
Low-intensity Pulsed Ultrasound (LIPUS) offers a safe, non-invasive, and effective alternative for managing pediatric fracture non-union, potentially reducing the need for revision surgery.
Dr. Vikas Basa, Department of Orthopaedics, Centre for Bone and Joint, Kokilaben Dhirubhai Ambani Hospital and Research Medical Centre, Mumbai, Maharashtra, India. E-mail: basavikas@gmail.com
Abstract
Introduction: Pediatric fracture non-union is more common than generally expected. The risk factors are similar to those in adults, and treatment remains equally challenging. Surgery is almost always necessary to restart the healing process. One of the conservative options now being used is low-intensity pulsed ultrasound (LIPUS). It has been applied both in fresh fractures to stimulate all stages of healing and in non-unions, working by promoting repair at the molecular level.
Case Report: We present a case of a distal one-third humeral shaft fracture in a child that developed atrophic non-union and was treated with LIPUS. Therapy was initiated, and sequential radiographs were evaluated for healing. Encouraging signs of union were seen at 3 months, with successful fracture union at 6 months.
Conclusion: This was the 1st time LIPUS was used in India for the management of pediatric fracture non-union. While several studies have demonstrated the use of LIPUS in adult non-unions, little literature exists regarding its use in children. Even though this is a single case report, we hope it will encourage further trials and research and help establish LIPUS as a novel technique for managing pediatric fracture non-union.
Keywords: Pediatric, fracture, non-union, humerus, low-intensity pulsed ultrasound.
In clinical practice, humeral fractures are common in children. Most heal well due to the strong biological capacity for bone healing and remodeling in this age group. However, some progress to non-union despite appropriate treatment. Although non-union is often considered rare in children, it is more common than generally believed. Scaphoid (12%) and femoral neck fractures (5%) are at the highest risk, with humeral fractures (2%) not far behind [1]. Risk factors for pediatric non-union include the anatomical location of the fracture, the nature of injury (open or closed), soft tissue loss, body mass index, smoking, and Vitamin D deficiency [1,2]. When non-union occurs, intervention is usually required – surgical or otherwise – to restart the healing process [3]. Revision surgery, with success rates ranging from 68% to 96% [3,4], is standard but carries risk. Therefore, more conservative options are being explored, particularly for cases with a high surgical risk. One such method is low-intensity pulsed ultrasound (LIPUS), a form of ultrasound applied in both acute fractures and non-unions [5]. It promotes osteogenesis by inducing micromechanical stress, thereby stimulating healing at the cellular level [6]. While LIPUS is commonly used in adults, there are only a few reports of its use in pediatric fractures. We present a case of aseptic non-union of a distal humeral shaft fracture treated with LIPUS. Parents have provided informed consent for publication of this case.
Technique
The treatment of LIPUS was discussed with the parents in detail, and informed consent was obtained, as this would be the first reported case in India. Therapy was started in February 2020. The treatment area was marked on the skin, and LIPUS administered daily for 20 min. To monitor the progress and the fracture healing, monthly radiographs were obtained.
A 13-year-old boy presented in May 2019 with a fracture of the distal third of the right humeral shaft after a fall (Fig. 1).
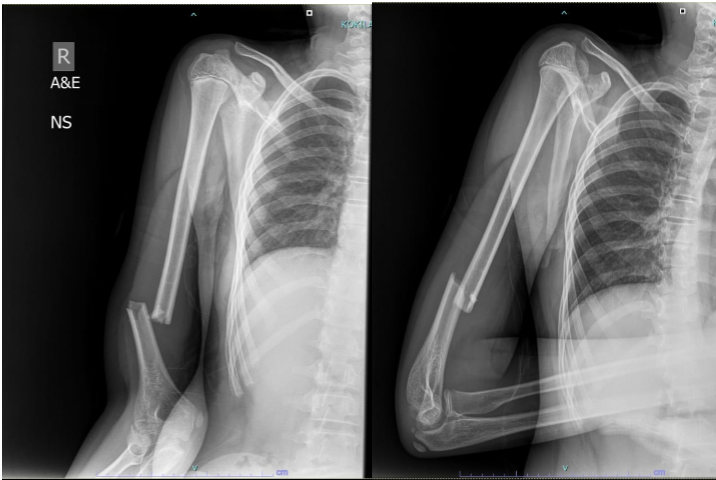
Figure 1: Initial presentation – distal humeral shaft fracture.
The injury was closed, with no neurovascular deficit. After discussion with the family, he underwent open reduction and internal fixation with plating. The procedure was uneventful, and he was discharged a few days later with intact neurovascular status (Fig. 2).
