
Head-split proximal humerus fractures are rare and often missed. Computed tomography scans with a dedicated classification system, Schiebel’s, help the surgeon plan appropriate management of such fractures.
Dr. Kaustav Mukherjee, Department of Orthopaedics, Santiniketan Medical College and Hospital, Bolpur, West Bengal, India. E-mail: kaustavm.1992@gmail.com
Abstract
Purpose: Humerus head-split fractures are a rare subgroup of proximal humerus fractures that are challenging to treat. Being a coronal plane fracture, they are often missed on standard shoulder radiographs. We aim to bring forward the difficulties in identifying the isolated head split fractures, modes of internal fixation, possible complications of missing the head-split component in a complex proximal humerus fracture fixation, and the outcomes on the functionality of the shoulder joint.
Materials and Methods: A retrospective case–control study with all fractures treated by internal fixation was carried out at our institution. Shoulder axial computed tomography (CT) based Schiebel’s classification, Type 1 (head-split with posterior subluxation), Type 2 (head-split with anterior subluxation), and Type 3 (head-split with impaction), was utilized to grade the fractures. Fixation included two groups: cancellous screws alone and a plate-augmented-screw construct. The control group included cases where head splits were not addressed appropriately. Functional and radiological analyses were done at regular follow-up visits.
Results: A total of 24 patients were included in the study, 9 fixed by screws alone and 15 by plate-augmented-screw construct. The mean age of the study group was 34.5 years, with 85% male patients. Bony union was achieved in all cases, with the average time to union being 29 weeks. The study group recorded a mean Oxford shoulder score of 49 ± 2.45, contrary to the control group with a mean score of 22 ± 4.32 (P < 0.05).
Conclusion: Simple head splits are easily missed on standard shoulder radiographs and need additional imaging/views for diagnosis. Schiebel Type 1 and 2 fractures recorded excellent functional outcomes when addressed appropriately.
Keywords: Head split, humerus, internal fixation, young.
Humerus head split fractures represent a subgroup of proximal humerus fractures, which are seldom seen in young patients [1]. This fracture pattern, which is rarely encountered, represents a serious treatment challenge because of involvement and occasionally the comminution of the articular surface [2]. Head split usually occurs in high-velocity injuries, when the articular surface of the humeral head cleaves into two or more parts as it impacts against the glenoid, with or without dislocation [3]. Treatment for proximal humerus fractures ranges from non-operative treatment to various surgical options; however, head split fractures often represent an indication for surgical intervention [4]. In a complex proximal humerus fracture, where a head-split component is in associated with a humerus neck/tuberosity fractures, the treating surgeon often tend to miss this important component in fixation. This often leads to suboptimal results even after excellent fixation of extra-articular proximal humerus fracture components. In general, a clear definition and a treatment algorithm for head split fractures are lacking to date, with most surgeons preferring internal fixation for young patients [5]. This is largely due to the fact that the conventional proximal humerus fracture classifications do not address these components, which we need in decision-making while fixing these fractures.
We discussed a few cases over the last 10 years that were treated by internal fixation for humerus head split fractures. We have used two methods of internal fixation – one using cancellous screws alone and the other using a combination of locking plate with antero-posterior (AP) screws. We aim to bring forward the challenges in identifying these fractures, the necessity for higher imaging, principles of treatment, and the possible complications associated with this relatively rare pattern of fracture. We hypothesize that Schiebel’s classification can be an effective guide while treating these fractures, with the results of internal fixation in simple head split fractures being excellent.
