
Establishing disease-specific MCID and PASS thresholds for commonly used shoulder PROMs improves interpretation of patient-reported outcomes in acromioclavicular joint arthropathy and supports standardized reporting in clinical research.
Dr. Abhay Tyagi, Department of Orthopaedics, Kalinga Institute of Medical Sciences, Bhubaneswar - 751024, Odisha, India. E-mail: abhay20tyagi@gmail.com
Abstract
Introduction: Minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) are essential for interpreting patient-reported outcome measures (PROMs). However, disease-specific thresholds for acromioclavicular (AC) joint arthropathy are not well established, limiting meaningful interpretation of patient-reported outcomes.
Materials and Methods: This prospective observational cohort study included adults with symptomatic AC joint arthropathy managed either conservatively or surgically. PROMs – including the Constant–Murley score, American Shoulder and Elbow Surgeons score, University of California Los Angeles score, Quick Disabilities of the Arm, Shoulder and Hand, Western Ontario Rotator Cuff (WORC) index, and visual analogue scale for pain – were collected at baseline and 12 months. MCID, substantial clinical benefit (SCB), and maximum outcome improvement (MOI) were determined using anchor-based methods with a global rating of change scale and receiver operating characteristic analysis, supported by distribution-based estimates. PASS thresholds were derived using a patient satisfaction anchor. Thresholds were calculated separately within surgical and conservative treatment contexts in accordance with Consensus-based Standards for the Selection of Health Measurement Instruments recommendations.
Results: A total of 170 patients (100 conservative, 70 surgical) completed a 12-month follow-up. All PROMs demonstrated excellent reliability (intraclass correlation coefficient range, 0.85–0.96) and strong anchor validity (Spearman r, 0.51–0.62; P < 0.001). Anchor-based MCID values differed across PROMs and treatment contexts but consistently exceeded measurement error. The WORC index demonstrated the highest responsiveness (area under the curve, 0.84; standardised response mean, 0.85). PASS thresholds reflected acceptable symptom states across PROMs, and approximately 92% of patients achieving MCID also met PASS criteria. Thresholds were derived independently within each treatment context and were not intended for comparative assessment of treatment effectiveness.
Conclusion: This study establishes disease-specific MCID, SCB, MOI, and PASS thresholds for commonly used shoulder PROMs in AC joint arthropathy. These benchmarks enhance the interpretability of patient-reported outcomes, support standardised reporting in clinical research, and should be applied as measurement tools rather than indicators of comparative treatment efficacy.
Keywords: Acromioclavicular joint arthropathy, minimal clinically important difference, patient acceptable symptom state, patient-reported outcome measures, shoulder outcome scores.
Acromioclavicular (AC) joint arthropathy is a common source of shoulder pain and functional limitation, particularly among individuals involved in overhead activities and manual labor. Degenerative changes of the AC joint may result in localized pain, discomfort during cross-body movements, and reduced health-related quality of life. Management options include conservative measures such as physiotherapy and injections, as well as surgical interventions like arthroscopic distal clavicle excision, depending on symptom severity and functional impairment [1,2].
Patient-reported outcome measures (PROMs) are widely used to quantify pain, function, and quality of life in patients with shoulder disorders. Commonly used instruments include the Constant–Murley score, American Shoulder and Elbow Surgeons (ASES) score, University of California Los Angeles (UCLA) score, quick disabilities of the arm, shoulder and hand (QuickDASH), Western Ontario Rotator Cuff (WORC) index, and the visual analog scale (VAS) for pain [3,4,5,6]. Although these tools are well validated, interpretation of numerical score changes remains challenging without clinically meaningful reference thresholds.
The minimal clinically important difference (MCID) is defined as the smallest change in an outcome measure perceived by patients as beneficial and serves to distinguish clinically meaningful improvement from measurement variability [7,8]. Beyond minimal improvement, additional concepts such as substantial clinical benefit (SCB) and maximum outcome improvement (MOI) capture higher levels of patient-perceived benefit, while the patient acceptable symptom state (PASS) reflects the threshold beyond which patients consider their symptoms satisfactory [9,10,11,12]. Together, these constructs provide a comprehensive framework for interpreting PROMs across the spectrum of patient-perceived outcomes.
