
Oblique lateral closing wedge osteotomy is a simple, safe, and effective technique for correcting pediatric cubitus varus, providing reliable deformity correction with good functional and cosmetic outcomes while minimizing complications.
Dr. Jaideep Das, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: jaideepdas01@gmail.com
Abstract
Introduction: Cubitus varus is the most common late complication following displaced supracondylar fractures of the humerus in children and is primarily caused by malunion. Although often considered cosmetic, it may lead to functional impairment and long-term complications. Corrective osteotomy remains the standard treatment, with multiple techniques described. This study evaluates the clinical and radiological outcomes of oblique lateral closing wedge osteotomy in pediatric patients.
Case Series: This case series includes five pediatric patients (2 males, 3 females; mean age 7.6 years) with post-traumatic cubitus varus deformity who underwent corrective osteotomy using the oblique lateral closing wedge technique. All patients were operated on at least 1 year after the initial injury. The mean preoperative angle of correction was 25.2° (range: 20–40°). Fixation was achieved using lateral-entry Kirschner wires. At 1-year follow-up, all patients demonstrated radiological union, restoration of carrying angle comparable to the contralateral side, and good to excellent functional outcomes based on the Mayo Elbow Performance Score.
Conclusion: Oblique lateral closing wedge osteotomy is a simple, safe, and reproducible technique for correcting cubitus varus deformity in children. It provides reliable deformity correction, satisfactory functional outcomes, and improved cosmetic alignment while minimizing complications. This represents a preliminary case series evaluating the technique and warrants validation in larger studies.
Keywords: Cubitus varus, supracondylar fracture, osteotomy, pediatric, humerus, Kirschner wire.
Supracondylar fractures of the humerus are the most common pediatric elbow injuries [1,2,3], with a peak incidence around 5–7 years of age. Cubitus varus is the most common late complication of displaced supracondylar fractures in children, with a reported incidence ranging from 3% to 58% [4]. It is also called gunstock deformity. Although trochlear avascular necrosis or physeal growth disturbances may contribute to progressive deformity, the most common cause is malunion [5].
Malunion may result from (1) inadequately treated or untreated fractures, (2) loss of reduction in conservatively treated patients, (3) inadequate fixation in surgically treated patients, and (4) medial column comminution leading to late collapse into varus [6].
The deformity consists of three components: Varus malalignment, hyperextension, and internal rotation. Hyperextension may remodel in children younger than 10 years, and internal rotation is usually compensated by shoulder movements. However, varus deformity does not remodel and requires corrective osteotomy.
Uncorrected cubitus varus may lead to complications such as lateral condylar fractures [7], posterolateral rotatory instability [8], snapping medial triceps, and ulnar nerve instability [9].
Various osteotomy techniques have been described, including lateral closing wedge, three-dimensional osteotomy [10], step-cut osteotomy [11,12], dome osteotomy, and distraction osteogenesis. The oblique lateral closing wedge osteotomy offers the advantage of correcting deformity while minimizing lateral condylar prominence without increasing surgical complexity.
This case series was conducted at a tertiary care hospital between October 2024 and September 2025. All patients were operated on at least 1-year post-trauma to rule out growth disturbances as a cause for the deformity. The study included 2 males and 3 females with an age at the time of corrective surgery ranging from 4 years to 10 years (average 7.6 years).
Informed consent was obtained from all patients’ guardians for the use of clinical data and images.
This study is presented as a preliminary case series aimed at demonstrating feasibility and reproducibility rather than establishing definitive clinical superiority. Due to the small sample size, formal statistical analysis was not performed, and results are presented descriptively.
Inclusion and exclusion criteria
Patients with significant cubitus varus deformity (carrying angle exceeding 5–10° of varus) with potential for late sequelae, skeletally immature patients at least 1 year post-trauma to rule out growth disturbances were included. Patients with skeletal maturity were excluded. Functional outcomes were assessed using the Mayo Elbow Performance Score (MEPS), a validated scoring system evaluating pain (45 points), range of motion (20 points), stability (10 points), and function (25 points), with a total score of 100. Outcomes were graded as excellent (>90), good (75–89), fair (60–74), and poor (<60).
