
Spontaneous post-operative pneumothorax without pleural breach after posterior spinal instrumentation is exceptionally rare. This case contributes valuable insight to orthopedic, anesthetic, and perioperative practices by underscoring the need for heightened vigilance and proactive pulmonary risk assessment in spine surgery
Dr Mantu Jain, Department of Orthopaedics, All India Institute of Medical Sciences, Bhubaneswar - 751 019, Odisha, India. E-mail: montu_jn@yahoo.com
Abstract
Introduction: Prone positioning for spine surgery can present with life-threatening pulmonary complications like post-operative pneumothorax, due to barotrauma.
Case Report: A 51-year-old male with chronic instability type mid back pain and radiological features of thoracolumbar spondylodiscitis, underwent posterior stabilization, debridement and fusion under general anesthesia in prone position, without any intraoperative event. Immediately post-extubation, he developed acute dyspnea and pulmonary desaturation, for which he was treated with supportive care and was able to maintain satisfactory saturation and observed in the intensive care unit with monitoring. Persistent pulmonary desaturation and requirement of high flow oxygen led to diagnostic intervention with high-resolution computed tomography chest, which showed a small left apical pneumothorax without pleural breach, rib fracture or hemothorax. The patient did not require any invasive intervention and was managed by multidisciplinary team with oxygen therapy, non-invasive ventilation and pulmonary rehabilitation, with an uneventful recovery of pulmonary function and complete resolution of the pneumothorax by 3 weeks post-operative. He was administered appropriate medical management for spondylodiscitis.
Conclusion: Post-operative pneumothorax following prone spine surgery, likely from barotrauma, is a rare but potentially catastrophic complication that warrants high clinical vigilance, possible detection of asymptomatic bullae in pre-operative chest imaging. Early recognition, prompt imaging and coordinated multidisciplinary management are essential for optimal outcomes.
Keywords: Barotrauma, prone spine surgery, pneumothorax, pulmonary desaturation.
Posterior spinal instrumentation is a standard surgical approach for treating spinal instability caused by infection, trauma, or degenerative disease. Despite its effectiveness, the prone position required during surgery and the use of general anaesthesia can predispose patients to pulmonary complications, with an incidence reported between 0.9% and 2.1% [1,2]. Common postoperative complications include atelectasis, aspiration, pneumonia, and, rarely, pneumothorax [3]. Post-operative detection of pulmonary barotrauma, in which alveolar rupture occurs due to elevated transpulmonary pressure, is a relatively uncommon scenario but potentially life-threatening [4,5]. Most reported cases of pneumothorax or barotrauma following spinal surgery involve either an exacerbation of a pre-existing pneumothorax in the setting of traumatic spine injury [6] or an intraoperative pleural breach following an iatrogenic injury during pedicle screw insertion, predominantly in the thoracic spine surgeries [7,8,9]. In contrast, spontaneous post-operative pneumothorax without visible pleural violation is exceedingly rare. This report describes one such case scenario after posterior instrumented stabilisation for thoracolumbar spondylodiscitis, highlighting the diagnostic challenges and multidisciplinary evaluation.
A 51-year-old male presented with chronic mid-back pain and progressive difficulty in ambulation for 3 months. He had a known history of T11–T12 tubercular spondylodiscitis and was non-compliant with antitubercular therapy. There was no prior history of respiratory illness, smoking, or chronic obstructive pulmonary disease. On examination, he exhibited tenderness at the thoracolumbar junction and restricted spinal motion, with a normal neurological examination. Laboratory investigations revealed elevated erythrocyte sedimentation rate and C-reactive protein, consistent with an infective aetiology. Magnetic resonance imaging demonstrated contiguous involvement of T11–T12 vertebral bodies with destruction, disc collapse, and intra-osseous abscess (Fig. 1).