Importantly, MCID, SCB, MOI, and PASS are context-dependent measurement properties, influenced by baseline symptom severity, patient expectations, and treatment setting rather than being fixed characteristics of a PROM [13,14,15]. Consequently, disease-specific and context-specific thresholds are recommended to ensure accurate interpretation of patient-reported outcomes. While such thresholds have been established for several shoulder conditions, including rotator cuff disease and shoulder arthroplasty [16,17,18], corresponding benchmarks for AC joint arthropathy remain limited.
The absence of validated, disease-specific MCID, SCB, MOI, and PASS thresholds for AC joint arthropathy restricts meaningful interpretation of PROM-based outcomes in both clinical practice and research. Establishing these thresholds would enhance standardized outcome reporting and facilitate appropriate interpretation of treatment response without implying comparative effectiveness between management strategies.
Therefore, the purpose of this prospective cohort study was to establish disease-specific MCID, SCB, MOI, and PASS thresholds for commonly used shoulder PROMs in patients with symptomatic AC joint arthropathy, using anchor-based and distribution-based methods consistent with Consensus-based Standards for the Selection of Health Measurement Instrument (COSMIN) recommendations.
Study design and ethics
This prospective observational cohort study was conducted at a tertiary-care orthopedic center between January 2022 and December 2024. Approval of the Institutional Ethics Committee of KIMS, KIIT University, was obtained before study initiation (Ref: KIIT/KIMS/IEC/1017/2021), and written informed consent was secured from all participants. The study was conducted in accordance with the Declaration of Helsinki. Methodological design, analysis, and reporting were aligned with the COSMIN guidelines for studies evaluating measurement properties of PROMs.
Patient selection and diagnostic criteria
Adult patients (≥18 years) presenting with symptomatic AC joint arthropathy were screened for eligibility. Diagnosis was established using a combination of:
- Localized tenderness over the AC joint on clinical examination
- Pain reproduced with cross-body adduction testing
- Radiographic evidence of AC joint degeneration on Zanca-view radiographs.
Patients were eligible if symptoms persisted for a minimum of 3 months despite initial activity modification.
Exclusion criteria
Patients were excluded if they had:
- Prior AC joint surgery or intra-articular injection
- Acute traumatic AC joint injury
- Full-thickness rotator cuff tear on imaging
- Inflammatory arthritis, infection, or neurological disorders affecting the upper limb
- Cognitive impairment precluding reliable PROM completion.
Treatment allocation
Treatment modality was determined through shared decision-making between the patient and the treating surgeon, based on symptom severity, functional limitation, and patient preference.
Conservative management
Conservative treatment consisted of:
- Structured physiotherapy emphasizing scapular stabilization and rotator cuff strengthening (twice weekly for 6 weeks, followed by a home program)
- Oral non-steroidal anti-inflammatory drugs as required
- Optional ultrasound-guided AC joint corticosteroid injection for persistent symptoms.
Surgical management
Surgical treatment involved arthroscopic distal clavicle excision, performed using a standardized technique with resection of approximately 8–10 mm of the distal clavicle while preserving the superior capsule. All patients followed a standardized post-operative rehabilitation protocol focusing on early range of motion followed by progressive strengthening.
Outcome measures
PROMs were collected at baseline and at 12 months and included:
- Constant–Murley score
- ASES score
- UCLA score
- QuickDASH
- WORC index
- VAS for pain.
Higher scores indicate better outcomes for constant, ASES, UCLA, and WORC, whereas lower scores indicate improvement for QuickDASH and VAS. All change scores were oriented such that positive values represented clinical improvement.
Anchor selection and validation
A global rating of change (GRC) scale was used as the external anchor for anchor-based analyses. At 12 months, patients responded to the question:
“Compared with your condition before treatment, how would you describe your shoulder now?”
Responses were recorded on a 7-point Likert scale ranging from very much worse (−3) to very much improved (+3). Clinically important improvement was defined a priori as GRC ≥ +2, consistent with published MCID methodology.
Anchor validity was confirmed by:
- Moderate to strong correlations (Spearman r ≥ 0.50) between GRC scores and PROM change scores
- A monotonic increase in PROM improvement across ascending GRC categories.
Reliability and measurement error
Internal consistency was assessed using Cronbach’s alpha (α ≥ 0.80 considered acceptable). Test–retest reliability was evaluated using intraclass correlation coefficients (ICC, two-way random effects model), with ICC ≥ 0.75 indicating excellent reliability. Measurement error was quantified using the standard error of measurement (SEM) and minimal detectable change at the 95% confidence level (MDC95).