Pre-operative planning
Before surgery, a detailed geometric assessment of both the affected and unaffected limbs should be performed to plan the osteotomy. On clinical examination using a goniometer, assess the range of motion (especially elbow flexion and extension), compare the HEW (Humerus Elbow Wrist) angle of both upper limbs, evaluate ulnar nerve stability, and document the baseline neurovascular status.
Radiographically, measure and compare the HEW (Humerus Elbow Wrist) angle and Baumann angle of both sides. The osteotomy should be planned to correct the angular difference between the affected and normal limb. It is important to ensure proper anteroposterior (AP) radiograph positioning with the elbow in neutral and the forearm fully supinated, as any flexion or extension deformity can alter the apparent HEW (Humerus Elbow Wrist) angle.
Using the AP elbow radiograph, calculate the angle of correction (AOC) by comparing carrying angles of both limbs, then draw a V-shaped osteotomy with this angle, placing its apex on the medial distal humeral cortex just above the medial epicondyle and adjusting it so the distal cut lies above the olecranon fossa and the proximal cut is equal or longer, while ensuring the distal cut is oblique to the joint line to minimize lateral prominence (Fig. 1).
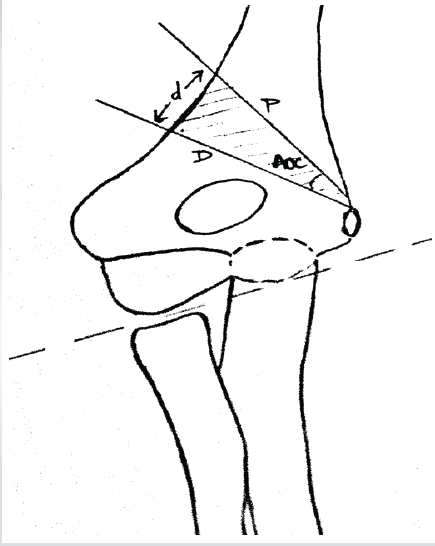
Figure 1: Initial template of the osteotomy site. The angle of correction in this example is 24°. The pathologic joint surface is noted inferiorly by a dotted line. P – proximal osteotomy, D – distal osteotomy, and d – distance between Kirschner wires designating lateral entry for osteotomy cuts.
Intra-operative procedure
Position the patient supine with the elbow on a hand table, arrange the C-arm fluoroscopy, and apply a tourniquet. Expose the distal humerus through a standard lateral approach, incise the periosteum, and perform subperiosteal elevation while preserving the medial periosteal sleeve.
Under fluoroscopic guidance, insert the first Kirschner wire (preferably distal) from lateral to medial at the planned osteotomy site. Place the second wire at a premeasured distance and angle corresponding to the AOC using a goniometer, ensuring safe placement relative to the ulnar nerve. Finally, insert two slightly divergent retrograde Kirschner wires through the lateral column in a near-vertical direction, stopping short of the distal osteotomy cut (Fig. 2 a, b, c).
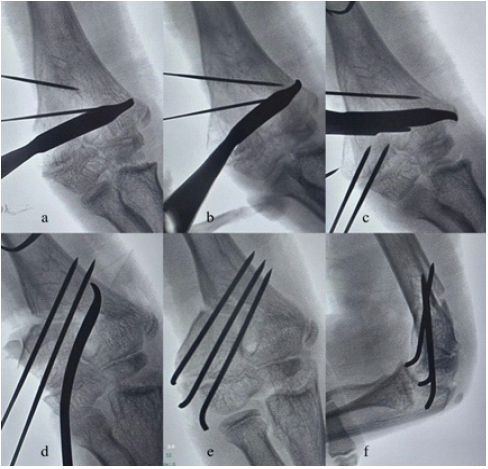
Figure 2: (a, b, c, d, e, f) Sequential fluoroscopy images of oblique lateral closing wedge osteotomy.
