
Limb-preserving reconstructive surgery can restore functional gait and shoe wear in adolescent patients with foot ectrodactyly.
Centenarro Jose S Meceda, Department of Orthopaedics, Jose R. Reyes Memorial Medical Center, Manila, Philippines. E-mail: centenarrojose@gmail.com
Abstract
Introduction: Foot ectrodactyly is a rare congenital malformation characterized by the absence of the central rays, resulting in a cleft foot deformity that may impair shoe wear, function, and cosmesis.
Case Report: We report an 18-year-old Filipino female with bilateral isolated foot ectrodactyly who presented with progressive pain during ambulation and difficulty wearing conventional footwear. Radiographs demonstrated the absence and hypoplasia of the second and third rays. A limb-preserving reconstructive procedure was performed on the symptomatic right foot, consisting of proximal first metatarsal closing wedge osteotomy, hallux interphalangeal joint arthrodesis, and soft-tissue web-space reconstruction.
Conclusion: At 6 months postoperatively, the patient achieved pain relief, improved forefoot alignment, and the ability to wear standard shoes and ambulate normally. This case highlights the role of reconstructive surgery in skeletally mature patients with foot ectrodactyly.
Keywords: Ectrodactyly, cleft foot, reconstructive surgery, adolescent, foot deformity.
Foot ectrodactyly, also referred to as cleft foot deformity, is a rare congenital condition characterized by the absence or hypoplasia of the central digital rays, resulting in a widened forefoot and a median cleft [1,2]. The reported incidence is approximately 1 in 90,000–100,000 live births. Clinically, patients may experience difficulty with footwear, altered foot morphology, gait disturbance, and cosmetic concerns, which often become more pronounced with increasing age and functional demand [3]. Surgical management of foot ectrodactyly is highly individualized and depends on patient age, severity of deformity, skeletal maturity, and functional goals. Some reported surgical options include ray amputation with cleft narrowing, soft-tissue reconstruction, and limb-preserving techniques aimed at improving forefoot alignment and shoe wear [4]. Previous surgical literature emphasizes that reconstruction is guided by dual objectives of restoring function and improving cosmesis, as demonstrated in medium to long-term follow-up series [5]. Simplified cleft-closure techniques have been proposed, particularly in pediatric patients, to achieve reliable narrowing of the forefoot when earlier flap-based approaches produced suboptimal results [6]. Over recent decades, a trend toward operative management has been noted, with primary goals centered on achieving a plantigrade, shoeable, and functionally stable foot while addressing esthetic concerns [7]. Studies have described multiple technical approaches, including simple closure, double pedicelled flap reconstruction, and silicone block insertion, with reported cosmetic complications such as widening, hypertrophic scarring, and toe overlap, particularly in cases involving multiple central ray deficiencies [8]. Additional reconstructive strategies have been reported to address transverse instability and metatarsal divergence. Metatarsal wedge resection with screw fixation combined with skin syndactyly has been shown in small series to improve forefoot narrowing and facilitate commercial shoe wear with high patient satisfaction [9]. In selected pediatric cases, a suture-button construct has been described to restore and maintain intermetatarsal stability while minimizing rigid hardware use [10]. For severe deformities, microsurgical reconstruction through microvascular toe transfer has been reported, with long-term follow-up demonstrating acceptable growth, symmetry, and cosmetic appearance in carefully selected patients [11]. Retrospective series further suggest that severity-based classification systems may aid in operative decision-making and that not all cleft feet require surgical correction, as some untreated cases may remain functionally satisfactory [12]. Despite the diversity of techniques and reported outcomes, no universally accepted surgical algorithm or standardized treatment protocol has been established. In adolescents and skeletally mature patients, management is more complex due to established foot structure and biomechanics, expectations regarding cosmesis, and the need to preserve foot length and push-off strength. Limb-preserving reconstructive approaches combining osteotomies, arthrodesis, and soft-tissue reconstruction have been described as viable alternatives to amputation in selected patients, with the primary goal of improving shoe wear and functional outcomes [3]. Literature addressing such approaches in adolescent patients remains limited. This case report aims to contribute to the existing evidence by describing reconstructive surgery in an adolescent with symptomatic foot ectrodactyly.