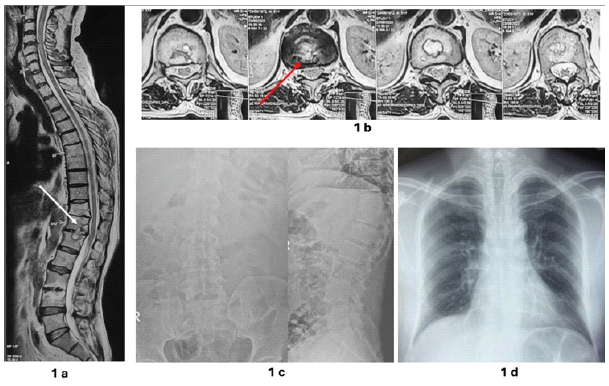
Figure 1: (a) Pre-operative magnetic resonance imaging (MRI) T2W sagittal image showing intraosseous abscess (white arrow); (b) Pre-operative MRI axial image with intraosseous abscess (red arrow); (c) Pre-operative spine radiographs; (d) Pre-operative chest radiograph without any abnormality.
His baseline disability assessment by the Oswestry Disability Index (ODI) was 60/100 [10]. In view of persistent instability-type mid-back pain and features of chronic spondylodiscitis, he was scheduled for posterior instrumented decompression (T9–L2), debridement and fusion under general anaesthesia. Anaesthesia was induced using propofol and maintained with sevoflurane in an oxygen-air mixture. The patient was ventilated in volume-controlled mode (tidal volume 8 mL/kg, peak airway pressure <28 cm H₂O, fraction of inspired oxygen 0.5). Intraoperative monitoring included end-tidal carbon dioxide (CO₂), arterial blood gas analysis (pH 7.4 and a partial pressure of oxygen [PaO₂] of 98 mmHg), and continuous pulse oximetry. The procedure lasted for 3 h with an uneventful intraoperative course. There was no clinical suspicion of a dural tear, as per the diligent probe testing for any pedicle breach. No pleural tear was suspected intraoperatively, as there was no ventilatory abnormality on monitoring. The patient was extubated in a haemodynamically stable condition, as per the standard institutional anaesthesia protocol. In the immediate post-extubation period, the patient developed sudden dyspnoea and desaturation (peripheral oxygen saturation [SpO₂] 80%). Auscultation revealed reduced air entry bilaterally with mild crepitations, with no improvement despite tracheobronchial suctioning. A significant decrease, observed in end-tidal CO₂ level, associated with an increase in peak airway pressure and with arterial blood gas analysis (pH 7.3 and a PaO₂ of 55 mmHg), was treated with the administration of high-flow oxygen by face mask, which improved oxygen saturation to 92%. He was managed with high-flow oxygen by non-invasive ventilation and observed in the intensive care unit. A post-operative chest radiograph showed a subtle left apical lucency (Fig. 2).
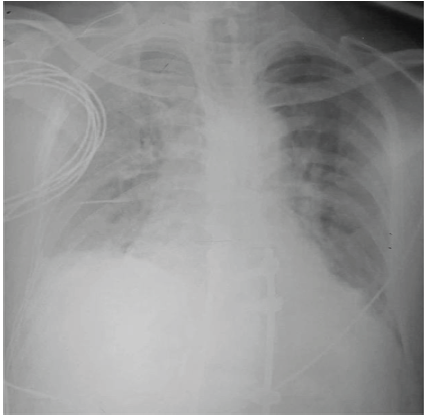
Figure 2: Post-operative chest X-ray showing lucency and features of pleural effusion.
Though there was no critical respiratory urgency, in view of persistent pulmonary desaturation of SpO₂ values to 80% on room air, whenever the patient was given a trial of room air breathing, a high-resolution computed tomography (HRCT) chest was done after achieving haemodynamic stability. Computed tomography (CT) of the chest showed a small left apical pneumothorax and a small left pleural effusion. There was no evidence of pedicle breach, screw malposition, pleural defect, rib fracture or haemothorax (Fig. 3).
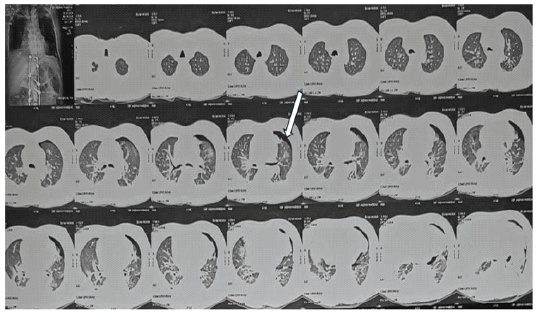
Figure 3: High-resolution computed tomography chest demonstrating left apical pneumothorax without pleural breach (White arrow).