All patients who were admitted to our institution with proximal humerus head split fractures from 2010 to 2020 were retrospectively followed up. Patients with proximal humerus fractures – head splits alone and complex proximal humerus fractures (head split + extra articular proximal humerus fracture) in the age group of 20–50 years were included in the study. Patients with pathological fractures and severe comminution were excluded. The control group included patients (age group 20–50 years), where the head split components were inadvertently missed (Table 1). A similar demographic distribution and identical injury severity were taken into account while selecting the control. Two sub-groups of patients (in the study group) were analyzed, with one group treated with cancellous screw fixation alone and the other operated by screws with augmented plate construct. This decision was solely based on the surgeon’s preference (upper limb surgeon with more than 10 years of experience) on the operating table as a means to achieve a sturdy fixation. Patients with axial CT scans showing isolated head splits underwent screw fixation alone, while head splits with a concomitant proximal humerus fracture were dealt with a plate-screw construct. X-rays and relevant higher imaging (CT/magnetic resonance imaging) were necessary for patients to be included in the study. All head split fractures were classified as per Schiebel’s classification (Fig. 1) retrospectively.
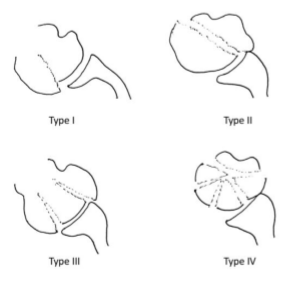
Figure 1: Schematic diagram of proximal humerus head split fractures classification as proposed by Scheibel et al.
Only Types 1, 2, and 3 Schiebel were included in the study group. This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the ethics committee of our university (IEC- SMCH/EC/2024–19, Approval date- November 12, 2024). Appropriate informed consent was taken from all the patients before their inclusion in our study.
A standard delto-pectoral approach allowed us to establish the rotator interval to identify the long head of the biceps tendon. Capsulotomy was done, the long head of the biceps tendon was mobilized and tenodesed to the pectoralis major, and the humeral head was exposed. The rotator cuff space approach was utilized, and humeral head retractors were put in place. Subluxed heads with fracture fragments were identified, reduced under fluoroscopy, and a temporary reduction was done with Kirschner wires. Definitive fixation was followed with screws (partially threaded hollow compression screws 4 mm) and, in cases augmented by a proximal humerus locking plate (AP screws were 3.5 mm cortical screws). Routine closures with absorbable sutures were done. Postoperatively, patients were mobilized, and rehabilitation was started from post-operative day 2 as tolerated, and the standard rehabilitation protocol was taught before discharge. Patients were followed up over the next 12 months with visits at regular intervals.
Radiological follow-up was done with X-rays – AP and lateral views, taken every 3rd month for the entire follow-up period. Radiological union of the fracture site was assessed on post-operative X-rays by two independent orthopedic surgeons, not involved in the study. The average of the two analyzers was taken to assess the mean time to radiological union. Union of the fracture site was also evaluated by the principal investigator on shoulder X-rays and inter/intra-observer reliability was tested. Clinical outcomes were recorded at the end of the follow-up period in all patients using the Oxford Shoulder score [6] and Visual Analog Scale (VAS), ranging from 0 (worst pain) to 10 (completely pain free). Active physiotherapy was taught and encouraged for all operated patients, and their compliance with the rehabilitation protocol was also closely monitored at each visit.
Statistical analysis was done using the Statistical Package for the Social Sciences software 25.0 (IBM Corp., Armonk, USA). Chi-square and Kruskal–Wallis tests were used to evaluate the variables to determine the significance of the fracture pattern and modes of internal fixation on the outcomes of the head split fractures. A multivariate analysis was performed to identify the parameters associated with good clinical and functional outcomes in these fractures. A value of P < 0.05 was considered significant.
Out of 39 patients presenting to us over the span of 10 years with proximal humerus head split fractures, 26 patients met the inclusion criteria, and two patients were lost to follow-up and were excluded from the study. In the final study group of 24 patients, the majority were male (85%). The mean age of the study group was 34.5 years ± 1.25. A total of 9 patients underwent fixation of the fracture by cancellous screws alone, and 15 patients were treated with a plate-augmented screw construct. The mean time from injury to operation in the first group was 3.8 days, whereas in the second group, it was 2.3 days. The mean physiotherapy duration in the first group was 36.4 weeks, whereas the other group recorded a mean duration of 44.7 weeks (Table 2). The control group included a total of ten patients, of whom three cases went into avascular necrosis (AVN) of the humerus head, two cases with non-union, and one case of stiff shoulder.