Perform the osteotomy using an oscillating saw or osteotome along the Kirschner wires, keeping the cut perpendicular to the distal humeral axis to avoid flexion or extension deformity, and preserve a small medial cortical hinge to protect the periosteum and ulnar nerve. Finally, remove the osteotomy guide wires.
Reduce the osteotomy by gently flexing the elbow and pronating the forearm, then confirm alignment on AP and lateral fluoroscopy. Advance the preplaced lateral K-wires across the osteotomy into the proximal fragment, add a third K-wire for stability, and reconfirm fixation. Finally, irrigate and close the wound with the elbow at 90°, cut and bend the wires outside the skin, and apply sterile dressings (Fig. 2d, e, f).
Post-operative care
Immobilize the limb in the above elbow slab at 90° elbow flexion with neutral forearm rotation. At 1 week, check radiographs and replace with a cast. Radiographs were repeated at 4 weeks to assess callus formation, if adequate callus was observed, K-wires were removed, and a gradual elbow range of movements was started. If callus formation was inadequate, the cast was continued for an additional 2 weeks.
Patients were followed up regularly for a minimum duration of 1 year to assess radiological union, maintenance of correction, and functional outcomes.
All patients followed a standardized post-operative protocol involving immobilization in an above-elbow cast for 4 weeks (except one patient who required an additional 2 weeks of immobilization), followed by K-wire removal and initiation of elbow range-of-motion exercises.
Case 1
A 10-year-old male presented with cubitus varus deformity with an AOC of 24°. Adequate intraoperative correction and stability were achieved using three K-wires. At 1-year follow-up, complete union of the osteotomy was observed with a MEPS score of 95 (excellent outcome) (Figs. 3, 4).

Figure 3: 10-year-old male with cubitus varus deformity with an angle of correction of 24° (case 1). (a and b) Pre-operative anteroposterior and lateral view X-rays of the right elbow, (c) preoperative clinical picture of the cubitus varus deformity, (d and e) intra-operative clinical picture of osteotomy, (f) fluoroscopy image of final shoot, (g) immediate post-procedure correction of deformity, (h and i) post-operative anteroposterior and lateral view X-rays of the right elbow.
Case 2
An 8-year-old female with an AOC of 22° underwent corrective osteotomy with satisfactory intraoperative correction using three K-wires. At 1-year follow-up, the patient demonstrated a MEPS score of 90 (excellent outcome) with good functional recovery, satisfactory cosmetic correction, and radiographic union.
Case 3
A 4-year-old male with a deformity requiring 20° correction underwent corrective osteotomy with fixation using two K-wires. At 1-year follow-up, the patient achieved a MEPS score of 92 (excellent outcome) (Fig. 5).
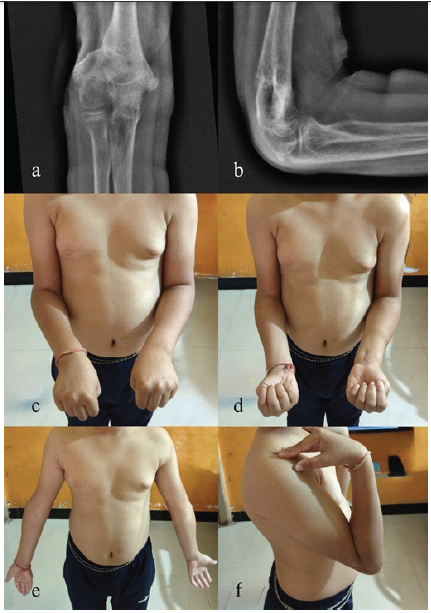
Figure 4: 1-year follow-up X-rays and elbow range of motions. (a and b) 1-year followup X-ray right elbow anteroposterior and lateral views, (c and d) follow-up clinical picture showing pronation and supination, respectively, (e and f) follow-up clinical picture showing elbow extension and elbow flexion, respectively.