Determination of MCID, SCB, and MOI
Anchor-based methods
- MCID was defined as the PROM change corresponding to GRC ≥ +2
- SCB corresponded to GRC ≥ +3
- MOI was defined as the PROM change associated with the highest GRC category.
Receiver operating characteristic (ROC) curve analysis was performed, and optimal thresholds were determined using the Youden index.
Distribution-based methods
Distribution-based estimates included SEM, MDC95, and 0.5 × standard deviation. MCID values were considered valid only if they exceeded MDC95, ensuring changes were greater than measurement error.
PASS determination
PASS was determined at 12 months using a dichotomous satisfaction anchor based on the question:
“Considering your daily activities, pain, and functional limitations, do you consider your current shoulder condition satisfactory?” (yes/no)
ROC analysis was used to derive PROM-specific PASS cut-off values.
Subgroup-specific analysis
To account for differences in baseline severity, patient expectations, and achievable improvement, MCID, SCB, MOI, and PASS thresholds were derived separately for surgically and conservatively managed patients. Thresholds were calculated independently within each subgroup and were not statistically compared between treatment groups.
Sample size considerations
Although no a priori sample size calculation was performed, the final cohort size was considered adequate for anchor-based MCID estimation based on methodological recommendations suggesting a minimum of 50 patients per subgroup for reliable ROC-based threshold derivation. Both treatment cohorts exceeded this threshold.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation or median (interquartile range). ROC performance was assessed using area under the curve (AUC), and responsiveness was quantified using standardized response means (SRM). AUC values ≥0.80 were considered excellent. Statistical analyses were performed using Statistical Package for the Social Sciences version 26 (IBM Corp., Armonk, NY), with P < 0.05 considered statistically significant.
Patient flow and baseline characteristics
A total of 196 patients were screened for eligibility. Twenty-six patients were excluded due to rotator cuff tears, prior AC joint injection, inflammatory arthritis, or refusal to participate. One hundred seventy patients were included and completed 12-month follow-up, comprising 100 conservatively managed and 70 surgically treated patients (Fig. 1 and Table 1).
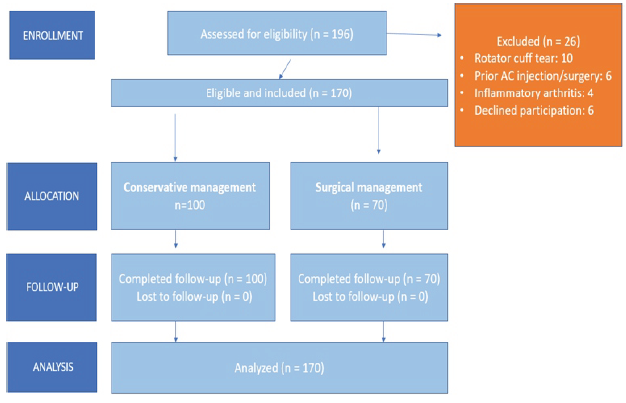
Figure 1: Patient flow diagram of study enrollment, treatment allocation, and follow-up.
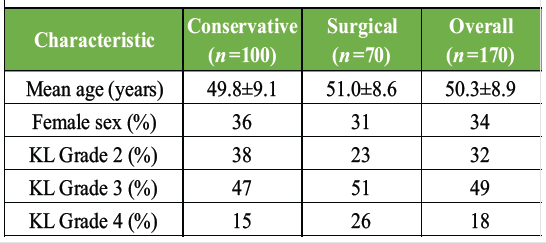
Table 1: Baseline characteristics
Reliability and anchor validity
All PROMs demonstrated excellent internal consistency and reliability (Cronbach α >0.80; ICC range 0.85–0.96). Correlations between GRC scores and PROM change scores ranged from 0.51 to 0.62 (P < 0.001), confirming anchor validity and appropriate responsiveness to perceived clinical change (Fig. 2a).
MCID, SCB, and MOI thresholds
Anchor-based MCID, SCB, and MOI thresholds differed by treatment context and are summarized below (Table 2 and Fig. 2b).
Distribution-based estimates supported anchor-based thresholds, with all MCID values exceeding MDC95 (Fig. 2c).