An 18-year-old Filipino female presented with long-standing bilateral foot deformities associated with intermittent pain during ambulation and difficulty wearing conventional footwear. The deformities were congenital in onset and had been noted at birth; however, no medical or surgical intervention had been pursued during childhood. The patient reported the onset of intermittent forefoot pain at approximately 10 years of age, described as mild-to-moderate in intensity (Visual Analog Scale [VAS] score 3/10), particularly during prolonged walking and standing. Symptoms initially resolved spontaneously but gradually recurred with increasing frequency. By late adolescence, she noted worsening discomfort affecting the right foot, increasing difficulty with prolonged ambulation, and inability to comfortably fit the right foot into standard closed footwear. Despite these symptoms, she remained able to ambulate independently without gait asymmetry. The left foot, although similarly affected by congenital deformity, remained functional and was able to accommodate conventional footwear without significant pain or limitation. As a result, surgical intervention for the left foot was not pursued. On physical examination, both feet demonstrated deep median clefts consistent with ectrodactyly, with the absence of the central digits. The right foot exhibited forefoot widening, lateral deviation of the hallux, clinical hallux interphalangeus, and cutaneous syndactyly of the fourth and fifth toes (Fig. 1).

Figure 1: Pre-operative clinical photograph of the right foot demonstrating a deep median cleft consistent with ectrodactyly, absence of the central digits, forefoot widening, hallux interphalangeus, and cutaneous syndactyly of the fourth and fifth toes.
The left foot demonstrated a similar anatomic cleft pattern, though narrower in configuration, and was likewise noted to have hallux interphalangeus; however, overall alignment and function remained acceptable. The plantar skin was intact bilaterally without callosities or ulceration. Neurovascular examination was normal. Radiographs of the right foot demonstrated hypoplasia of the second metatarsal, which was medially deviated and fused to the base of the first metatarsal, as well as hypoplasia of the third metatarsal with absence of the phalanges of the second and third toes. These findings resulted in widening of the intermetatarsal space between the first and fourth rays (Fig. 2).

Figure 2: Pre-operative radiograph of the right foot demonstrating hypoplasia of the second metatarsal with medial deviation and fusion to the base of the first metatarsal, hypoplasia of the third metatarsal, and absence of the phalanges of the second and third toes, resulting in widening of the intermetatarsal space between the first and fourth rays.
No degenerative changes were observed in the hindfoot or ankle joints. Given the patient’s skeletal maturity, right-sided symptoms, and desire to improve comfort during ambulation and shoe wear while preserving foot length, a limb-preserving reconstructive approach was selected for the right foot only. Surgical intervention on the left foot was deferred due to preserved function and satisfactory shoe accommodation.
Surgical technique:
After informed consent was obtained, the patient was brought to the operating room and positioned supine. A pneumatic tourniquet was applied to the thigh, and the right lower extremity was prepared and draped in a sterile manner. Fluoroscopy was utilized intraoperatively for guidance. A dorsal-medial approach to the forefoot was performed to expose the first ray while preserving surrounding soft-tissue attachments. A proximal closing wedge osteotomy of the first metatarsal was performed to correct metatarsal malalignment and reduce the widened intermetatarsal angle between the first and fourth rays. The osteotomy was carefully planned to achieve controlled realignment while minimizing excessive shortening of the first ray. Reduction was achieved under fluoroscopic guidance and stabilized using screw fixation. Following correction of metatarsal alignment, persistent hallux interphalangeus was noted. An interphalangeal joint arthrodesis of the hallux was therefore performed through a medial approach. The joint surfaces were prepared in the standard fashion, and fusion was achieved in a functional position to correct the deformity and enhance first-ray stability. Fixation was accomplished using compression screw fixation. After narrowing of the intermetatarsal gap, local soft-tissue reconstruction of the web space was performed through a longitudinal dorsoplantar incision between the first and fourth rays, using the adjacent medial skin of the first ray and lateral skin of the fourth ray. The mobilized skin edges were approximated with simple interrupted sutures to recreate a functional and cosmetically acceptable web space. Hemostasis was achieved, and the wound was closed in layers. A sterile dressing and immobilization were applied before tourniquet release.
Outcome and follow-up:
The post-operative course was uneventful, and the patient was discharged on post-operative day 3 with immobilization and a structured rehabilitation program. The post-operative protocol consisted of non-weight-bearing for the first 4 weeks, followed by heel weight-bearing for the subsequent 4 weeks. Full weight-bearing was permitted thereafter once radiographic evidence of union was confirmed. Early post-operative clinical examination demonstrated satisfactory correction of forefoot alignment and web-space reconstruction (Fig. 3).

Figure 3: Post-operative photograph of the right foot demonstrating improved forefoot alignment, narrowing of the intermetatarsal gap, and reconstructed central web space following limb-preserving reconstructive surgery.
Post-operative radiographs confirmed satisfactory correction of forefoot alignment, restoration of functional foot length, and appropriate positioning of fixation devices (Fig. 4).

Figure 4: Post-operative radiograph of the right foot demonstrating correction of forefoot alignment following proximal first metatarsal closing wedge osteotomy and hallux interphalangeal joint arthrodesis with stable internal fixation.
At follow-up, the patient reported complete resolution of pain in the operative foot (VAS score 0/10), improved comfort during prolonged ambulation, and the ability to wear conventional closed footwear without difficulty. At 6 months post-operatively, clinical appearance demonstrated maintained correction and improved cosmetic contour (Fig. 5).

Figure 5: Photograph of the right foot at 6 months postoperatively demonstrating maintained correction, improved cosmetic appearance, and a well-formed central web space.
Follow-up radiographs showed stable fixation of the first metatarsal osteotomy and successful fusion of the hallux interphalangeal joint without complications (Fig. 6). The patient remained able to ambulate normally without gait asymmetry.

Figure 6: Radiographs of the right foot at 6 months postoperatively demonstrating stable fixation of the first metatarsal osteotomy and successful fusion of the hallux interphalangeal joint without complication.
This case highlights the management of symptomatic foot ectrodactyly in an adolescent patient, where the primary functional issues were pain, impaired shoe wear, and altered forefoot alignment. Limb-preserving reconstructive surgery successfully addressed these concerns, resulting in pain relief, restoration of gait, and the ability to wear conventional footwear. A case report on foot ectrodactyly described a pediatric foot ectrodactyly patient treated with ray amputation and soft-tissue reconstruction to narrow the cleft and improve cosmesis [1]. While effective in younger children, ray amputation sacrifices foot length. It may lead to compromise of push-off strength, which can be less acceptable in skeletally mature individuals with higher functional expectations and lesser biomechanical and anatomic adaptability. Medium to long-term follow-up data from early studies demonstrated that cleft foot repair aims to improve both functional alignment and cosmetic appearance, with generally satisfactory outcomes reported over several years of follow-up [5]. These reports emphasized narrowing of the cleft and improvement in forefoot contour as primary surgical goals. Simplified cleft-closure techniques have been described, particularly in pediatric patients, to achieve reliable approximation of the metatarsals and narrowing of the forefoot [6]. These techniques were proposed as modifications of earlier flap-based approaches and focused on technical reproducibility and reduction of soft-tissue tension. Comparative studies evaluating simple closure, double-pedicled flaps, and silicone block insertion have documented variable cosmetic outcomes, including cleft widening, hypertrophic scarring, and toe malalignment in some patients [8]. These findings illustrate that technique selection influences long-term esthetic results. Additional strategies addressing metatarsal divergence have been reported. A small case series described metatarsal wedge resection with screw fixation and skin syndactyly, noting improved forefoot narrowing and patient satisfaction with shoe wear [9]. In a separate pediatric case report, a suture-button construct was used to maintain intermetatarsal stability, with short-term maintenance of correction observed [10]. For more extensive deformities, microvascular toe transfer has been described, with 8-year follow-up demonstrating continued growth and acceptable cosmetic appearance in the reconstructed foot [11]. Retrospective analyses have also proposed classification-based approaches to guide operative decision-making and reported that some untreated cleft feet remained functionally acceptable [9]. Review literature further reiterates that surgical management primarily seeks to achieve a plantigrade, shoeable foot while improving appearance, although no standardized treatment protocol has been established [7]. Various reconstructive strategies have also been described for cleft foot deformities with central ray deficiencies, including soft-tissue flap techniques designed to achieve web space narrowing and improved cosmesis. [13]. Collectively, the literature reflects multiple operative techniques with reported functional and cosmetic improvement but without a universally accepted or standardized surgical algorithm. In this patient, a reconstructive approach was done, given skeletal maturity, unilateral symptoms, and the desire to preserve foot length and biomechanics. Bony correction through metatarsal osteotomy restored forefoot alignment and first-ray stability, while soft-tissue reconstruction improved forefoot contour and web-space formation. Similar limb-preserving strategies have been reported in the literature as effective options for improving shoe wear and functional outcomes in selected patients with ectrodactyly [3]. Adolescents with foot ectrodactyly often face unique functional and psychosocial challenges, including difficulty with prolonged ambulation, inability to wear standard footwear, and self-consciousness related to foot appearance [8]. Surgical success in this population should therefore be defined not only by radiographic correction but also by functional independence, footwear tolerance, and psychosocial well-being. In the present case, the patient’s ability to resume normal daily activities and wear conventional shoes represented a meaningful improvement in quality of life. This report is limited by its single-patient design and relatively short follow-up period. Long-term outcomes of reconstructive surgery for foot ectrodactyly in adolescents remain insufficiently studied. Future research, including larger case series and longer follow-up, is needed to define better indications, optimal surgical techniques, long-term functional and psychosocial outcomes, while considering that surgical intervention is still highly dependent on the patient’s presentation. Comparative studies between ray amputation and limb-preserving reconstruction may further guide surgical decision-making in skeletally mature patients. Therefore, the conclusions drawn from this study should be interpreted with caution. Despite these limitations, this case contributes to clinical practice by demonstrating that limb-preserving reconstructive surgery can be a viable and effective option for adolescent or skeletally mature patients with symptomatic foot ectrodactyly. For surgeons managing similar cases, careful patient selection and a focus on functional goals, particularly shoe wear, gait, and psychosocial well-being, are essential.
Reconstructive bony and soft-tissue procedures can provide meaningful functional and cosmetic improvement in adolescent patients with foot ectrodactyly. In skeletally mature individuals, limb-preserving surgery represents an effective alternative to ray amputation, particularly when functional outcomes, shoe wear, and psychosocial considerations are the primary concerns.
In adolescents with symptomatic foot ectrodactyly, limb-preserving reconstructive surgery can provide meaningful improvement in pain, forefoot alignment, and ability to wear conventional footwear while maintaining foot length and biomechanics. Surgical management should be individualized, with intervention primarily indicated for patients with functional limitations rather than cosmesis alone.
References
- 1. Raza S, Rehman S, Toor Z, Naeem R, Qureshi SA, Ahmed M, et al. Surgical management of ectrodactyly-associated foot deformity in a child: A case report. J Med Case Rep 2025;19:452. [Google Scholar] [PubMed]
- 2. Penchaszadeh VB, De Negrotti TC. Ectrodactyly-ectodermal dysplasia-clefting (EEC) syndrome: Dominant inheritance and variable expression. J Med Genet 1976;13:281-4. [Google Scholar] [PubMed]
- 3. Wojcicki P, Wysocki M, Wojcicka K. Ectrodactyly-ectodermal dysplasia-clefting syndrome-plastic surgeon’s considerations. J Craniofac Surg 2010;21:1388-92. [Google Scholar] [PubMed]
- 4. Nirmala SV, Chilamakuri S, Pavuluri C, Nuvvula S, Veluru S. Ectrodactyly: A rare anomaly of limbs. J Dr YSR Univ Health Sci 2015;4:53-5. [Google Scholar] [PubMed]
- 5. Sumiya N, Onizuka T. Seven years’ survey of our new cleft foot repair. Plast Reconstr Surg 1980;65:447-59. [Google Scholar] [PubMed]
- 6. Wood VE, Peppers TA, Shook J. Cleft-foot closure: A simplified technique and review of the literature. J Pediatr Orthop 1997;17:501-4. [Google Scholar] [PubMed]
- 7. Choudry Q, Kumar R, Turner PG. Congenital cleft foot deformity. Foot Ankle Surg 2010;16:e857. [Google Scholar] [PubMed]
- 8. Tani Y, Ikuta Y, Ishida O. Surgical treatment of the cleft foot. Plast Reconstr Surg 2000;105:1997-2002. [Google Scholar] [PubMed]
- 9. Talusan PG, Telles C, Perez JL, Reach JS Jr. Treatment of cleft foot deformity with a suture-button construct in the pediatric foot: A case report. Foot Ankle Int 2013;34:1299-304. [Google Scholar] [PubMed]
- 10. Sunagawa T, Kimori K, Ikuta Y, Ishida O, Tani Y. Microvascular toe transfer for cleft-foot plasty: Eight-year follow-up. J Reconstr Microsurg 2002;18:83-5. [Google Scholar] [PubMed]
- 11. Lejman T, Michno P. [Surgical treatment of congenital cleft foot]. Chir Narzadow Ruchu Ortop Pol 1998;63:475-8. [Google Scholar] [PubMed]
- 12. Abraham E, Waxman B, Shirali S, Durkin M. Congenital cleft-foot deformity treatment. J Pediatr Orthop 1999;19:404-10. [Google Scholar] [PubMed]
- 13. Takagi S, Kadomatsu K. The flap-bag technique: A new closure technique for treatment of cleft foot deformities with two central ray deficiencies. JPRAS Open 2019;21:35-42. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Cleft Hand and Foot Syndrome: A Report of Three Cases with Review of Literature
November 1, 2025 Cleft Hand and Foot Syndrome: A Report of Three Cases with Review of Literature July 1, 2026 Cadaveric Dissection of Adult Neglected Talipes Equinovarus
July 1, 2026 Cadaveric Dissection of Adult Neglected Talipes Equinovarus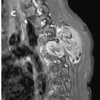 June 1, 2026 Adolescent Paraspinal Lipoblastoma: A Case Report
June 1, 2026 Adolescent Paraspinal Lipoblastoma: A Case Report May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report
May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report