
[box type=”bio”] What to Learn from this Article?[/box]
Technique of Arthroscope assisted intralesional curettage of giant cell tumor.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 6-8 | Aashay Kekatpure, Milind Pimprikar, Aditya Kekatpure. DOI: 10.13107/jocr.2250-0685.259
Authors: Aashay Kekatpure[1], Milind Pimprikar[1], Aditya Kekatpure[1]
[1] Department of Orthopaedics, ADTOOS Clinic And Pimprikar Hospital Nasik. India.
Address of Correspondence:
Dr. Aashay Kekatpure,
C/O Dr Milind Pimprikar, Pimprikar Hospital. Govind Nagar Chowk No. 5. Behind Prakash Hotel. Bombay Naka.
Nashik. Maharashtra. India.
E-mail: dr.aashayk@gmail.com
Abstract
Introduction: Incomplete intralesional curettage remains the most important factor contributing to the recurrence of the GCT tumor. A 360 degree view of the tumor cavity can be achieved with the help of an arthroscope, which can aid complete intralesional curettage.
Case Report: This technical note describes the use of arthroscope assisted curettage of the distal femur GCT.
Conclusion: Use of an arthroscope can improve the visibility for intralesional curettage 5 of Giant Cell tumor.
Keywords: Giant Cell Tumor; Arthroscope; Curettage.
Introduction
Giant cell tumor is a rare and enigmatic tumor with unpredictable clinical course and treatment outcomes [1,6]. Surgery is the mainstay of treatment and usually consists of intra-lesional curettage [6,7,8] local control rates range from 80% to 90% after this procedure [9,10,11,12]. Patients with extensive, recurrent, and/or biologically more aggressive tumors may require wide excision [13,14].Intralesional curettage is reasonable when the functional benefit outweighs the risk of recurrence as is the case in many cases of GCT of distal femur [14]. To avoid incomplete intralesional curettage we propose arthroscope assisted curettage and provide the video of the same.
Case report
A 33 yrs old female presented to us with knee pain after history of fall with minimal swelling .Anterior and lateral knee radiograph showed features suggestive of Giant cell tumor and intercondylar fracture. A CT scan further strengthed the suspicion of GCT (Fig 1 & 2). 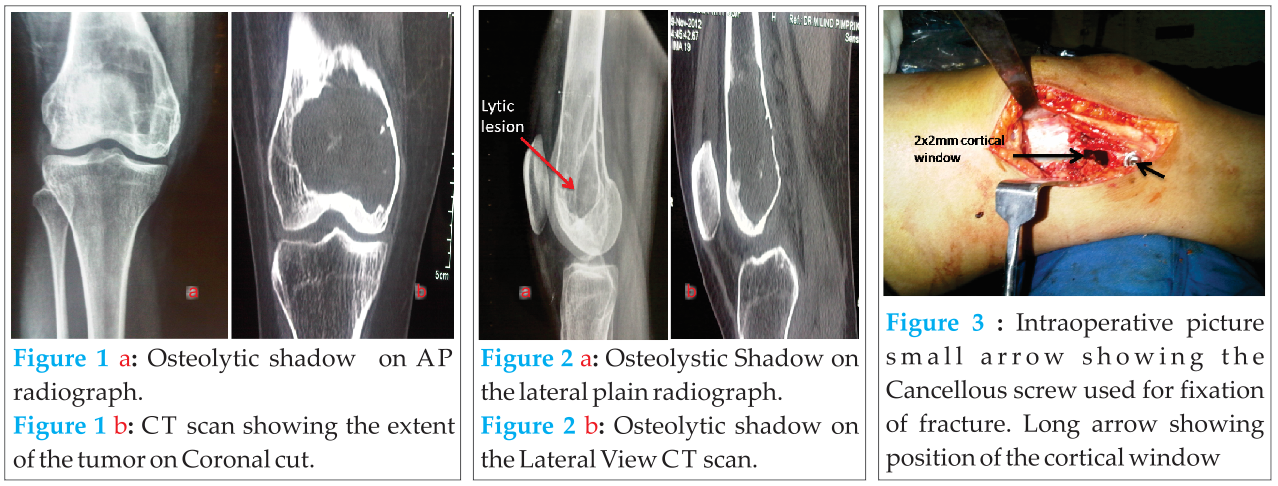 Surgical decision of arthroscope assisted fixation of the fracture and intralesional curettage of the GCT was contemplated considering the age and proximity to the joint. With knee in 90deg flexion standard antero-lateral portal was taken at the soft spot above the joint line 2cm lateral to the patellar tendon. Hematoma was drained, antero-medial portal was established with outside in technique. The joint was copiously irrigated. The reduction of the fracture was confirmed under vision with the help of the arthroscope. A guide wire was passed from the lateral femoral condyle , 6.5 mm drill bit was used and with a 70mm 6.5mm CC screw with washer fracture was fixed. The portals were closed with 3.0 ethilone. A lateral longitudinal incision was taken on the distal femur extending upto the screw. The fascia was incised to expose the lateral femoral condyle . A cortical window of 2x2cm was made with an intact perisosteal hinge 2cms above the screw head (Fig 3). A 30 deg arthroscope with a light source was introduced through the cortical window .After introduction of the scope the light source cable was rotated to have a 360 deg visualization of the tumor cavity.The surrounding structures of the cortical window were covered with sterile mop to avoid spillage of the tumor cells coming out along with the irrigation fluid in the surrounding tissue. The