommon and may result in stiffness and functional impairment if diagnosis is delayed or treated conservatively.
Case Report: A 15-year-old boy presented 6 months after an untreated McKee Type IV coronal shear fracture of the distal humerus with pain, stiffness, and restricted elbow motion. Radiographs and computed tomography demonstrated a malunited shear fragment with a “double-arc” sign. Osteotomy through the malunited fracture plane was performed through an anterolateral approach, followed by fixation with headless compression screws. Early mobilization was initiated postoperatively. At 18 months, the patient achieved a flexion–extension arc of 0°–120°, full forearm rotation, and radiological union. The Mayo Elbow performance score was 95, and the disabilities of the arm, shoulder, and hand score was 4.2, indicating excellent functional recovery with minimal disability. No radiographic signs of avascular necrosis were noted.
Conclusion: Osteotomy-assisted open reduction through an anterolateral approach appears to be a viable surgical option for late-presenting McKee Type IV coronal shear malunions, enabling restoration of joint anatomy and function. However, conclusions are limited by the single-case design, absence of comparative analysis, and lack of long-term follow-up.
Keywords: McKee Type IV fracture, capitellum fracture, coronal shear fracture, anterolateral approach, osteotomy-assisted fixation.
Coronal shear fractures of the distal humerus are uncommon injuries, accounting for <1% of all elbow fractures [1,2]. McKee et al. expanded the Bryan and Morrey classification to include Type IV fractures, characterized by fracture extension from the capitellum to the lateral trochlea. As these fractures involve the articular surface, early anatomical reduction and stable fixation are essential to restore joint congruity and allow early mobilization [3]. Delayed diagnosis or conservative management can result in malunion, leading to pain, stiffness, and functional limitation. Reports of malunited capitellum fractures are rare, and literature on malunited McKee Type IV variants is extremely limited. Fragment excision has historically been used but may result in valgus instability and early degenerative changes [4]. The anterolateral approach offers improved visualization of both the capitellum and trochlea, facilitating anatomical reduction and optimal screw placement [5].
Given the rarity of this injury pattern, evidence remains limited and largely confined to isolated case reports. We present a rare case of a late-presenting McKee Type IV capitellum–trochlea malunion managed with osteotomy-assisted open reduction and internal fixation. To the best of our knowledge, reports describing osteotomy-assisted reconstruction of malunited McKee Type IV fractures in adolescents are extremely limited.
A 15-year-old right-hand–dominant boy presented with pain and restricted movement of the right elbow for 6 months following a fall on an outstretched hand. He had been initially treated with immobilisation in an above-elbow plaster for 6 weeks. On clinical examination, elbow flexion–extension ranged from 70° to 90°, with markedly restricted pronation and supination. Localised tenderness was present over the lateral distal humerus, with no neurovascular deficit (Fig. 1).

Figure 1: Clinical photograph showing restricted elbow flexion and extension (70°–90°) and significantly limited forearm rotation. The radiograph shows a malunited capitellum and trochlea shear fragment with the “double-arc” sign.
Radiographs revealed a malunited coronal shear fragment involving the capitellum extending into the trochlea, demonstrating the “double-arc” sign (Fig. 1). Computed tomography confirmed a McKee Type IV fracture pattern with anterosuperior displacement of the fragment (Fig. 2).
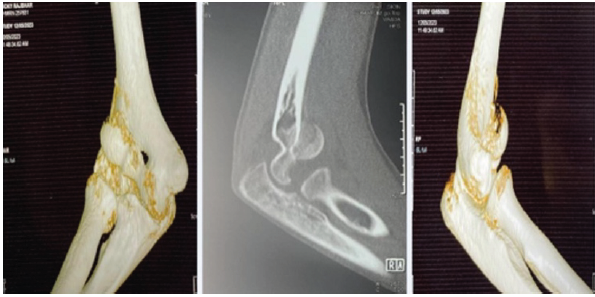
Figure 2: Preoperative computed tomography images illustrating a McKee Type IV coronal shear fracture involving the capitellum and lateral trochlea.
Surgical intervention was performed using an anterolateral approach. The interval between the brachialis and brachioradialis was developed, and the radial nerve was identified and protected. Osteotomy was performed along the malunited fracture plane to mobilise the fragment. The articular surface was anatomically reduced and provisionally fixed with two 1.5 mm K-wires and stabilized using three 3.5 mm Herbert headless compression screws are placed anterior-to-posterior (Figs. 3 and 4).