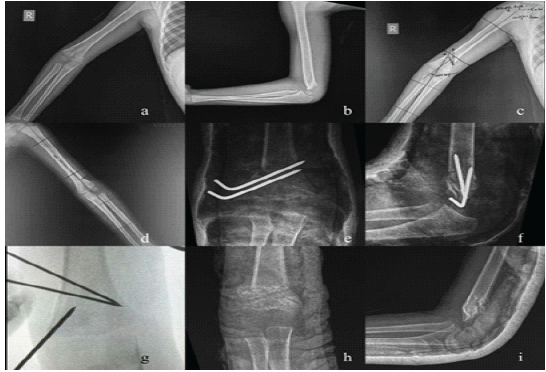
Figure 5: 4-year-old male with a deformity requiring 20° correction underwent corrective osteotomy (case 3). (a and b) Pre-operative X-rays, right elbow anteroposterior (AP) and lateral views, (c and d) pre-operative planning of the angle of correction, (e and f) immediate post-operative X-rays, right elbow AP and lateral views, (g) intra-operative fluoroscopy showing the osteotomy level, (h and i) 6-month follow-up X-ray, right elbow AP and lateral views.
Case 4
A 10-year-old female with a 20° deformity underwent corrective osteotomy with fixation using three K-wires. Radiographs at 4 weeks showed inadequate callus formation; therefore, immobilization was continued for an additional 2 weeks. At 1-year follow-up, the patient demonstrated a MEPS score of 88 (good outcome).
Case 5
A 6-year-old female presented with a severe deformity (AOC 40°) and was treated with corrective osteotomy using two K-wires. The patient developed a superficial pin-tract infection, which was managed conservatively. At 1-year follow-up, the patient achieved a MEPS score of 85 (good outcome) despite a superficial pin-tract infection.
All patients achieved radiological union and restoration of carrying angle comparable to the contralateral side at 1-year follow-up. Functional outcomes assessed using the MEPS showed excellent results in three patients and good results in two patients. The mean MEPS score was 90 ± 3.8 (range: 85–95). No cases demonstrated instability, recurrence of deformity, or major complications.
Cosmetic outcomes were also satisfactory in all patients based on carrying angle correction, consistent with Flynn’s criteria.
No patient demonstrated residual deformity, instability, or functional limitation at final follow-up (Table 1).
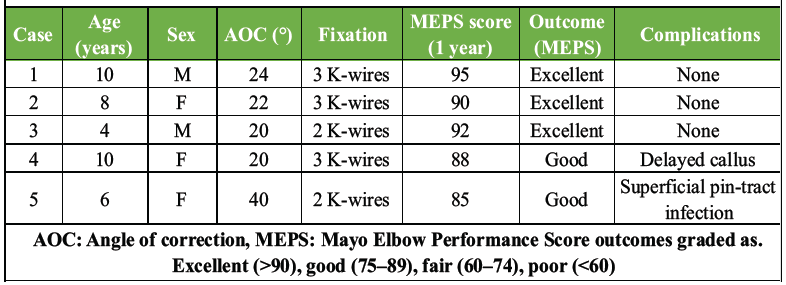
Table 1: Patient demographics, surgical details, and 1-year functional outcomes
Cubitus varus deformity following supracondylar fractures is primarily the result of malunion and requires corrective osteotomy, as the varus component does not remodel. Although previously considered a cosmetic deformity, it is now recognized to be associated with significant long-term complications such as lateral condylar fractures, posterolateral rotatory instability, and ulnar nerve pathology [7,8,9]. Therefore, surgical correction is recommended in patients with significant deformity.
The ideal osteotomy technique should be simple, reproducible, safe, and capable of achieving reliable functional and cosmetic outcomes. Early corrective osteotomy techniques for cubitus varus were described in the literature [13,14], and since then, multiple methods have evolved. The conventional lateral closing wedge osteotomy remains widely used due to its technical simplicity and predictable results, with studies reporting satisfactory correction and reliable union [15-19]. However, it is associated with lateral condylar prominence and may require cross K-wire fixation, increasing the risk of ulnar nerve injury [12].