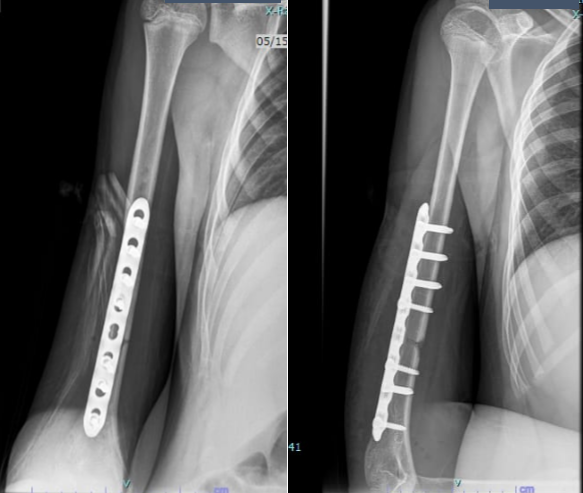
Figure 2: Post-operative radiograph after plating.
His wounds healed well, and there were no complications during the initial post-operative period. However, even after 7–8 months, radiographs showed no signs of union (Fig. 3 and 4).
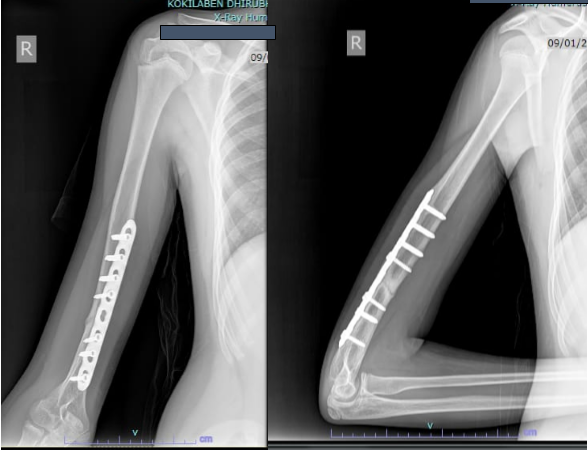
Figure 3: Radiograph at 7 months showing non-union.
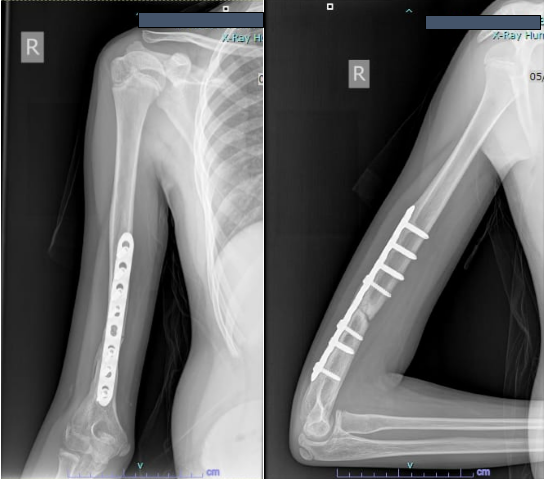
Figure 4: Radiograph at 8 months confirming non-union.
Revision plating with bone grafting was initially considered, but after a multidisciplinary team consultation and with an orthopedic surgeon in Japan experienced in LIPUS, the decision was made to attempt LIPUS therapy.
The procedure was discussed in detail with the parents, as this would be the first reported case in India. After written consent was obtained, therapy was started in February 2020. The treatment area was marked on the skin, and LIPUS was administered daily for 20 min. Monthly radiographs were taken to monitor progress.
By 3 months, early signs of healing were visible. Therapy was continued, and by 6 months the radiographs showed complete union (Fig. 5).

Figure 5: Radiograph at 3 months after starting low-intensity pulsed ultrasound showing early healing.
The patient had regained a full range of motion at the elbow and shoulder. He subsequently underwent implant removal and returned to pain-free, unrestricted activities (Fig. 6).

Figure 6: Radiograph at 6 months after low-intensity pulsed ultrasound showing complete union.
Fracture healing occurs in four phases: Inflammation, soft callus, hard callus, and remodeling. LIPUS has been shown to stimulate all of these phases [6]. Lou et al. [7] demonstrated that LIPUS reduces the time to union in fresh fractures without affecting functional recovery. A systematic review and meta-analysis by Leighton et al. [3] provided significant evidence supporting its use in non-unions. Although hypertrophic non-unions are thought to respond more readily than atrophic non-unions due to higher biological activity, evidence is inconclusive. LIPUS generates micromotion at the fracture site, which is converted into biochemical signals. This activates cellular pathways involving integrins, focal adhesions, and prostaglandin E2, ultimately leading to increased COX-2 expression and stimulation of osteogenic genes [5]. Worldwide, LIPUS is increasingly used for both fresh fractures and non-unions [4,7-10]. Tsukada et al. [11] reported promising results in patients under 18 years with early spondylolysis, showing a faster return to sports (61 days with LIPUS vs. 167 days without). Other studies have demonstrated its usefulness in unstable forearm fractures, supracondylar humeral fractures, and scaphoid non-unions in children [5,12,13]. Concerns have been raised about heat generation and possible thermal necrosis. However, modern devices produce only 1/10th to 1/50th of the heat generated by conventional physiotherapy ultrasound machines. The therapy is considered safe, with the main adverse effect being skin irritation from the coupling gel [14]. Contraindications include local skin disease, pacemaker use, pregnancy, and malignancy. The average treatment duration is 3–6 months [11]. Since this was the first case of pediatric non-union treated with LIPUS in India, the device was provided free of cost by the manufacturer (Accellus, Nippon Sigmax Co Ltd, Japan) (Fig. 7). Nevertheless, cost remains an important consideration, particularly in developing countries.