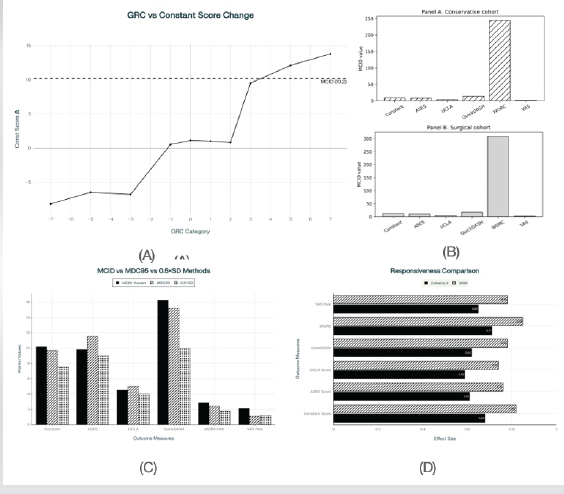
Figure 2: (a) Relationship between global rating of change and patient-reported outcome measures (PROM) change scores. (b) Anchor-based minimal clinically important difference (MCID) thresholds derived separately for surgical and conservative cohorts using multiple analytical methods. (c) Comparison of MCID with measurement error estimates across PROMs (subgroup-specific analysis). (d) Responsiveness of patient-reported outcome measures in acromioclavicular joint arthropathy.
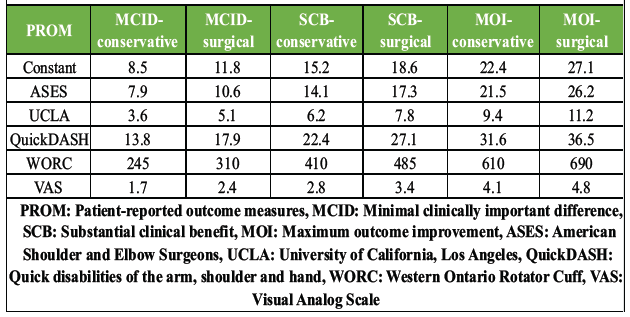
Table 2: Anchor-based MCID, SCB, and MOI by treatment context
PASS Thresholds (Table 3).
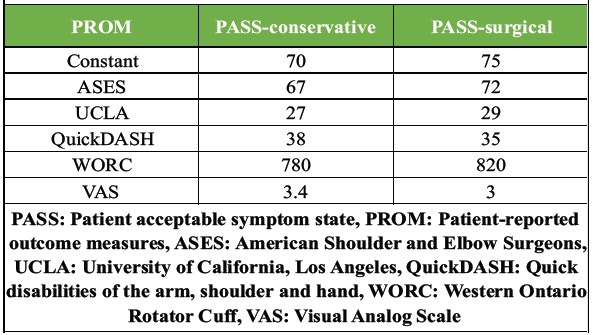
Table 3: PASS cut-off values by treatment context
Achievement of MCID and PASS
Across PROMs, 46–51% of patients achieved MCID at 12 months. Among patients who achieved MCID, approximately 92% also met PASS criteria, supporting the clinical relevance of the derived thresholds. The proportion of patients achieving MCID and higher benefit levels varied by treatment context, reflecting differences in baseline severity and achievable improvement rather than comparative treatment effectiveness.
Responsiveness
The WORC index demonstrated the highest responsiveness (AUC 0.84; SRM 0.85), followed by Constant and ASES scores. QuickDASH and VAS demonstrated moderate responsiveness (Table 4 and Fig. 2d).
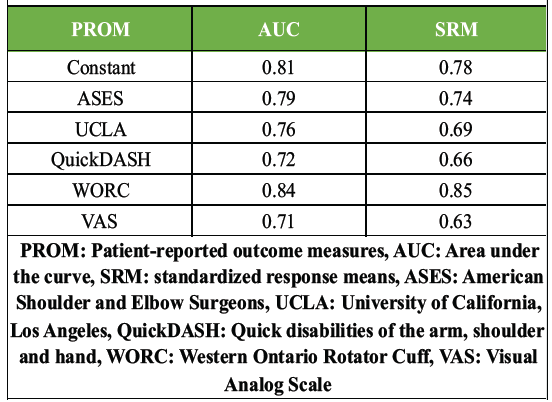
Table 4: Responsiveness indices
The principal finding of this study is the establishment of disease-specific MCID, SCB, MOI, and PASS thresholds for six commonly used PROMs in patients with symptomatic AC joint arthropathy. Using a prospective design and COSMIN-aligned methodology, the derived thresholds provide clinically meaningful benchmarks for interpreting patient-reported outcomes in this condition.