irrigation fluid was started . A small curette , 4.5 mm shaver tip and a high speed burr were used to curette the GCT cavity. The end point of curettage was visualization of the normal cortical bone through the arthroscope. During the curettage copious normal saline was used for irrigation of the cavity .After curettage dry visualization of the cavity was done. Later the cavity was filled with bone graft harvested from the ipsilateral iliac crest. The remaining cavity was filled with poly methyl methacrylate cement. Homeostasis was achieved. Incision was closed in layers over drain. Knee range of movements was started immediate post operatively as tolerated. Patient was advised to walk with a walker non-weight bearing for 4weeks subsequently was advised to bear weight. Patient was asked to come for follow up every month in the initial 6 months. On every visit radiograph of the knee was done to identify signs of recurrence. After one year of follow up the patient has full range of movement and no signs of recurrence on serial radiographs (Fig 4 & 5).
Surgical decision of arthroscope assisted fixation of the fracture and intralesional curettage of the GCT was contemplated considering the age and proximity to the joint. With knee in 90deg flexion standard antero-lateral portal was taken at the soft spot above the joint line 2cm lateral to the patellar tendon. Hematoma was drained, antero-medial portal was established with outside in technique. The joint was copiously irrigated. The reduction of the fracture was confirmed under vision with the help of the arthroscope. A guide wire was passed from the lateral femoral condyle , 6.5 mm drill bit was used and with a 70mm 6.5mm CC screw with washer fracture was fixed. The portals were closed with 3.0 ethilone. A lateral longitudinal incision was taken on the distal femur extending upto the screw. The fascia was incised to expose the lateral femoral condyle . A cortical window of 2x2cm was made with an intact perisosteal hinge 2cms above the screw head (Fig 3). A 30 deg arthroscope with a light source was introduced through the cortical window .After introduction of the scope the light source cable was rotated to have a 360 deg visualization of the tumor cavity.The surrounding structures of the cortical window were covered with sterile mop to avoid spillage of the tumor cells coming out along with the irrigation fluid in the surrounding tissue. The irrigation fluid was started . A small curette , 4.5 mm shaver tip and a high speed burr were used to curette the GCT cavity. The end point of curettage was visualization of the normal cortical bone through the arthroscope. During the curettage copious normal saline was used for irrigation of the cavity .After curettage dry visualization of the cavity was done. Later the cavity was filled with bone graft harvested from the ipsilateral iliac crest. The remaining cavity was filled with poly methyl methacrylate cement. Homeostasis was achieved. Incision was closed in layers over drain. Knee range of movements was started immediate post operatively as tolerated. Patient was advised to walk with a walker non-weight bearing for 4weeks subsequently was advised to bear weight. Patient was asked to come for follow up every month in the initial 6 months. On every visit radiograph of the knee was done to identify signs of recurrence. After one year of follow up the patient has full range of movement and no signs of recurrence on serial radiographs (Fig 4 & 5).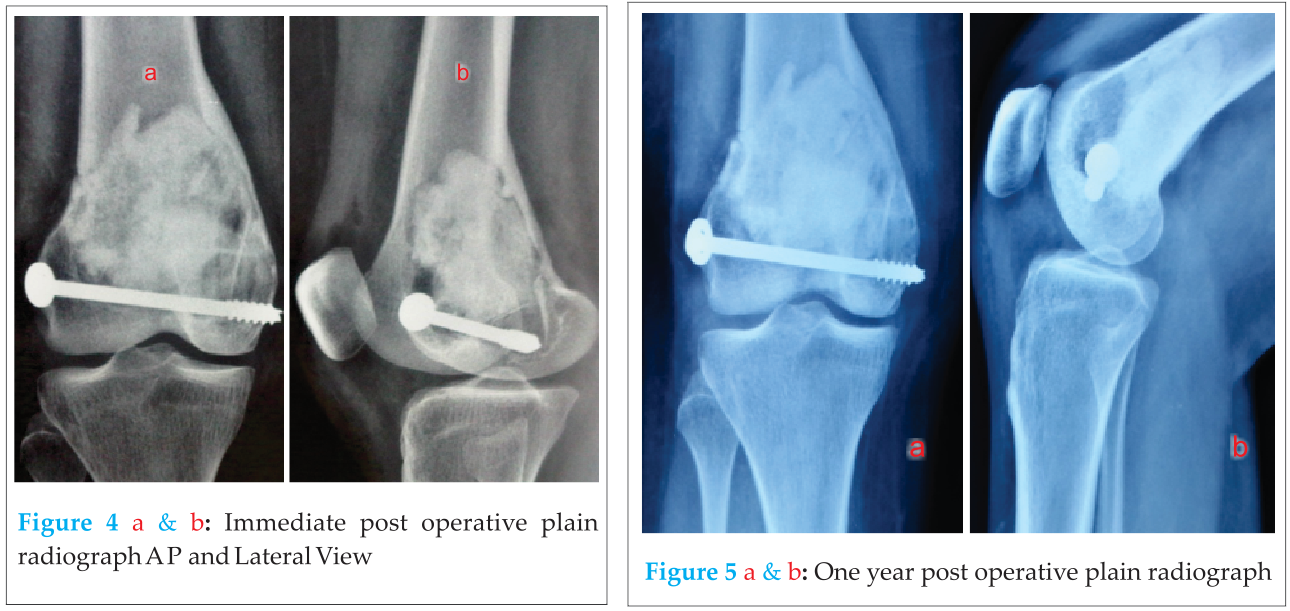
Discussion
Giant Cell Tumor of Bone (GCT) is a primary bone tumor of mesenchymal origin presenting as a localized osteolytic lesion [10,11,12]. GCT mostly affects the meta-epiphyseal region of long bones [10,11,12].The distal femur and the proximal tibia are the most common sites of occurrences. Females are more commonly affected in their third and fourth decade of life. GCT exhibits locally aggressive features with an unpredictable course of progression [10,11,12].
Although close to 100% local control is achieved with en bloc resection [13] procedure is associated with functional disabilities due to the peri-articular location of the tumor [14]. Hence, intralesional curettage has been accepted as modality of treatment for GCT of bone. This method of treatment carries a inherent risk of higher recurrence rate. Recurrence rates are approximately 16% to 45% [10,13,15,17]. To reduce high local recurrence rates thermal adjuvants and cytotoxic agents are being advocated. These include phenol, polymethylmethacrylate (PMMA), argon beam coagulation, anhydrous alcohol, and liquid nitrogen [18,23].
Blackley et al. reported on the recurrence rates of GCT in 59 patients between 1986 and 1996 treated with intralesional procedures using high-speed burr alone [15]. They concluded that the adequacy of the removal of the tumor rather than the use of adjuvant modalities is what determines the risk of recurrence.
Intralesional curettage is an effective treatment for majority of GCT. Patients with extensive, aggressive, and/or incompletely resectable GCTs are the one’s who require wide excision and curettage. Torres-Eguía RJ et al [25] has described Epiphyseal femoral tumour resection under intraosseous endoscopic control. They had resected 4 benign cystic femoral head tumours under intraosseous endoscopic control. The resections were completely extraarticular through a tunnel made in the femoral neck from the lateral cortex. The procedures were assessed endoscopically with the help of a standardarthroscope. With a minimum follow-up of 1 year (range 1-16 years), there were no recurrences.In our case there was no difficulty in inserting cement or bone graft.
Conclusion
Our technique of use of Arthroscope can be a valuable addition to the treatment GCT. The salient feature of this technique is it gives a 360 deg view of the tumor cavity through a small cortical window thus avoiding fuctional disability by preserving the cortical shell.
Clinical Message
Use of arthroscope for intralesional curettage aids in 360 degree visualization of the tumor cavity with minimal compromise of the cortical integrity.
References
1. Klenke FM, Wenger DE, Inwards CY, Rose PS, Sim FH. Giant cell tumor of bone: risk factors for recurrence. Clin Orthop Relat Res. 2011;11:591–599. doi: 10.1007/s11999-010-1501-7.
2. .Zuo D, Zheng L, Sun W, Fu D, Hua Y, Cai Z. Contemporary adjuvant polymethyl methacrylate cementation optimally limits recurrencein primary giant cell tumor of bone patients compared to bone grafting: a systematic review and meta-analysis. World J Surg Oncol. 2013 Jul 16;11:156
3. Goldenberg RR, Campbell CJ, Bonfiglio M. Giant-cell tumor of bone: an analysis of two hundred and eighteen cases. J Bone Joint Surg Am. 1970;11:619–664.
4. Sanerkin NG. Malignancy, aggressiveness, and recurrence in giant cell tumor of bone. Cancer. 1980;11:1641–1649.
5. Pazionis TJ, Alradwan H, Deheshi BM, Turcotte R, Farrokhyar F, Ghert M. A Systematic Review and Meta-Analysis of En-Bloc vs Intralesional Resection for Giant Cell Tumor of Bone of the Distal Radius. Open Orthop J. 2013 Apr 28;7:103-8.