The French osteotomy and its modifications provide stable fixation using screws and tension band constructs, with good long-term outcomes [18]. However, these techniques require hardware implantation, possible secondary removal procedures, and do not consistently address lateral condylar prominence.
More complex osteotomies have been developed to overcome these limitations. Three-dimensional osteotomies, including computer-assisted techniques, provide accurate deformity correction [10]. However, correction of internal rotation may not be necessary and may compromise stability due to reduced bone contact, while hyperextension often remodels in younger children [16]. These techniques are also resource-intensive and less practical in routine clinical settings.
Step-cut osteotomies offer improved intrinsic stability and better control over fragment translation, reducing lateral prominence [11,12]. However, they are technically demanding and increase operative time, limiting their routine use. Similarly, dome and isosceles triangular osteotomies allow multiplanar correction with improved bone contact but are less reproducible and technically more complex [6,17].
Systematic reviews suggest that no single osteotomy technique is superior, and the choice should balance technical complexity with clinical outcomes [15]. Complications such as nerve injury, loss of correction, and infection remain concerns across all methods [12].
In this context, the oblique lateral closing wedge osteotomy offers a distinct advantage by combining simplicity with improved cosmetic outcomes. The oblique orientation allows simultaneous angular correction and medial translation of the distal fragment, thereby minimizing lateral condylar prominence without increasing surgical complexity.
This technique can be performed through a standard lateral approach without extensive dissection or specialized instrumentation, making it reproducible even in low-resource settings. Furthermore, lateral-entry K-wire fixation avoids medial pin placement, reducing the risk of ulnar nerve injury [12,18].
In our series, all patients achieved satisfactory correction, restoration of carrying angle, and near-normal range of motion, with minimal complications. Functional outcomes assessed using MEPS were good to excellent in all cases, and cosmetic outcomes were also satisfactory, consistent with Flynn’s criteria. These findings are comparable to those reported with both conventional and advanced osteotomy techniques, supporting the effectiveness of this method.
While various osteotomy techniques exist, the present study highlights a practical modification using an oblique lateral cut that allows simultaneous angular correction and medial translation, thereby reducing lateral condylar prominence without increasing technical complexity. This makes the technique particularly suitable for resource-limited settings, where advanced instrumentation or implants may not be readily available.
Thus, the oblique lateral closing wedge osteotomy provides an optimal balance between simplicity, safety, and clinical outcomes, making it well suited for the routine management of cubitus varus deformity in children.
Limitations
This study has several limitations, including a small sample size, lack of a control group, and absence of statistical analysis. Although patients were followed for 1 year, longer follow-up is required to assess growth-related changes, recurrence of deformity, and late complications. In addition, as a single-center case series, the findings may not be generalizable.
Oblique lateral closing wedge osteotomy is a simple, safe, and reproducible technique for correcting cubitus varus deformity in children. It provides reliable deformity correction with sustained results at 1-year follow-up, good functional outcomes, and improved cosmetic alignment while avoiding the complications associated with more complex procedures. With proper planning and technique, it appears to be a promising and practical option in selected cases, though larger studies are required.
Oblique lateral closing wedge osteotomy provides reliable correction of cubitus varus with minimal complications and should be considered a practical technique in pediatric patients.