The radiological outcome was assessed by the mean time to bony union, which was 28.5 weeks in the screw group and 29.3 weeks in the plate-screw construct group. Functional outcome assessment for the study group recorded Oxford shoulder scores of 51.6 and 42.9 in the two sub-groups, respectively (P < 0.05). Mean VAS score in the screw group was 9.2, whereas in the plate-screw group it was 8.7 (P < 0.05). The mean Oxford shoulder score for the control group was recorded at 22.4 ± 4.32 (P < 0.05), with respect to a score of 48.6 ± 2.45 in the study group.
Proximal humerus fractures are common in the elderly but less common in young adults [7]. Head split fractures of the humerus with subluxation or dislocation may occur in young people but are rare and difficult to treat [8]. Initial X-rays of the shoulder may be misleading as the fracture tends to be missed in a standard AP view. Y view and axillary view X-rays are recommended for better visualization of the humeral head with respect to the glenoid; however, the severe pain might hinder us from taking these views at initial presentation [5]. Head split fractures can be identified by a double contour shadow and often by a “pelican” sign, which can be identified on radiographs but requires years of experience [9]. The diagnosis of this inconspicuous fracture pattern on a normal radiograph is quite difficult and needs higher imaging, such as CT, for accurate diagnosis. Resch et al. suggested CT scans for all complex proximal humerus fractures, which allows better evaluation of head-shaft relationship, tuberosity displacement, degree of comminution, and glenoid articular surface involvement [2]. However, the diagnosis of head split fractures is poor even in the presence of CT scans, with Greiwe et al. stating that only 37.5% of head splits were identified on normal radiographs and 50% on CT [9]. A missed diagnosis of head split fractures can lead to severe complications [5], with Chesser et al. documenting three cases of missed diagnosis where the patients developed bony ankylosis and shoulder stiffness [8]. We also need to consider the fact that the limited availability of higher imaging in rural setups and the lack of surgeon awareness increase the chances of missing these fractures. Our study had eight patients who had a missed diagnosis of head split fractures, and were referred to us from other centers, as the standard AP shoulder X-rays (Fig. 2) were inconclusive with the clinical findings in the patient (pain, inability to lift the arm).
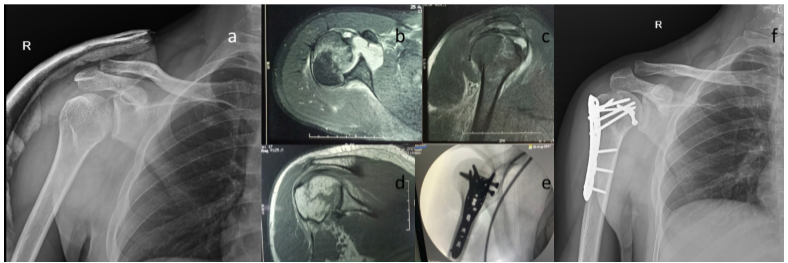
Figure 2: A 28-year-old male presented to the outpatient department, referred from an outside hospital with a history of trauma 2 days back. The patient presented with a magnetic resonance imaging (MRI) scan done, as initial X-rays were stated to be normal at the outside hospital (case of missed proximal humerus head split fracture). (a) X-ray antero-posterior view of right shoulder, (b) MRI scan – axial view showing a head split fracture with posterior subluxation of the shoulder joint (Schiebel Type 1), (c and d) showing the sagittal and coronal cut sections, respectively, (e) Intraoperative fluoroscopy pictures showing fixation of the fracture by plate-screw construct, (f) Post-operative X-ray 4 weeks post-fixation.