The features of immediate postoperative desaturation merit consideration of the commonest differential diagnosis, like traumatic haemothorax or haemopneumothorax due to an inadvertent pedicle screw malposition, apart from any primary pulmonary pathology triggered during positive pressure ventilation. A multidisciplinary evaluation by an intensivist and pulmonologist was initiated, and in view of the radiological features and persistent improvement in saturation with oxygen, he was treated by conservative management and close monitoring with high-flow oxygen therapy, incentive spirometry, and pulmonary physiotherapy with improvement in arterial blood gas analysis (pH 7.4 and a PaO₂ of 85 mmHg). Serial chest imaging demonstrated gradual resolution of chest lucency over the next 5 days, and the patient was ambulated on post-operative day 6, with gradual weaning off of oxygen support over 2 weeks. Follow-up HRCT at 3 weeks and 12 weeks confirmed complete resolution of the apical pneumothorax. He was treated with anti-tubercular therapy for spondylodiscitis. On follow-up evaluation at 6 months, 1 year and 3 years follow-up, he had no pulmonary symptoms and was also evaluated with HRCT chest, which showed complete resolution of pneumothorax. His back pain improved significantly, and he remained asymptomatic with good spinal fusion radiologically, an ODI score of 10% and resolution of the intra-osseous abscess as well (Fig. 4). He had no recurrence of pulmonary symptoms at every follow-up, without any radiological signs of pulmonary lucency or pleural effusion.
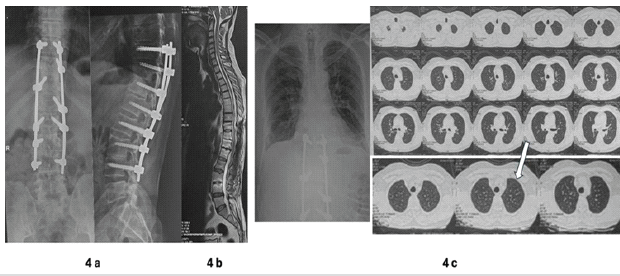
Figure 4: (a) Post-operative spine radiograph with fusion and no residual instability; (b) Post-operative T2W sagittal image at 3 years follow-up with healed abscesses and residual modic changes; (c) Follow-up computed tomography confirming complete resolution of pneumothorax (White arrow).
Any post-operative pulmonary desaturation following an uneventful spine surgery procedure in the prone position poses a major diagnostic challenge for the surgical team, impacting clinical outcomes. A normal chest radiograph, in the setting of spondylodiscitis in the thoracolumbar column, usually does not warrant any further imaging, apart from a pulmonary function test (PFT), if feasible. Post-operative barotrauma following prone spine surgery is exceedingly rare but associated with significant clinical importance due to its potential to cause rapid respiratory compromise [3,5,7,8]. Early recognition in the prone position can be challenging, as clinical clues are often masked by mechanical ventilation and limited intraoperative visualisation [11]. Postoperatively, respiratory distress may be attributed to more common causes such as atelectasis, mucus plugging, or aspiration, potentially delaying diagnosis. Thus, any unexplained desaturation after prone spine surgery should prompt early clinical diagnosis with ultrasound and needle placement and further imaging in a non-responsive patient with an X-ray/CT scan once haemodynamically stable. The predictors of any potential intra-operative pulmonary complication during prone spine surgery should be suspected by the anaesthesiologist, either by observing unexplained elevated airway pressures, the sudden fall of oxygen saturation, altered breath sounds or hypotension. The rare occurrence of post-operative desaturation and pneumothorax following prone spine surgery has been reported predominantly in scenarios like traumatic spine injury, with a pre-operative small pneumothorax that worsened in the postoperative period [6]. However, delayed onset pneumothorax has also been described, following spine deformity correction surgery, due to bullous emphysema or undetected blebs. Primary spontaneous pneumothorax in the setting of prone spine surgery can be initiated by a cascade of events, triggering rupture of subclinical or latent bullae or blebs, probably due to positive pressure ventilation or barotrauma, amenable to radiological diagnosis by a CT. Barotrauma occurs when increased alveolar pressure causes rupture, allowing air to escape into the interstitial and pleural spaces [13,14]. Risk factors include high airway pressures [15,16]. Large tidal volumes and pre-existing pulmonary blebs [12,17]. Subclinical apical blebs, often asymptomatic and undetectable on plain chest radiographs, can rupture during positive pressure ventilation, especially under prolonged anaesthesia in the prone position. In the present case, there was no identifiable pleural injury or pedicle screw-induced pulmonary injury, suggesting rupture of an undetected apical bleb under positive pressure. Although barotrauma-induced rupture of a subclinical bleb is the most plausible explanation, the exact mechanism remains speculative because no direct intraoperative evidence of alveolar rupture or pleural violation was identified. Transthoracic ultrasound is the gold standard for diagnosing pneumothorax, reducing reliance on chest X-rays and CT. It was, however, not done intraoperatively in this particular case due to the technical challenges in performing a transthoracic ultrasound in the prone position without compromising surgical field sterility. Furthermore, there was no eventful course till the time the patient was extubated, and also no alarm was raised in view of deranged pulmonary parameters by the anaesthesia team, which precluded the indication of an intraoperative transthoracic ultrasound [8]. The risk of alveolar overdistension can be minimised by lung-protective ventilation strategies, limiting plateau pressure to <30 cm H₂O and using moderate positive end-expiratory pressure [18,19]. Anaesthesia records in our case documented peak airway pressure consistently below 28 cm H₂O and tidal volumes of 8 mL/kg. However, continuous plateau-pressure and driving-pressure trends were not prospectively recorded, which we acknowledge as a limitation. Future studies should incorporate real-time logging of dynamic compliance and driving pressures for better stratification of barotrauma risk. The tidal volume of 8 mL/kg, while within the norms of conventional practice, is higher than the 6 mL/kg prescribed in lung protective protocols. The consideration of lower tidal volumes in future cases involving high-risk patients also warrants merit. In addition, clear communication between anaesthesiologists and surgeons is crucial to promptly identify abnormal ventilatory patterns and prioritise life-saving pulmonary management before completion of spine surgery. Patients on mechanical ventilation or those requiring positive pressure ventilation with pneumothorax need prior tube thoracostomy to prevent tension pneumothorax. Conservative management is safe and effective for small, stable pneumothoraces, whereas larger or tension pneumothoraces necessitate intercostal drainage [20]. The decision to manage the patient conservatively was taken based on improvement in clinical parameters and imaging. Literature stipulates that small stable pneumothoraces in haemodynamically stable patients may be managed conservatively. Emergency management includes needle decompression followed by tube thoracostomy with an underwater seal. Even small pneumothoraces can cause severe cardiopulmonary effects in patients with limited pulmonary reserve. Positive pressure ventilation can enlarge air leaks and hinder pleural healing; hence, low tidal volumes (6 mL/kg) with high respiratory rates are advised to protect the opposite lung. Traditional management is chest tube thoracostomy, but image-guided small-bore catheters (7–10 Fr) show a 68.6% success rate with no major complications, comparable to large-bore tubes (55% success). Persistent air leak or failed lung expansion warrants thoracic surgical consultation within 3–5 days. PFTs were not done preoperatively in view of the absence of any clinical/radiological features suggesting compromised pulmonary reserve. Postoperatively, the patient demonstrated complete recovery of pulmonary function. We do recommend PFTs in select high-risk patients before these surgeries, as well as during the recovery phase, for objective documentation of the clinical course. Pre-operative HRCT chest was not performed because the patient had no respiratory symptoms, smoking history, or radiographic abnormalities on chest radiography. Therefore, the presence of pre-existing asymptomatic blebs or bullae could not be conclusively excluded. The present case highlights the crucial relevance of suspecting a pulmonary event, which was either intraoperatively exacerbated or even a pre-operative trigger that manifested in the course of operative events, as the pre-operative chest radiograph, reviewed retrospectively, shows a radiograph without any clue of pulmonary effusion or any other pulmonary pathology. However, as the patient had no pulmonary symptoms, with a normal clinical examination, the patient was taken up for the surgical procedure without a CT scan of the chest, which might have shown a pre-existing, asymptomatic bulla. The causal relationship between barotrauma and pneumothorax in this case is indeed inferred from the temporal relationship between the surgery and onset of the patient’s symptoms. Establishing causality beyond doubt would have required a thoracoscopy/autopsy, neither of which was indicated/applicable in this case. The background of tubercular spondylodiscitis also raises the possibility of pulmonary tuberculosis (TB) that could have led/contributed to the pneumothorax. However, in the absence of any evidence of active/healed TB in the pre-operative X-ray and post-operative HRCT, this possibility can be safely assumed to be very unlikely. Our experience further reinstates the utility of a pre-operative CT in select patients with risk factors. Although this case report describes a single patient, the rarity of spontaneous pneumothorax following prone spine surgery warrants that each individual instance be meticulously analysed and followed up. Early diagnosis and multidisciplinary supervision led to favourable recovery in this case. The patient’s perspective was positive; he appreciated the prompt recognition and conservative management that prevented invasive intervention. This case highlights the need for vigilance in detecting rare pulmonary complications after spine surgery and reinforces the importance of preoperative risk assessment for subclinical lung pathology.