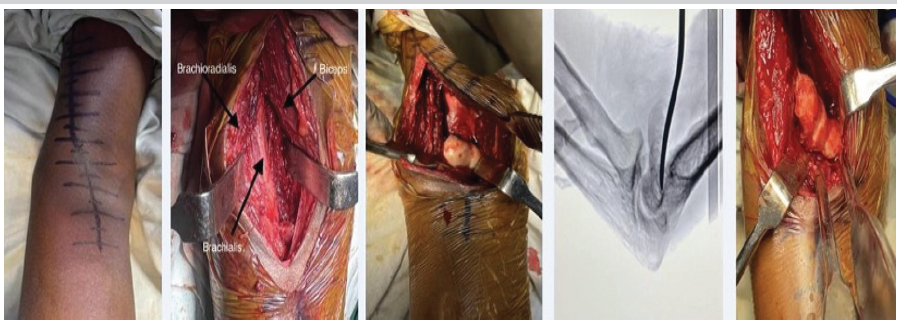
Figure 3: Intraoperative photographs demonstrating the anterolateral approach, exposure of the malunited fragment, osteotomy through the original fracture plane, and the retrieved osteotomized fragment.
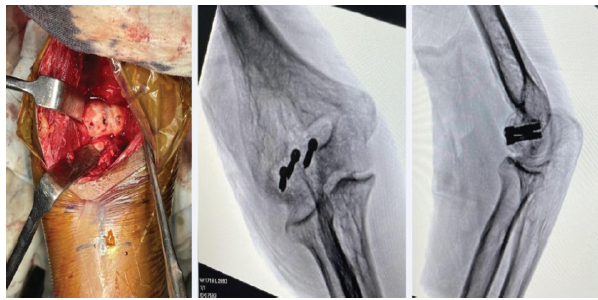
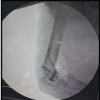
Figure 4: Intraoperative, clinic, and fluoroscopic images showing anatomical reduction and fixation with three 3.5-mm Herbert headless compression screws.
Intraoperative fluoroscopy confirmed satisfactory reduction and fixation.
Operative time and intraoperative blood loss were within acceptable limits, although not formally quantified. No intraoperative complications were encountered. Postoperatively, the elbow was immobilized in a posterior splint for 2 weeks. Active-assisted mobilization was initiated thereafter, followed by strengthening exercises at 6 weeks and return to unrestricted activity at 12 weeks. At 18 months follow-up, the patient demonstrated a flexion–extension arc of 0°–120°, full pronation–supination, and complete radiological union. No radiographic signs of avascular necrosis were noted; however, magnetic resonance imaging (MRI) was not performed to assess subclinical changes (Fig. 5).
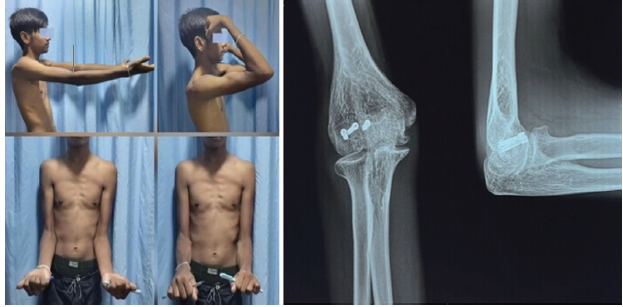
Figure 5: Follow-up clinical photos at 18 months showing near-normal elbow motion and radiographs demonstrating complete union.
The Mayo Elbow Performance Score (MEPS) was 95 (excellent), and the Disabilities of the Arm, Shoulder, and Hand (DASH) score was 4.2, indicating minimal disability and excellent functional recovery.
McKee Type IV coronal shear fractures are rare injuries involving both the capitellum and trochlea, presenting significant surgical challenges [1,2]. These fractures disrupt the anterior articular surface of the distal humerus, necessitating anatomical reduction and stable fixation to restore function [3,6]. Malunions are uncommon due to the preference for early surgical intervention. Literature on osteotomy-assisted reconstruction of malunited McKee Type IV fractures is sparse. Jeevannavar et al. reported successful corrective osteotomy in Type I fractures [7], but evidence for Type IV malunions remains limited. Several studies have reported favourable outcomes following acute fixation. Tanrıverdi et al. demonstrated excellent MEPS scores with headless screw fixation [3], while Wiktor and Tomaszewski reported excellent functional recovery in adolescents [8]. Dubberley et al. emphasized stable fixation in combined capitellum–trochlea fractures [9]. Despite a delayed presentation, our patient achieved outcomes comparable to those reported in acute cases.
While alternative strategies such as fragment excision or arthroplasty have been described, particularly in chronic cases, these may compromise joint stability and predispose to early degenerative changes. Anatomical reconstruction, although technically demanding, preserves joint congruity and function. The anterolateral approach was selected due to superior visualization of the anterior distal humerus, particularly when the fracture extends medially. Yu et al. demonstrated improved exposure and fixation using this approach [5]. Biomechanical studies support perpendicular screw placement for optimal stability [10]. Osteotomy through a malunited fracture is technically challenging, requiring precise recreation of the fracture plane and management of soft tissue contractures. The success of this technique is highly dependent on surgical expertise. In this case, excellent functional recovery without avascular necrosis demonstrates that delayed reconstruction can yield favourable outcomes when performed meticulously. The combined use of MEPS and DASH scoring provides both clinician-based and patient-reported outcome assessment, enhancing the robustness of functional evaluation. Despite encouraging outcomes, certain limitations must be acknowledged.