Although AO has classified head split as 11C2-3, any named classification lacks to date [5]. Hertel et al. proposed a classification based on Codman’s drawing [10]. Guix et al. made another description on proximal humerus later in 2009 [11]. However, these classifications were based on plain radiographs and were inconsistent with intraoperative findings. Gavaskar et al. highlighted Edelson’s CT-based classification that had higher interobserver reliability [12]. Schiebel et al. proposed the first CT-based classification exclusively for head split fractures and identified four distinct patterns [5]. Our case series has utilized this classification retrospectively, where axial shoulder cuts were utilized to grade these fractures. This classification system has made identifying the various fracture subtypes easier (Table 3). Our study group recorded a mean shoulder score of 51.8 ± 0.56 for Schiebel Type 1 and 2 fractures in comparison to a mean score of 40.8 ± 0.87 for Schiebel Type 3 fractures (P < 0.01). This provided valuable information regarding better outcomes of internal fixation in simple head splits fractures (Schiebel Types 1 and 2).
A classification not only helps to plan the management but also predicts the most dreaded complication of head split-head ischemia or AVN of the head. Gavaskar and Tummala mentioned a complex fracture pattern, presence of anterior dislocation, and choice of surgical approach (delto-pectoral approach), all associated with a higher incidence of AVN [12]. Ogawa et al. reported head split fractures with a posterior fracture dislocation, which maintained a good intact infero-medial attachment in 90% cases and had a low risk of AVN [13]. An excellent study by Robinson et al. predicted AVN risks and subclassified these injuries into two groups – Type I was defined as a humeral head that retained its capsular attachment, >2 cm in length, and had arterial bleeding. In contrast, Type II injuries were characterized by the head being significantly detached from capsular attachment, being <2 cm in length, and having no demonstrable arterial bleed [14]. Hertel et al. also emphasized the importance of the postero-medial bone spike attached to the humeral head as a favorable predictor of perfusion of the humeral head [10]. Our cases had an extra-articular postero-medial bone spike in 18 patients and could be classified as Robinson Type I, which can be associated with a good prognosis.
Given a wide option for treatment of head split fractures, ranging from conservative management for undisplaced fractures to shoulder arthroplasty in grossly comminuted fractures, choosing the ideal management is still a point of debate. Non-displaced or minimally displaced fractures can be treated conservatively in a brace or sling immobilization for 4 weeks [5]. This makes non-operative management apt for older patients with low functional demands, but operative fixation becomes a necessity in younger age groups, keeping in mind the complications arising from immobilizing a joint for longer periods. In younger patients, head-preserving methods of treatment are more appropriate [15]. The use of minimal fixation techniques with careful soft-tissue handling has significantly reduced the chances of AVN in head-preserving surgeries [1]. Furthermore, rich vascular supply to the humeral head and its excellent healing potential by revascularization after stable internal fixation have been mentioned by Schai et al. [16], Swamy and Schemitsch [17]. Open anatomic reduction and internal fixation should be considered the first line of treatment in all patients younger than 50 years, as hemiarthroplasty at such an early age has revealed poor results [15]. Chesser et al. described good results with internal fixation using one or two cancellous screws alone in simple head split fractures with complete bony union in all three cases, with patients ranging from the age of 19 to 41 years [8]. Another option for joint preservation treatment for this fracture pattern is open reduction and internal fixation (ORIF) using a locked plate with additional AP screws to stabilize the head-split, as mentioned by Gavaskar and Tummala [12]. Out of the 15 patients in their study (under the age of 55 years), bony union was achieved in 13 with no osteonecrosis or non-union. We followed a similar fixation principle, with 9 patients undergoing minimal internal fixation with screws alone (Fig. 3) and 15 patients being managed by a plate-screw construct.