Figure 7: Low-intensity pulsed ultrasound device (Accellus, Nippon Sigmax Co Ltd, Japan).
This case demonstrates a favorable outcome for a challenging condition – pediatric fracture non-union – using LIPUS therapy. Although a single case, it highlights the potential of this non-invasive modality and may encourage further studies to establish its role as a novel treatment option in pediatric fracture non-union.
Pediatric fracture non-union, though uncommon, poses significant treatment challenges due to a lack of significant evidence and associated surgical risks. Low-intensity pulsed ultrasound offers a promising, non-invasive therapeutic alternative that stimulates bone healing at the molecular level. In this case, a successful union was achieved in an atrophic humeral non-union without the need for revision surgery. The therapy was well tolerated, safe, and effective, demonstrating its potential role in managing pediatric non-unions, especially when surgical intervention carries a higher risk or is not preferred.
References
- 1. Zura R, Kaste SC, Heffernan MJ, Accousti WK, Gargiulo D, Wang Z, et al. Risk factors for nonunion of bone fracture in pediatric patients: An inception cohort study of 237,033 fractures. Medicine (Baltimore) 2018;97:e11691. [Google Scholar] [PubMed]
- 2. Arslan H, Subaşý M, Kesemenli C, Ersuz H. Occurrence and treatment of nonunion in long bone fractures in children. Arch Orthop Trauma Surg 2002;122:494-8. [Google Scholar] [PubMed]
- 3. Leighton R, Watson JT, Giannoudis P, Papakostidis C, Harrison A, Steen RG. Healing of fracture nonunions treated with low-intensity pulsed ultrasound (LIPUS): A systematic review and meta-analysis. Injury 2017;48:1339-47. [Google Scholar] [PubMed]
- 4. Gebauer D, Mayr E, Orthner E, Ryaby JP. Low-intensity pulsed ultrasound: Effects on nonunions. Ultrasound Med Biol 2005;31:1391-402. [Google Scholar] [PubMed]
- 5. Elsebahy SY, Olama KA, Elsayed MM. Low-intensity pulsed ultrasound for healing supracondylar fracture. Physiother Q 2020;28:15-9. [Google Scholar] [PubMed]
- 6. Mundi R, Petis S, Kaloty R, Shetty V, Bhandari M. Low-intensity pulsed ultrasound: Fracture healing. Indian J Orthop 2009;43:132-40. [Google Scholar] [PubMed]
- 7. Lou S, Lv H, Li Z, Zhang L, Tang P. The effects of low-intensity pulsed ultrasound on fresh fracture: A meta-analysis. Medicine (Baltimore) 2017;96:e8181. [Google Scholar] [PubMed]
- 8. Lou S, Lv H, Li Z, Tang P, Wang Y. Effect of low-intensity pulsed ultrasound on distraction osteogenesis: A systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res 2018;13:205. [Google Scholar] [PubMed]
- 9. Padilla F, Puts R, Vico L, Raum K. Stimulation of bone repair with ultrasound: A review of the possible mechanic effects. Ultrasonics 2014;54:1125-45 [Google Scholar] [PubMed]
- 10. Nolte PA, Van Der Krans A, Patka P, Janssen IM, Ryaby JP, Albers GH. Low-intensity pulsed ultrasound in the treatment of nonunions. J Trauma 2001;51:693-702; discussion 702-3. [Google Scholar] [PubMed]
- 11. Tsukada M, Takiuchi T, Watanabe K. Low-intensity pulsed ultrasound for early-stage lumbar spondylolysis in young athletes. Clin J Sport Med 2019;29:262-6. [Google Scholar] [PubMed]
- 12. Ota T, Itoh S, Yamashita K. The efficacy and safety of combination therapy of low-intensity pulsed ultrasound stimulation in the treatment of unstable both radius and ulna fractures in children. Biomed Mater Eng 2017;28:545-53. [Google Scholar] [PubMed]
- 13. Farkash U, Bain O, Gam A, Nyska M, Sagiv P. Low-intensity pulsed ultrasound for treating delayed union scaphoid fractures: Case series. J Orthop Surg Res 2015;10:72. [Google Scholar] [PubMed]
- 14. Poolman RW, Agoritsas T, Siemieniuk RA, Harris IA, Schipper IB, Mollon B, et al. Low intensity pulsed ultrasound (LIPUS) for bone healing: A clinical practice guideline. BMJ 2017;356:j576. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series
May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report
January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report September 1, 2025 Transverse Periprosthetic Fracture With a Bent Stem Following Reverse Total Shoulder Arthroplasty – A Case Report
September 1, 2025 Transverse Periprosthetic Fracture With a Bent Stem Following Reverse Total Shoulder Arthroplasty – A Case Report April 1, 2025 Bilateral Anterior Shoulder Dislocations with Greater Tuberosity Fractures Study Design: A Case Report
April 1, 2025 Bilateral Anterior Shoulder Dislocations with Greater Tuberosity Fractures Study Design: A Case Report