Surgical teams involved in prone surgeries under general anaesthesia often face sudden worsening of pulmonary parameters, either intraoperatively or immediately post-extubation. It is prudent to follow a standardised algorithm and checklist-based exclusion of the probable offending factor, understanding the role of imaging vis-à-vis urgent intensive care procedures like tube thoracostomy. Given the rare nature of this case, we were unable to identify a standardised checklist in the existing literature. Based on the clinical course, observations, and key lessons learned, we have developed a practical checklist that may help clinicians recognise and manage similar situations in the future in post-operative desaturation, as shown in Fig. 5.

Figure 5: Algorithm for pre-operative assessment and clinical workflow for post-operative pulmonary desaturation.
This proposed algorithm has not been prospectively validated and can be regarded as an adjunctive clinical aid rather than a standardised protocol. Post-operative pulmonary barotrauma after prone spine surgery, though uncommon, requires early recognition, prompt imaging, and multidisciplinary management. The case emphasises the relevance of preventive strategies, identifying subclinical pulmonary abnormalities during surgical planning to prevent complications.
Spontaneous post-operative pneumothorax without pleural breach after posterior spinal instrumentation is extremely rare. Despite its rarity, post-operative pneumothorax should remain a differential diagnosis in unexplained desaturation, as prompt recognition is crucial for optimal outcomes. The multidisciplinary approach used in this case may not be readily available in all healthcare settings, particularly where resources are limited. However, the key aspects of management – maintaining a high index of suspicion, obtaining timely imaging, and providing appropriate respiratory support – can be applied across a wide range of clinical environments. This case highlights the need for vigilant monitoring and proactive pulmonary risk assessment in spine surgery.
References
- 1. Kim BD, Smith TR, Lim S, Cybulski GR, Kim. Predictors of pulmonary complications after spine surgery: A multivariate analysis. Spine J 2014;14:799-807. [Google Scholar] [PubMed]
- 2. Lee JH, Kim KT, Lee SH, Kang KJ, Lee JS, Son ES. Three different methods in deformity correction of degenerative flat back: a single surgeon’s experience with 64 consecutive cases. Asian Spine J 2015;9:361-9. [Google Scholar] [PubMed]
- 3. Ki S, Choi B, Cho SB, Hwang S, Lee J. Unexpected tension pneumothorax developed during anaesthetic induction aggravated by positive pressure ventilation: a case report. Medicina (Kaunas). 2023;59(9):1631. doi:10.3390/medicina59091631. [Google Scholar] [PubMed] [CrossRef]
- 4. Ioannidis G, Lazaridis G, Baka S, Mpoukovinas I, Karavasilis V, Lampaki S, Kioumis I, Pitsiou G, Papaiwannou A, Karavergou A, et al. Barotrauma and pneumothorax. J Thorac Dis. 2015;7(Suppl 1):S38-S43. [Google Scholar] [PubMed]
- 5. Lou Y, Zhang Y, Wang Z, Zhao C, Li Z, Huang Q, Tang H, Xiao J. Large pneumothorax following thoracic and lumbar tumour surgery: risk factors and management strategies. Front Surg. 2023;10:1066841. [Google Scholar] [PubMed]
- 6. Levin NJ, Ghorishi AR, Charnowitz N, Rosenthal A, Ditchek J. Pneumothorax in the setting of spinal surgery: A case report and review of the literature. Cureus 2022;14:e26743. [Google Scholar] [PubMed]
- 7. Yamada K, Abe Y, Satoh S, et al. Pneumothorax by penetrating endplate screw for diffuse idiopathic skeletal hyperostosis: a case report. Clin Case Rep. 2023;11:e6877. [Google Scholar] [PubMed]