Across all PROMs, anchor-based thresholds were supported by strong anchor validity, excellent reliability, and concordant distribution-based estimates, confirming that the identified MCID values exceeded measurement error and represented meaningful clinical change. These findings reinforce the methodological robustness of the derived thresholds and support their use in outcome interpretation rather than treatment comparison [13,14].
The WORC index demonstrated the highest responsiveness among evaluated PROMs, as reflected by superior SRMs and area under the ROC curve. This finding is consistent with prior literature demonstrating the sensitivity of the WORC index to changes in shoulder-specific pathology and patient-perceived improvement [6,19]. The strong responsiveness of the WORC index suggests that it may be particularly suitable for longitudinal assessment in AC joint arthropathy, although responsiveness alone does not imply superiority of any treatment modality.
MCID, SCB, MOI, and PASS thresholds were derived separately within surgical and conservatively managed cohorts to account for differences in baseline severity, expectations, and achievable improvement. This subgroup-specific approach aligns with contemporary recommendations emphasizing that clinically meaningful change thresholds are context-dependent and should not be assumed to be universal across treatment settings [13,15]. Importantly, thresholds were derived independently and were not statistically compared between groups, as the study was not designed to evaluate comparative treatment effectiveness.
A substantial proportion of patients who achieved MCID also met PASS criteria, supporting the conceptual relationship between meaningful improvement and attainment of an acceptable symptom state. Similar associations have been reported across musculoskeletal conditions and reinforce the clinical relevance of these metrics when used appropriately for outcome interpretation [10,11,12,20,21 ]. However, variation in the proportion of patients achieving these thresholds across treatment contexts should be interpreted descriptively and within the limits of the study design.
The strengths of this study include its prospective design, complete follow-up, use of multiple validated PROMs, and rigorous application of both anchor-based and distribution-based methods in accordance with COSMIN guidelines. The inclusion of SCB and MOI further extends the interpretive framework beyond minimal improvement, offering a more comprehensive understanding of patient-perceived benefit.
These thresholds define patient-perceived meaningful change and acceptable symptom states and are not intended to compare the effectiveness of surgical and conservative management.
Several limitations merit consideration. The study was conducted at a single center, which may limit generalizability. Diagnostic confirmation relied on clinical and radiographic criteria without routine diagnostic injections. In addition, although treatment-specific thresholds were derived, the observational design precludes causal inference or comparison of treatment effectiveness. External validation in independent cohorts will be important to confirm the applicability of these thresholds across diverse populations. Lack of subgroup analysis based on baseline characteristics may limit the assessment of outcome variability across different patient groups.
This study provides validated, disease-specific MCID, SCB, MOI, and PASS thresholds for commonly used shoulder PROMs in AC joint arthropathy. These thresholds enhance the interpretability of patient-reported outcomes, support standardized reporting in clinical research, and should be applied as measurement tools rather than indicators of comparative treatment efficacy.
Disease-specific MCID and PASS thresholds provide clinically meaningful benchmarks for interpreting shoulder PROMs in AC joint arthropathy and should be used to guide outcome interpretation rather than to compare treatment effectiveness.
References
- 1. Beitzel K, Mazzocca AD, Cote MP, Apostolakos J, Solovyova O, Imhoff AB, et al. Current concepts in the treatment of acromioclavicular joint dislocations. Arthroscopy 2013;29:387-97. [Google Scholar] [PubMed]
- 2. Ben H, Wang Y, Liu J, Chen X, Zhang L, Zhao Y, et al. Relationship between achieving minimal clinically important difference and patient-reported satisfaction after orthopaedic surgery. J Orthop Surg 2025;30:123-9. [Google Scholar] [PubMed]
- 3. Brozek JL, Guyatt GH, Schünemann HJ. How a well-grounded minimal important difference can enhance transparency of patient-reported outcomes. J Clin Epidemiol 2006;59:1046-52. [Google Scholar] [PubMed]
- 4. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 1987;214:160-4. [Google Scholar] [PubMed]
- 5. Copay AG, Subach BR, Glassman SD, Polly DW Jr., Schuler TC. Understanding the minimum clinically important difference: A review of concepts and methods. Spine J 2007;7:541-6. [Google Scholar] [PubMed]
- 6. Dabbagh A, Ebrahimzadeh MH, Moradi A, Kachooei AR, Hallaj-Moghaddam M, Tabrizi A, et al. Determining the minimal clinically important difference for shoulder outcome scores after rotator cuff repair. J Orthop Res 2025;43:851-7. [Google Scholar] [PubMed]
- 7. Dawson J, Hill G, Fitzpatrick R, Carr A. The benefits of using patient-based methods of assessment. J Bone Joint Surg Br 2001;83:418-26. [Google Scholar] [PubMed]
- 8. Flatow EL, Duralde XA. The acromioclavicular joint: Anatomy, function, and pathology. J Bone Joint Surg Am 1990;72:704-11. [Google Scholar] [PubMed]
- 9. Gagnier JJ, Robbins C, Bedi A, Carpenter JE, Miller BS. Establishing patient acceptable symptom state thresholds for shoulder conditions: A systematic review. J Shoulder Elbow Surg 2024;33:12-23. [Google Scholar] [PubMed]
- 10. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand) [corrected]. The upper extremity collaborative group (UECG) Am J Ind Med 1996;29:602-8. [Google Scholar] [PubMed]
- 11. Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials 1989;10:407-15. [Google Scholar] [PubMed]
- 12. Kirkley A, Griffin S, McLintock H, Ng L. The development and evaluation of a disease-specific quality of life measurement tool for shoulder instability. Am J Sports Med 1998;26:764-72. [Google Scholar] [PubMed]
- 13. Michener LA, McClure PW, Sennett BJ. American shoulder and elbow surgeons standardized shoulder assessment form, patient self-report section: Reliability, validity, and responsiveness. J Shoulder Elbow Surg 2002;11:587-94. [Google Scholar] [PubMed]
- 14. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments. Qual Life Res 2010;19:539-49. [Google Scholar] [PubMed]
- 15. Roy JS, MacDermid JC, Woodhouse LJ. Measuring shoulder function: A systematic review of outcome measures. Shoulder Elbow 2009;1:89-99. [Google Scholar] [PubMed]
- 16. Snyder SJ, Banas MP. Arthroscopic treatment of acromioclavicular joint disease. Orthop Clin North Am 2003;34:567-75. [Google Scholar] [PubMed]
- 17. Tashjian RZ, Deloach J, Porucznik CA, Powell AP. Determining the minimal clinically important difference for the American shoulder and elbow surgeons score after shoulder arthroplasty. J Bone Joint Surg Am 2016;98:163-71. [Google Scholar] [PubMed]
- 18. Terwee CB, Prinsen CA, Chiarotto A, Westerman MJ, Patrick DL, Alonso J, et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures. Qual Life Res 2018;27:1159-70. [Google Scholar] [PubMed]
- 19. Tubach F, Ravaud P, Baron G, Falissard B, Logeart I, Bellamy N, et al. Evaluation of clinically relevant states in patient reported outcomes in knee and hip osteoarthritis: The patient acceptable symptom state. Ann Rheum Dis 2005;64:34-7. [Google Scholar] [PubMed]
- 20. Wright RW, Baumgarten KM, Dunn WR, Spindler KP. Predictors of patient satisfaction after rotator cuff repair. J Bone Joint Surg Am 2013;95:1993-9. [Google Scholar] [PubMed]
- 21. Yendluri A, Somerson JS, Hsu JE, Gee AO, Matsen FA, Wagner ER, et al. Establishing minimal clinically important difference values for patient-reported outcomes following reverse total shoulder arthroplasty. Clin Orthop Relat Res 2025;483:145-56. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2020 Management of Neglected Odontoid Fracture in the Ankylosed Spine: A Case Report and Technical Note
August 10, 2020 Management of Neglected Odontoid Fracture in the Ankylosed Spine: A Case Report and Technical Note January 10, 2024 A Rare Case of Grisel’s Syndrome in A 6-Year-Old Child
January 10, 2024 A Rare Case of Grisel’s Syndrome in A 6-Year-Old Child February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report
February 1, 2026 Fungal Infection of Native Hip Joint Presenting as Secondary Arthritis in 52-Year-Old Male – A Rare Case Report March 1, 2026 Vascularized fibular flap for gunshot-induced composite foot defects: Two-case report and comprehensive literature review
March 1, 2026 Vascularized fibular flap for gunshot-induced composite foot defects: Two-case report and comprehensive literature review