6. Gitelis S, Mallin BA, Piasecki P. Intralesional excision compared with en bloc resection for giant-cell tumors of bone. J Bone Joint Surg Am. 1993;75:1648–55.
7. Liu YP, Li KH, Sun BH. Which treatment is the best for giant cell tumors of the distal radius? A meta-analysis. Clin Orthop Relat Res. 2012;470()(10 ):2886–94.
8. Bini SA, Gill K, Johnston JO. Giant cell tumor of bone: curettage and cement reconstruction. Clin Orthop Relat Res. 1995;321:245–250.J Bone Joint Surg Br. 2012 Jul;94(7):882-8. doi: 10.1302/0301-620X.94B7.28927.
9. Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. Journal of Bone and Joint Surgery. American.1987;69(1):106–114.
10. Turcotte RE, Wunder JS, Isler MH, et al. Giant cell tumor of long bone: a Canadian Sarcoma Group study. Clinical Orthopaedics and Related Research. 2002;(397):248–258.
11. Balke M, Schremper L, Gebert C, et al. Giant cell tumor of bone: treatment and outcome of 214 cases. Journal of Cancer Research and Clinical Oncology. 2008;134(9):969–978. [
12. Rock M. Curettage of giant cell tumor of bone. Factors influencing local recurrences and metastasis. La Chirurgia Degli Organi di Movimento. 1990;75(1):204–205.
13. Su Y-P, Chen W-M, Chen T-H. Giant-cell tumors of bone: an analysis of 87 cases. International Orthopaedics. 2004;28(4):239–243.
14. Gitelis S, Mallin BA, Piasecki P, Turner F. Intralesional excision compared with en bloc resection for giant-cell tumors of bone.Journal of Bone and Joint Surgery. American. 1993;75(11):1648–1655.
15. Blackley HR, Wunder JS, Davis AM, White LM, Kandel R, Bell RS. Treatment of giant-cell tumors of long bones with curettage and bone- grafting. Journal of Bone and Joint Surgery. American. 1999;81(6):811–820.
16. Ghert MA, Rizzo M, Harrelson JM, Scully SP. Giant-cell tumor of the appendicular skeleton. Clinical Orthopaedics and Related Research. 2002;(400):201–210.
17. O’Donnell RJ, Springfield DS, Motwani HK, Ready JE, Gebhardt MC, Mankin HJ. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. Journal of Bone and Joint Surgery. American. 1994;76(12):1827–1833.
18. Lewis VO, Wei A, Mendoza T, Primus F, Peabody T, Simon MA. Argon beam coagulation as an adjuvant for local control of giant cell tumor. Clinical Orthopaedics and Related Research. 2007;(454):192–197.
19. Becker WT, Dohle J, Bernd L, et al. Local recurrence of giant cell tumor of bone after intralesional treatment with and without adjuvant therapy. Journal of Bone and Joint Surgery. American. 2008;90(5):1060–1067.
20. Dürr HR, Maier M, Jansson V, Baur A, Refior HJ. Phenol as an adjuvant for local control in the treatment of giant cell tumour of the bone. European Journal of Surgical Oncology. 1999;25(6):610–618.
21. Jones KB, DeYoung BR, Morcuende JA, Buckwalter JA. Ethanol as a local adjuvant for giant cell tumor of bone. The Iowa Orthopaedic Journal. 2006;26:69–76.
22. Kivioja AH, Blomqvist C, Hietaniemi K, et al. Cement is recommended in intralesional surgery of giant cell tumors: a Scandinavian Sarcoma Group study of 294 patients followed for a median time of 5 years. Acta Orthopaedica. 2008;79(1):86–93.]
23. Malawer MM, Bickels J, Meller I, Buch RG, Henshaw RM, Kollender Y. Cryosurgery in the treatment of giant cell tumor: a long term followup study. Clinical Orthopaedics and Related Research. 1999;(359):176–188.
24. MendenhallWM1, Zlotecki RA, Scarborough MT, Gibbs CP, MendenhallNP Giant cell tumor of bone. Am J Clin Oncol. 2006 Feb;29(1):96-9.
25. Torres-Eguía RJ1, Colmenero Rolón CA, Arauz De Robles S, Guillen García P Epiphyseal femoral tumour resection under intraosseous endoscopic control. Hip Int. 2010;20 Suppl 7:S32-5. doi: 10.5301/HIP.2010.4469.
| How to Cite This Article: Kekatpure A, Pimprikar M, Aditya Kekatpure A. Arthroscope Assisted Intralesional Curettage of GCT. Journal of Orthopaedic Case Reports 2015 April-June;5(2):6-8. Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-259-fulltext-2/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