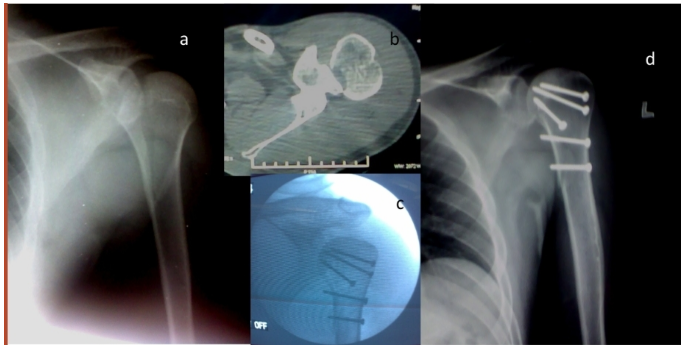
Figure 3: A 38-year-old male sustained closed injury to left shoulder and presented to us with (a) X-ray antero-posterior view of left shoulder, (b) computed tomography was done as no clear pattern was visualized on the X-rays and axial cuts revealed a head split (Schiebel Type 1), (c) Intra-operative fluoroscopy image showing fixation with screws alone through a standard delto-pectoral approach, (d) Post-operative X-ray at 18 weeks with good bony union and recorded excellent functional outcome.
Oxford shoulder score for the screws alone group was significantly better than the plate-screw construct group (P < 0.05), with 3 patients (from plate-screw construct group) complaining of hardware irritation on overhead abduction and demanding implant removal at 1 year follow-up (Fig. 4).
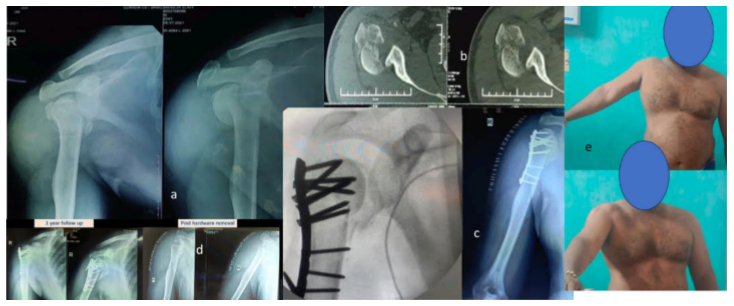
Figure 4: A 35-year-old male presented with a proximal humerus fracture, computed tomography scans, 3D reconstruction (a), and sagittal views (b) showing a comminuted fracture of the proximal humerus. However, the head split component was missed, as evident in axial views (Schiebel Type 3) (c) fracture was stabilized using a PHILOS plate, along with intraoperative C-arm showing inadequate reduction of the head component, (d) the patient presented to us at regular intervals with complaints of pain and inability to lift the shoulder, and eventually required hardware removal, (e) functional outcome at 1 year recorded poor shoulder scores.
Duration of physiotherapy and rehabilitation (required by the patients to regain near normal shoulder movements) in the screws alone group was 36.4 weeks, which was shorter than 44.7 weeks in the plate screws construct group (P = 0.232).
In our study, we had 17 cases of Schiebel Type 1 and 8 cases each from Schiebel Type 2 and 3. Chesser et al. stated a favorable prognosis post-internal fixation for posterior fracture subluxation/dislocation rather than anterior fracture dislocation of the humerus head split fractures [8]. An extensive literature analysis was done regarding treatment plans for head split fractures, but no clear consensus was found. Throughout the literature, support available, it was noted that young patients, with higher functional demand and good bone stock, sustaining a simple head split fracture benefitted from an ORIF, rather than a primary arthroplasty, which has yielded poor results [15]. Hemiarthroplasty can be a salvage option in cases of AVN or degenerative arthritis complications caused by failure of an initial ORIF procedure [3]. Most common complications include malunion, non-union, and AVN. Jost et al. reported that 10 out of 11 head split fractures treated with locking plate osteosynthesis went into malunion, highlighting the difficulty of maintaining the reduction in these fractures [18]. Gavaskar and Tummala stated that complex fracture patterns recorded a non-union rate of 20% and AVN rate of 40% with one case of glenohumeral arthritis, two cases of intra-articular screw penetration [12]. We recorded two cases of AVN failure (Schiebel Type 3) and one case of varus collapse (Schiebel Type 1). However, it is important to identify head splits, as without stabilizing these coronal plane fractures, mere fixation of proximal humerus fractures alone by a locking plate has high chances of failure. The outcome of the surgeries does depend, to a large extent, on the nature of the fracture and the quality of reduction achieved during fixation. A good anatomic head reduction and a relatively simpler fracture pattern have excellent functional outcomes in such patients (Fig. 5).

Figure 5: Follow-up in right proximal humerus head split fracture operated by antero-posterior screw augmented by plate construct – functional and radiological analysis at 36 weeks.
We acknowledge certain limitations in our study. A single-center study with a retrospective study design, limited cases, and varying degrees of surgeon expertise in handling such rare fractures are potential issues that we faced. We focused only on the simple fracture patterns of the head split, where internal fixation was implemented. The majority were from Schiebel Type 1 and 2, with a younger age group. It is difficult to standardize treatment for all head splits with such data. The more complex patterns, such as Schebel 3 and 4, were not included, as studies suggested that arthroplasty has better functional outcomes. Second, the retrospective study design has good chances of selection bias, and a low sample size might seem inadequate. Third, the selection of the patients undergoing the two different modalities of internal fixation (screws alone vs. plate-augmented-screw fixation) was completely on the operating surgeon’s choice and did not follow a strict treatment algorithm. We would also like to highlight that all the patients in the control group were operated on by six different senior surgeons over a span of 10 years, and that can affect the clinical outcomes of the patient based on the surgeon’s expertise in handling these fractures. Saying all these and considering simple head split fractures to be a very rare fracture pattern in young adults, we believe that a single-center study spanning over 10 years is just enough to indicate the efficacy of internal fixation in treating simple head split proximal humerus fractures.
Diagnosis of these simple head split fractures, without gross displacement or comminution, is difficult on AP view shoulder X-rays alone. The clinician should be aware of this fracture pattern and should screen the humeral head in higher imaging before ruling out any fractures, in suspicious cases. There is a definite lack of awareness regarding the treatment approach and fixation principles of these fractures. We conclude that primary internal fixation of simple head split fractures (Schiebel Type 1 and 2) in young adults has an excellent radiological and functional outcome. Increased complication rates are expected in the high-risk group with dissociated fracture patterns, showing varied outcomes (Schiebel Type 3). The study highlights the significant difference in outcomes of identifying and achieving a near anatomical fixation of the head split fragments, yielding higher shoulder scores and stress upon the fact that we cannot afford to miss them. Fixing head split fractures with cancellous screws alone (minimal internal fixation) recorded better functional outcomes, and patients had a lower incidence of hardware irritation. Bony union was achieved in both screws alone and plate-screw construct groups, with no significant difference in time to radiological union, proving both these modes can be used effectively as means of internal fixation in the treatment of this relatively rare variant of proximal humerus fractures.
Head split fractures are rare variant of proximal humerus fractures. Standard radiographs with double arc shadow should draw suspicion of a head split component. CT scans allow for better visualization and Schiebel’s classification allow to plan a surgical fixation approach. Good outcomes can be expected with Schiebel type 1 and 2 fractures, where the head split component is addressed appropriately.
References
- 1. Bailie AG, McAlinden MG. Complex head-splitting fracture-dislocation of the proximal humerus successfully treated with minimal internal fixation: A case report and discussion. Injury 2006;37:82-5. [Google Scholar] [PubMed]
- 2. Resch H, Tauber M, Neviaser RJ, Neviaser AS, Majed A, Halsey T, et al. Classification of proximal humeral fractures based on a pathomorphologic analysis. J Shoulder Elbow Surg 2016;25:455-62. [Google Scholar] [PubMed]
- 3. Gokkus K, Agar E, Sagtas E, Aydin AT. Proximal humerus head-splitting fracture associated with single-part anterior dislocation. BMJ Case Rep 2014;2014:bcr2013202188. [Google Scholar] [PubMed]
- 4. Shrader MW, Sanchez-Sotelo J, Sperling JW, Rowland CM, Cofield RH. Understanding proximal humerus fractures: Image analysis, classification, and treatment. J Shoulder Elbow Surg 2005;14:497-505. [Google Scholar] [PubMed]
- 5. Schiebel M, Peters P, Moro F, Moroder P. Head-split fractures of the proximal humerus. Obere Extrem 2019;14:93-102. [Google Scholar] [PubMed]
- 6. Dawson J, Rogers K, Fitzpatrick R, Carr A. The Oxford shoulder score revisited. Arch Orthop Trauma Surg 2009;129:119-23. [Google Scholar] [PubMed]
- 7. Lind T, Krøner K, Jensen J. The epidemiology of fractures of the proximal humerus. Arch Orthop Trauma Surg 1989;108:285-7. [Google Scholar] [PubMed]
- 8. Chesser TJ, Langdon IJ, Ogilvie C, Sarangi PP, Clarke AM. Fractures involving splitting of the humeral head. J Bone Joint Surg Br 2001;83:423-6. [Google Scholar] [PubMed]
- 9. Greiwe RM, Vargas-Ariza R, Bigliani LU, Levine WN, Ahmad CS. Hemiarthroplasty for head-split fractures of the proximal humerus. Orthop 2013;36:e905-11. [Google Scholar] [PubMed]
- 10. Hertel R, Hempfing A, Stiehler M, Leunig M. Predictors of humeral head ischemia after intracapsular fracture of the proximal humerus. J Shoulder Elbow Surg 2004;13:427-33. [Google Scholar] [PubMed]
- 11. Guix JM, Pedrós JS, Serrano AC. Updated classification system for proximal humeral fractures. Clin Med Res 2009;7:32-44. [Google Scholar] [PubMed]
- 12. Gavaskar AS, Tummala NC. Locked plate osteosynthesis of humeral head-splitting fractures in young adults. J Shoulder Elbow Surg 2015;24:908-14. [Google Scholar] [PubMed]
- 13. Ogawa K, Yoshida A, Inokuchi W. Posterior shoulder dislocation associated with fracture of the humeral anatomic neck: Treatment guidelines and long-term outcome. J Trauma 1999;46:318-23. [Google Scholar] [PubMed]
- 14. Robinson CM, Khan LA, Akhtar MA. Treatment of anterior fracture-dislocations of the proximal humerus by open reduction and internal fixation. J Bone Joint Surg Br 2006;88:502-8. [Google Scholar] [PubMed]
- 15. Sperling JW, Cofield RH, Rowland CM. Neer hemiarthroplasty and Neer total shoulder arthroplasty in patients fifty years old or less. Long-term results. J Bone Joint Surg Am 1998;80:464-73. [Google Scholar] [PubMed]
- 16. Schai P, Imhoff A, Preiss S. Comminuted humeral head fractures: A multicenter analysis. J Shoulder Elbow Surg 1995;4:319-30. [Google Scholar] [PubMed]
- 17. Swamy G, Schemitsch EH. Humeral head fracture dislocation: Case report and review of the literature. J Trauma 1998;44:377-80. [Google Scholar] [PubMed]
- 18. Jost B, Spross C, Grehn H, Gerber C. Locking plate fixation of fractures of the proximal humerus: Analysis of complications, revision strategies and outcome. J Shoulder Elbow Surg 2013;22:542-9. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series
August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series August 1, 2026 Functional and Cosmetic Outcome in Vertical Midline versus Horizontal Curvilinear Patella-Centered Incision in Internal Fixation of Patellar Fractures
August 1, 2026 Functional and Cosmetic Outcome in Vertical Midline versus Horizontal Curvilinear Patella-Centered Incision in Internal Fixation of Patellar Fractures July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall
July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall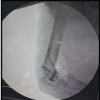 July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report
July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report