References
- 1. Siris IE. Supracondylar fractures of the humerus. Surg Gynecol Obstet 1939;68:201-22. [Google Scholar] [PubMed]
- 2. Mitchell WJ, Adams JP. Supracondylar fractures of the humerus in children: A ten-year review. JAMA 1961;175:573-7. [Google Scholar] [PubMed]
- 3. Griffin PP. Supracondylar fractures of the humerus. Treatment and complications. Pediatr Clin North Am 1975;22:477-86. [Google Scholar] [PubMed]
- 4. Tellisi N, Abusetta G, Day M, Hamid A, Ashammakhi N, Wahab KH. Management of Gartland’s type III supracondylar fractures of the humerus in children: The role audit and practice guidelines. Injury 2004;35:1167-71. [Google Scholar] [PubMed]
- 5. Voss FR, Kasser JR, Trepman E, Simmons E Jr., Hall JE. Uniplanar supracondylar humeral osteotomy with preset Kirschner wires for posttraumatic cubitus varus. J Pediatr Orthop 1994;14:471-8. [Google Scholar] [PubMed]
- 6. Chaudhary SD, Ghoti SD, Bochare AM. Correction of cubitus varus with lateral closed wedge osteotomy and cross K-wire fixation: Results of a prospective series of 19 patients. J Orthop Traumatol Rehabil 2019;11:104-8. [Google Scholar] [PubMed]
- 7. Davids JR, Maguire MF, Mubarak SJ, Wenger DR. Lateral condylar fracture of the humerus following posttraumatic cubitus varus. J Pediatr Orthop 1994;14:466-70. [Google Scholar] [PubMed]
- 8. O’Driscoll SW, Spinner RJ, McKee MD, Kibler WB, Hastings H 2nd, Morrey BF, et al. Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-69. [Google Scholar] [PubMed]
- 9. Spinner RJ, O’Driscoll SW, Davids JR, Goldner RD. Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg Am 1999;24:718-26. [Google Scholar] [PubMed]
- 10. Takeyasu Y, Oka K, Miyake J, Kataoka T, Moritomo H, Murase T. Preoperative, computer simulation-based, three-dimensional corrective osteotomy for cubitus varus deformity with use of a custom-designed surgical device. J Bone Joint Surg Am 2013;95:e173. [Google Scholar] [PubMed]
- 11. Davids JR, Lamoreaux DC, Brooker RC, Tanner SL, Westberry DE. Translation step-cut osteotomy for the treatment of posttraumatic cubitus varus. J Pediatr Orthop 2011;31:353-65. [Google Scholar] [PubMed]
- 12. Bali K, Sudesh P, Krishnan V, Sharma A, Manoharan SR, Mootha AK. Modified step-cut osteotomy for post-traumatic cubitus varus: Our experience with 14 children. Orthop Traumatol Surg Res 2011;97:741-9. [Google Scholar] [PubMed]
- 13. DeRosa GP, Graziano GP. A new osteotomy for cubitus varus. Clin Orthop Relat Res 1988;236:160-5. [Google Scholar] [PubMed]
- 14. Sweeney JG. Osteotomy of the humerus for malunion of supracondylar fractures. J Bone Joint Surg Br 1975;57:117. [Google Scholar] [PubMed]
- 15. Abdelmotaal HM, Abutalib RA, Khoshhal KI. The closed wedge counter shift osteotomy for the correction of post-traumatic cubitus varus. J Pediatr Orthop B 2013;22:376-82. [Google Scholar] [PubMed]
- 16. Moraleda L, Valencia M, Barco R, González-Moran G. Natural history of unreduced Gartland type-II supracondylar fractures of the humerus in children: A two to thirteen-year follow-up study. J Bone Joint Surg Am 2013;95:28-34. [Google Scholar] [PubMed]
- 17. Beuerlein MJ, Reid JT, Schemitsch EH, McKee MD. Effect of distal humeral varus deformity on strain in the lateral ulnar collateral ligament and ulnohumeral joint stability. J Bone Joint Surg Am 2004;86:2235-42. [Google Scholar] [PubMed]
- 18. Raney EM, Thielen Z, Gregory S, Sobralske M. Complications of supracondylar osteotomies for cubitus varus. J Pediatr Orthop 2012;32:232-40. [Google Scholar] [PubMed]
- 19. North D, Held M, Dix-Peek S, Hoffman EB. French osteotomy for cubitus varus in children: A long-term study over 27 years. J Pediatr Orthop 2016;36:19-24. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report
April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report January 1, 2025 Evaluating Outcomes of Step-Cut Osteotomy for Pediatric Cubitus Deformities
January 1, 2025 Evaluating Outcomes of Step-Cut Osteotomy for Pediatric Cubitus Deformities July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature
July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature