
Periprosthetic joint infection leading to multiple revision procedures compromises soft tissue integrity and predisposes to recurrent instability of even a constrained total hip replacement. A novel, previously unreported failure interface exists at the junction between the factory-assembled constrained liner insert and the bipolar head, occurring in the absence of locking ring failure and distinct from the well-described failure modes – and should be considered in the evaluation of recurrent instability following revision total hip arthroplasty with constrained liners. In complex revision scenarios with compromised abductors and prior infection, patient education regarding activity restrictions and strict follow-up compliance are as important as the technical aspects of surgery.
D Naveen Kumar, Department of Orthopaedics, Parvathy Hospital, Chennai, Tamil Nadu, India. E-mail: nknaveenkarthik@gmail.com
Abstract
Introduction: Constrained acetabular liners are used as a salvage option for recurrent instability in revision total hip arthroplasty (THA). While failure mechanisms, including pelvic fixation loss, liner-shell dissociation, biomaterial fracture, and femoral head dislocation, are described in the literature, failure at the interface between the constrained liner insert and the bipolar head remains underreported.
Case Report: A 45-year-old male factory worker presented 7 weeks after right hip hemiarthroplasty with signs of periprosthetic joint infection and dislocation. He underwent staged treatment including wound debridement, antibiotic cement spacer placement, and revision THA with a constrained liner. The patient subsequently experienced recurrent instability necessitating a second revision. Intraoperatively, the failure was identified at the factory-assembled constrained liner insert-bipolar head junction without any locking ring fracture. This represents a previously undescribed failure interface in constrained THA.
Conclusion: This case highlights a novel anatomical failure interface in constrained THA systems. Surgeons must be aware that dissociation at the constrained liner insert-bipolar head junction can occur independently of locking ring failure, particularly in multiply-revised hips with impingement. Careful implant selection, optimized component positioning, and rigorous rehabilitation, compliance are critical to long-term success.
Keywords: Constrained acetabular liner, revision total hip arthroplasty, periprosthetic joint infection, instability, ring failure, bipolar head dissociation.
Dislocation following total hip arthroplasty (THA) is one of the most challenging complications, occurring in up to 20% of revision cases [1]. Constrained acetabular liners have emerged as a salvage option for high-risk patients with recurrent instability, abductor deficiency, cognitive dysfunction, or no identifiable correctable cause of dislocation [2,3]. While they successfully reduce redislocation rates, their use is tempered by a defined spectrum of mechanical failure modes. Yun et al. described four failure mechanisms, namely, failure of fixation to the pelvis, dissociation between the constraining liner and metal shell, biomaterial failure, and dislocation of the femoral head from the constrained liner [4]. Cooke et al. classified similar failure types and emphasized impingement as a unifying underlying mechanism [5]. Ward et al. described a novel complication of complete dissociation of the polyethylene component in a dual-mobility bearing following closed reduction, highlighting that previously undescribed failure interfaces can and do occur with newer implant designs [6]. To the best of our knowledge, no prior report has documented failure specifically at the factory-assembled junction between the constrained liner insert and the bipolar head, in the absence of locking ring fracture. We present such a case, occurring in the context of multiply-revised THA following periprosthetic joint infection (PJI), and discuss the mechanism, management, and implications.
A 45-year-old male factory worker presented to our emergency department 7 weeks after undergoing right hemiarthroplasty for a right neck of femur fracture sustained in a slip-and-fall accident. He complained of pain and swelling over the right hip with seropurulent discharge from the wound. He denied fever, cough, breathlessness, or constitutional symptoms. His history was significant for a seizure disorder but he was not on any current medications. He was a non-smoker and non-alcoholic. Clinical examination revealed diffuse swelling over the right hip, which was held in a position of flexion, adduction, and internal rotation. Tenderness was present along the anterior joint line with a visible discharging sinus. Range of motion was painfully restricted. Distal pulses were intact bilaterally, with no neurovascular deficit. Laboratory investigations revealed elevated inflammatory markers consistent with infection. Plain radiographs revealed a posteriorly dislocated hemiarthroplasty prosthesis (Fig. 1).