Limitations of the study:
This report has several important limitations. It represents a single case, limiting generalizability and introducing potential selection bias, particularly as the patient was young with good healing potential. No control group or comparison with alternative treatment methods, such as fragment excision or arthroplasty, was included.
Although the 18-month follow-up demonstrates excellent functional recovery, long-term outcomes such as post-traumatic arthritis remain unknown. Advanced imaging, such as serial computed tomography scans or MRI, was not performed postoperatively to objectively assess articular congruity or detect subclinical avascular necrosis. While DASH scoring was included, a broader range of patient-reported outcome measures could further strengthen functional assessment. The technique is operator-dependent, and factors such as learning curve, operative difficulty, and intraoperative variables were not systematically quantified. Biomechanical validation of the fixation strategy in delayed reconstruction scenarios was not performed. In addition, rehabilitation protocols were not compared with alternative regimens. Given the rarity of McKee Type IV malunions, extrapolation of findings is limited, and there is potential for publication bias favouring successful outcomes. Further multicentric studies with larger cohorts and long-term follow-up are required to validate this approach.
Osteotomy-assisted open reduction through an anterolateral approach, combined with stable headless screw fixation, appears to be a viable surgical option for late-presenting McKee Type IV coronal shear malunions. This technique facilitates restoration of articular anatomy and function even in delayed cases. However, given the single-case design and lack of comparative and long-term data, further studies are required before this approach can be recommended as a standard treatment.
Late-presenting McKee Type IV capitellum coronal shear fractures can be effectively managed with osteotomy-assisted open reduction and internal fixation through an anterolateral approach. Anatomical restoration combined with stable fixation can result in excellent functional outcomes, even in delayed presentations.
References
- 1. Schmidt I. A complicated course of a coronal shear fracture type IV of the distal humerus resulting in resurfacing radiocapitellar joint replacement. Open Orthop J 2017;11:248-54. [Google Scholar] [PubMed]
- 2. Lamas C, Grau A, Almenara M, Trigo L. Coronal shear fractures of the capitellum and trochlea: Interobserver variability in classification and need for CT for surgical planning. JSES Int 2020;5:314-9. [Google Scholar] [PubMed]
- 3. Tanrıverdi B, Kural C, Altun S. Capitellum fractures: Treatment with headless screws and outcomes. Jt Dis Relat Surg 2020;31:291-7. [Google Scholar] [PubMed]
- 4. Jeevannavar SS, Shenoy KS, Daddimani RM. Corrective osteotomy through fracture site and internal fixation with headless screws for type I capitellar malunion. BMJ Case Rep 2013;2013:bcr2013009308. [Google Scholar] [PubMed]
- 5. Yu T, Tao H, Xu F, Hu Y, Zhang C, Zhou G. Comparison of lateral versus anterolateral approach with Herbert screw fixation for capitellum fractures. J Orthop Surg Res 2019;14:230. [Google Scholar] [PubMed]
- 6. Ring D, Jupiter JB. Fractures of the capitellum and trochlea. J Bone Joint Surg Am 2002;84:1639-46. [Google Scholar] [PubMed]
- 7. Wiktor L, Tomaszewski R. Humeral capitellum fractures in adolescents treated with open reduction and internal fixation. Adv Orthop 2022;2022:4012125. [Google Scholar] [PubMed]
- 8. Dubberley JH, Faber KJ, MacDermid JC, Patterson SD, King GJ. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am 2006;88:46-54. [Google Scholar] [PubMed]
- 9. Mighell MA, Harkins D, Klein D, Schneider S, Frankle M. Technique for internal fixation of capitellum and lateral trochlea fractures. J Orthop Trauma 2006;20:699-704. [Google Scholar] [PubMed]
- 10. Elkowitz SJ, Polatsch DB, Egol KA, Kummer FJ, Koval KJ. Capitellum fractures: A biomechanical evaluation of three fixation methods. J Orthop Trauma 2002;16:503-6. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report
July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach June 1, 2026 Acute Capitellum Fracture with Distal Radio-ulnar Joint Disruption: An Atypical Variant of an Essex Lopresti Injury – Case Report
June 1, 2026 Acute Capitellum Fracture with Distal Radio-ulnar Joint Disruption: An Atypical Variant of an Essex Lopresti Injury – Case Report April 1, 2026 Functional and radiological outcome of capitellum fracture fixation with headless screws through lateral approach to elbow, a prospective observational study
April 1, 2026 Functional and radiological outcome of capitellum fracture fixation with headless screws through lateral approach to elbow, a prospective observational study