- 8. Wu L, Zhang X, Wang Y, et al. Risk factors for pulmonary complications after posterior spinal instrumentation and fusion in the treatment of congenital scoliosis: a case-control study. BMC Musculoskelet Disord. 2019;20:331. doi:10.1186/s12891-019-2708-8. [Google Scholar] [PubMed] [CrossRef]
- 9. Taccone P, Chiumello D. Prone positioning in the ICU. In: Hall JB, Schmidt GA, Kress JP, editors. Principles of Critical Care. New York: Oxford University Press; 2016. Chapter 99. doi:10.1093/med/9780199600830.003.0099. [Google Scholar] [PubMed] [CrossRef]
- 10. Fairbank JC, Pynsent The Oswestry Disability Index. Spine (Phila., Pa., 1976) 2000;25:2940-52; discussion 2952. [Google Scholar] [PubMed]
- 11. Cho W, Cho. Complications in posterior spinal fusion. Asian Spine J 2020;14:910-20. [Google Scholar] [PubMed]
- 12. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, Adhikari NKJ, Amato MBP, Branson R, Brower RG, Ferguson ND, Gajic O, Gattinoni L, Hess D, Mancebo J, Morris AH, Rubenfeld GD, Pham T, Pesenti A, Stewart TE, Slutsky AS, Brochard LJ An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: Mechanical ventilation in adult patients with acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine. 2017;195:1253–1263 [Google Scholar] [PubMed]
- 13. Noppen M, Dekeukeleire T. Pneumothorax: Epidemiology, pathophysiology, and cause. Eur Respir Rev 2008;17:117-21. [Google Scholar] [PubMed]
- 14. Anzueto A, Frutos-Vivar F, Esteban A, Alía I, Brochard L, Stewart T, Benito S, Tobin MJ, Elizalde J, Palizas F, et al. Incidence, risk factors and outcome of barotrauma in mechanically ventilated patients. Intensive Care Med. 2004;30(4):612-619. [Google Scholar] [PubMed]
- 15. Gammon RB, Shin MS, Buchalter SE. Pulmonary barotrauma in mechanical ventilation. Patterns and risk factors. 1992;102(2):568-572. [Google Scholar] [PubMed]
- 16. Diaz R, Heller D. Barotrauma and Mechanical Ventilation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. [Google Scholar] [PubMed]
- 17. American Thoracic Management of spontaneous pneumothorax: Clinical practice guideline. Am J Respir Crit Care Med 2020;201:e24-41. [Google Scholar] [PubMed]
- 18. Rahman NM, Asciak R, Bedawi EO, Bhatnagar R, Clive AO, Hassan M, et al. British Thoracic Society clinical statement on pleural procedures. Thorax 2023;78:s43-s68. [Google Scholar] [PubMed]
- 19. Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, Schoenfeld D, Thompson BT; National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med. 2004;351(4):327-336. [Google Scholar] [PubMed]
- 20. Dreyfuss D, Saumon: Ventilator-induced lung injury: Lessons from experimental studies. Am J Respir Crit Care Med 1998;157:294-323. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 1-Year Follow-Up Result of Early Definitive Management of the Trauma Patient in a Tertiary Health Care Centre
January 1, 2025 1-Year Follow-Up Result of Early Definitive Management of the Trauma Patient in a Tertiary Health Care Centre November 1, 2024 Hydropneumothorax in an Isolated Midshaft Clavicle Fracture
November 1, 2024 Hydropneumothorax in an Isolated Midshaft Clavicle Fracture October 10, 2022 A Rare Case of Distal Femur Physeal Fracture Dislocation with Positional Vascular Compromise in an Adolescent Male
October 10, 2022 A Rare Case of Distal Femur Physeal Fracture Dislocation with Positional Vascular Compromise in an Adolescent Male February 1, 2025 Stealth Navigation with iFuse-TORQ Implant for Sacroiliac Joint Fusion Technique Guide
February 1, 2025 Stealth Navigation with iFuse-TORQ Implant for Sacroiliac Joint Fusion Technique Guide