Figure 1: Anteroposterior pelvis radiograph showing right hip hemiarthroplasty with dislocation of the femoral head.
A diagnosis of PJI with instability was established. The patient was managed with wound debridement and lavage, explantation of the hemiarthroplasty prosthesis, and placement of an antibiotic-impregnated cement spacer (Fig. 2) as the first stage of a two-stage revision.
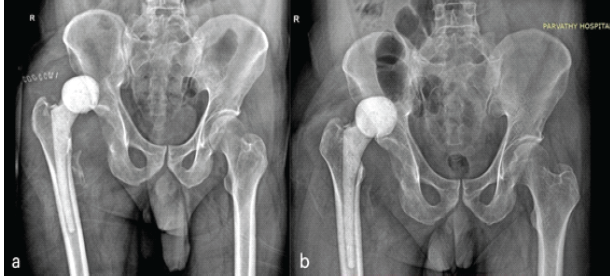
Figure 2: Anteroposterior radiograph of the pelvis showing dislocated antibiotic cement spacer (a) Five days and (b) Three months postoperatively.
The antibiotic-impregnated cement spacer had also dislocated on the 5th postoperative day. After an interval of 12 weeks on culture-directed intravenous antibiotics, with normalization of inflammatory markers and a negative aspiration, the patient underwent first-stage revision THA with a constrained acetabular liner construct (Fig. 3 and 4).
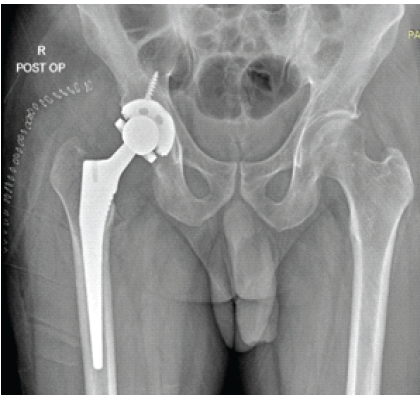
Figure 3: Post-operative anteroposterior radiograph of the pelvis demonstrating a right revision total hip arthroplasty with a cementless femoral stem and a constrained acetabular liner construct.
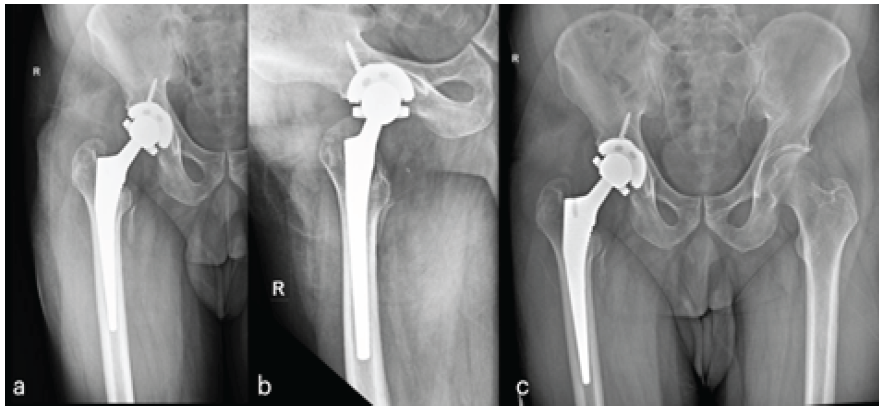
Figure 4: Post-operative radiograph of right hip following revision total hip arthroplasty with a constrained acetabular liner. (a and b) One month Anteroposterior and lateral, respectively, (c) two months anteroposterior view.
Given the significant soft-tissue compromise from the prior infection and multiple procedures, a constrained liner was selected to address anticipated intraoperative and post-operative instability. Unfortunately, the patient was poorly compliant with the prescribed post-operative hip precautions. He returned prematurely to ambulation and strenuous activities, including ground-level work, within 2 months of surgery and was on irregular follow-up. At 6 months following revision THA, he presented with dislocation, which was successfully managed with closed reduction (Fig. 5).
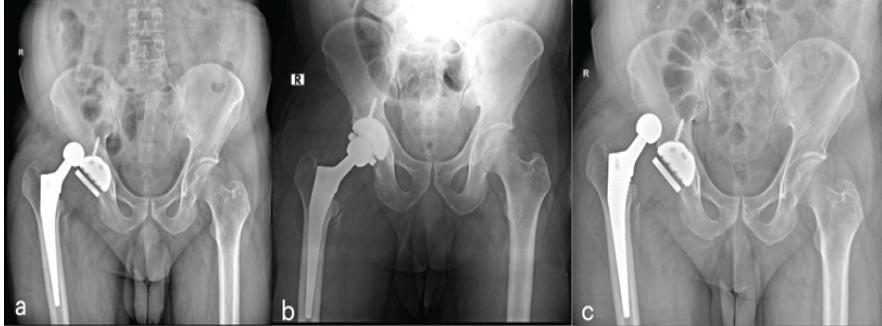
Figure 5: Anteroposterior pelvis radiograph showing (a) dissociation of the bipolar head from the constrained liner insert without ring disruption at 6 months postoperatively, (b) immediate post-closed reduction radiograph confirming satisfactory reduction of the femoral head within the constrained liner, (c) radiograph obtained 1 week following closed reduction demonstrating recurrent dislocation.
However, he resumed ambulation within 1 week of closed reduction and went on to develop a further dislocation. This sequence of events underscores the ongoing challenge of managing recurrent instability in the setting of compromised soft tissues, poor patient compliance, and a multiply-revised hip. Radiographic evaluation across the episodes demonstrated a recurring pattern of instability with the femoral head dislocating from the acetabular component (Fig. 3a and b). Hence, with persistent recurrent instability, the decision was made to proceed to a second revision THA. During the second revision, the acetabular component was found to be well-fixed (Fig. 6).
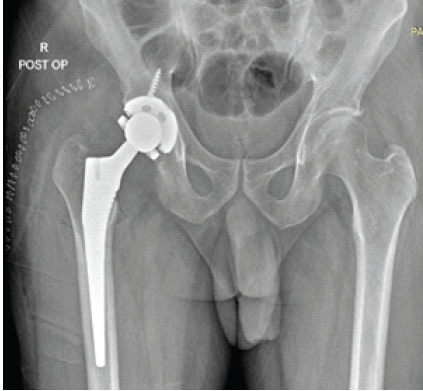
Figure 6: Post-operative anteroposterior radiograph of the pelvis demonstrating the second revision right total hip arthroplasty, with a cementless femoral stem and constrained acetabular liner construct.
The femoral stem was also well-fixed and retained. The polyethylene rim of the constrained liner insert was also found to be undeformed (Fig. 4). However, on intraoperative examination of the retrieved failed liner assembly, a previously unreported failure mode was identified; the failure interface was located at the factory-assembled junction between the constrained liner insert and the bipolar head. Subsequent management involved further counselling regarding activity restrictions, physiotherapy focused on hip abductor strengthening, and close surveillance. At routine clinic follow-up, the prosthesis was well-positioned, and the patient had achieved a satisfactory range of motion (Fig. 7). The patient was advised regarding permanent restriction from heavy manual labour.
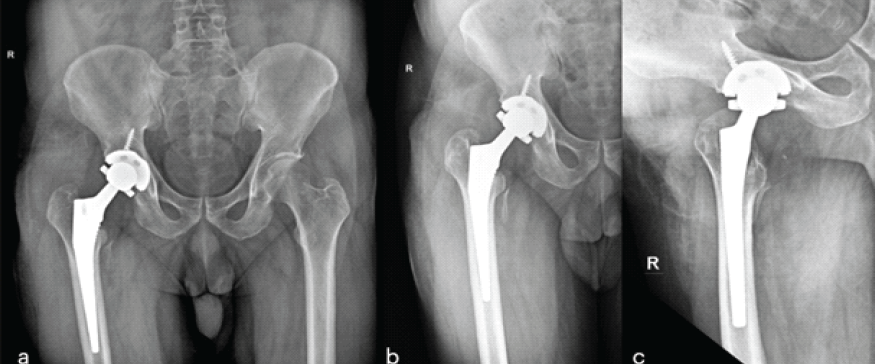
Figure 7: Post-operative radiographs following the second revision right total hip arthroplasty (a) Anteroposterior pelvic radiograph at 1 month, (b) anteroposterior and (c) lateral radiographs of the right hip at 1 year.
Constrained acetabular liners are a recognised salvage option for recurrent hip instability, particularly when soft-tissue reconstruction or component repositioning is not feasible or has already failed. However, their use comes with a well-defined risk of mechanical failure. Cooke et al. [5] described three failure modes in the Osteonics tripolar system: Type I (acetabular bone-prosthesis interface), Type II (liner-locking mechanism), and Type III (femoral head-locking mechanism), with a 13.8% reoperation rate at short-term follow-up. Yun et al. [4] expanded this classification to include four categories, identifying impingement as the principal underlying mechanism in each mode and emphasising that biomaterial failure manifests as fracture of the outer metal ring and deformation at the polyethylene liner’s apex, precisely the location of failure observed in our case.
The failure documented in this report is distinct in its anatomical localisation. While prior descriptions of Type III failure involve fracture or displacement of the locking ring [5], and while Yun et al. described biomaterial failure of the outer polyethylene rim [4], neither series reported failure specifically at the factory-assembled constrained liner insert-bipolar head junction without an associated locking ring fracture. This represents a fourth distinct failure interface, conceptually analogous to the intraprosthetic dislocation described in dual-mobility bearings, where dissociation occurs between components that are pre-assembled at manufacture rather than at the cement-liner or shell-liner interface [6].
Impingement remains the unifying mechanism. In our patient, the combination of multiply-revised soft tissues with compromised abductor function, a history of PJI, and poor compliance with post-operative restrictions created the biomechanical milieu for repetitive high-force impingement of the bipolar head against the constrained liner insert. The deformation observed at the polyethylene rim apex is consistent with fatigue failure driven by cyclic impingement loading, as described by Yun et al. [4]. Several lessons emerge from this case. First, patient compliance with postoperative restrictions is not merely a behavioural recommendation but a biomechanical imperative, particularly when constraining components are used in the context of multiply-revised hips. As demonstrated in our case, early return to strenuous activities effectively abolished the biological window for soft-tissue healing and impingement risk reduction. Second, the surgeon must be aware that failure interfaces in constrained systems may not conform to established classification schemes; a thorough intraoperative examination of retrieved components is essential to identify the specific failure mechanism, as management differs according to cause [7,8]. Third, the possibility of this novel failure interface should be considered when evaluating recurrent instability after constrained THA, particularly when radiographs do not clearly demonstrate locking ring fracture or cup loosening. The decision of whether to proceed to a constrained liner in the first place remains nuanced. In this patient, the combination of PJI sequelae, severely compromised soft tissues, abductor weakness, and intraoperative instability at the time of revision left few alternatives. As Berry [2] and Yun et al. [4] have emphasised, constrained liners should be reserved as a last resort, used only when all other correctable causes of instability have been addressed. In complex cases such as ours, supplementing the implant strategy with prolonged rehabilitation and meticulous follow-up is essential.
Registry-based data and systematic review evidence suggest that dual mobility implants demonstrate lower incidences of dislocation (3% versus 9%), re-revision for dislocation (2% vs. 9%), and re-revision for any cause (8% vs. 19%) when compared to constrained acetabular components [9]. With a dramatic increase in the head-to-neck ratio while reducing the risk of mechanical failure or excessive wear, dual mobility THA has been shown to outperform constrained liners at 10-year follow-up and continues to gain interest worldwide as the preferred option for managing instability [10]. In the present case, however, the use of a constrained liner was a pragmatic decision driven by the patient’s financial constraints, as dual mobility implants carry a significantly higher cost and were not accessible within the patient’s means.
This case documents a previously unreported failure interface in constrained THA, occurring at the factory-assembled constrained liner insert-bipolar head junction in the absence of locking ring fracture. The failure occurred in the context of multiply-revised THA following PJI, with contributing factors including impingement secondary to poor post-operative compliance. Revision arthroplasty surgeons should be aware of this failure mode when evaluating recurrent instability after constrained THA. The right surgery and right implant alone do not guarantee success; post-operative rehabilitation and patient compliance play equally pivotal roles in the long-term outcome.
When evaluating recurrent instability after constrained total hip arthroplasty, the failure interface between the constrained liner insert and the bipolar head, distinct from classic locking ring failure, should be considered. Intraoperative retrieval analysis is essential. Patient compliance with activity restrictions in the post-operative period is a critical determinant of implant longevity.
References
- 1. Fackler CD, Poss R. Dislocation in total hip arthroplasties. Clin Orthop 1980;151:169-78. [Google Scholar] [PubMed]
- 2. Berry DJ. Unstable total hip arthroplasty: Detailed overview. Instr Course Lect 2001;50:265-74. [Google Scholar] [PubMed]
- 3. Callaghan JJ, Heithoff BE, Goetz DD, Sullivan PM, Pedersen DR, Johnston RC. Prevention of dislocation after hip arthroplasty: Lessons from long-term followup. Clin Orthop Relat Res 2001;393:157-62. [Google Scholar] [PubMed]
- 4. Yun AG, Padgett D, Pellicci P, Dorr LD. Constrained acetabular liners: Mechanisms of failure. J Arthroplasty 2005;20:536-41. [Google Scholar] [PubMed]
- 5. Cooke CC, Hozack W, Lavernia C, Sharkey P, Shastri S, Rothman RH. Early failure mechanisms of constrained tripolar acetabular sockets used in revision total hip arthroplasty. J Arthroplasty 2003;18:827-33. [Google Scholar] [PubMed]
- 6. Ward JP, McCardel BR, Hallstrom BR. Complete dissociation of the polyethylene component in a newly available dual-mobility bearing used in total hip arthroplasty: A case report. JBJS Case Connect 2013;3:e94. [Google Scholar] [PubMed]
- 7. Lavigne MJ, Sanchez AA, Coutts RD. Recurrent dislocation after total hip arthroplasty: Treatment with an Achilles tendon allograft. J Arthroplasty 2001;16:13-8. [Google Scholar] [PubMed]
- 8. Kaplan SJ, Thomas WH, Poss R. Trochanteric advancement for recurrent dislocation after total hip arthroplasty. J Arthroplasty 1987;2:119-24. [Google Scholar] [PubMed]
- 9. Zogg CK, Falvey JR, Dimick JB, Haider AH, Davis KA, Grauer JN. Changes in discharge to rehabilitation: Potential unintended consequences of Medicare total hip arthroplasty/total knee arthroplasty bundled payments, should they be implemented on a nationwide scale? J Arthroplasty 2019;34:1058-65.e4. [Google Scholar] [PubMed]
- 10. Hoskins W, Bingham R, Hatton A, De Steiger RN. Standard, large-head, dual-mobility, or constrained-liner revision total hip arthroplasty for a diagnosis of dislocation: An analysis of 1,275 revision total hip replacements. J Bone Joint Surg Am 2020;102:2060-7. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bone Morphogenetic Proteins-2–Augmented Acetabular Bone Stock Restoration During Two-stage Revision for Periprosthetic Joint Infection: A Case Report
July 1, 2026 Bone Morphogenetic Proteins-2–Augmented Acetabular Bone Stock Restoration During Two-stage Revision for Periprosthetic Joint Infection: A Case Report July 1, 2026 Custom-Made Monoflange Acetabular Component for Revision Hip Arthroplasty in Paprosky Type IIIA Defect: A Case Report
July 1, 2026 Custom-Made Monoflange Acetabular Component for Revision Hip Arthroplasty in Paprosky Type IIIA Defect: A Case Report June 1, 2026 Antiphospholipid Syndrome–Associated Livedoid Vasculopathy Mimicking Recurrent Periprosthetic Joint Infection after Total Knee Arthroplasty: A Case Report
June 1, 2026 Antiphospholipid Syndrome–Associated Livedoid Vasculopathy Mimicking Recurrent Periprosthetic Joint Infection after Total Knee Arthroplasty: A Case Report June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report
June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report