
[box type=”bio”] What to Learn from this Article?[/box]
Ipsilateral Closed Clavicle and Scapular Spine Fracture with Acromioclavicular Joint Disruption.
Case Report | Volume 5 | Issue 2 | JOCR April-June 2015 | Page 58-61 | Raghavendra S Kembhavi, Boblee James. DOI: 10.13107/jocr.2250-0685.276
Authors: Raghavendra S Kembhavi[1], Boblee James[1]
[1] Department of Orthopaedics, Sri Lakshmi Narayan Institute Of Medical Sciences, Pondicherry. India.
Address of Correspondence
Dr Raghavendra S Kembhavi,
Plot No 8, Rajaannamalai Nagar, Behind Police Quaters, Pondicherry-605006. India.
Email: caringdocs@yahoo.com
Abstract
Introduction: Injuries around shoulder and clavicle are quite common. Injuries involving lateral end of clavicle involving acromioclavicular joints are commoner injuries. In this rare injury , we report about a case involving clavicle and scapular spine fracture with acromioclavicular disruption which has never been described in English literature as per our knowledge.
Case Report: A patient with closed clavicle and scapular spine fracture with acromioclavicular joint disruption was treated with open reduction and internal fixation of clavicle and scapular spine as a staged procedures. Six months post operatively, patient had excellent functional recovery with near full range of movements.
Conclusion: Though rare complex injury,clavicle fracture with scapular spine fracture with acromioclavicular disruption , when managed properly with good physiotherapy protocol post operatively will result in good clinical and functional outcome.
Keywords: Acromioclavicular joint, scaplar spine, pendulum exercises, corocoid process.
Introduction
Injuries around shoulder and clavicle are quite common. Injuries involving lateral end of clavicle with acromioclavicular joint disruption are commoner injuries[1]. On the other hand midshaft clavicle fractures with acromioclavicular joint(AC) disruption are relatively rare and have been described only few times in English literature[2,3,4]. Furthermore, mid shaft clavicle fracture with acromioclavicular joint disruption in association with scapular spine fracture has never been documented in English literature.
In this article, we report a case where all three things are injured namely, clavicle fracture, scapular spine fracture and acromioclavicular joint disruption. Our emphasis was on this rarest injury and how we managed this with staged surgeries alongwith strict physiotherapy protocol to get good functional outcome.
Case report
38 year male met with road traffic accident while being hit by heavy four wheeler while walking by the side of road. He sustained injury overhead and right shoulder. Patient was treated for head injury elsewhere and later he came to our institution for shoulder injury. On presentation, there was gross swelling over right shoulder with ecchymosis with tenderness over midclavicle, AC joint and over scapular spine region. There was no distal neurovascular deficit. X rays revealed, clavicle fracture comminuted at mid-distal one-third junction with scapular spine fracture alongwith acromioclavicular joint disruption(Fig 1). CT(Computed Tomography)scan showed lateral fragment of clavicle displaced inferiorly with communition at fracture site and medial fragment displaced superiorly. Acromion process was displaced slightly infero-posteriorly opening AC joint (Fig 2,3,4)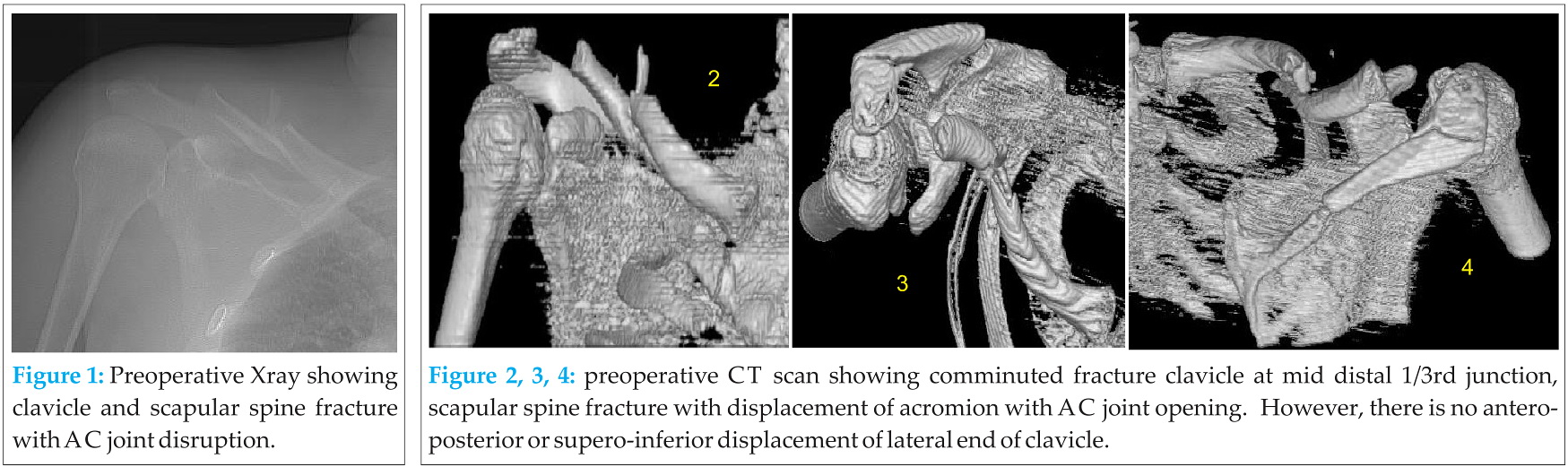
Patient was admitted and was planned for surgery once swelling and ecchymosis was reduced. Patient was explained regarding need of two surgical procedures seperately for clavicle and scapular spine due to need of two different positions, supine for clavicle and prone for scapular spine. In first surgery,open reduction and internal fixation of clavicle was performed in supine position with small sand bag under shoulder. 8 cm incision along the anterior border of midclavicle was made. Fracture site was exposed and we found deltoid muscle interposition in between fracture fragments. Comminuted small fracture fragments were anchored to main fragment with thick vicryl. Fixation was done with eight hole 3. 5 titanium plate and was placed anteriorly. AC joint was not opened. Clavicular length seemed to be achieved. Clinically there was no superoinferior displacement of clavicle at AC joint which probably was explained by intact coraco-clavicular(CC) ligament. Second surgery, after an interval of a week, was performed for scapular spine fracture in prone positon. 8cm incision along the spine of scapula was made. Fracture site seemed to be distracted due to shoulder sag. Fracture reduction assistance was done with inward pressure at shoulder. Internal fixation was done with 8 holed 3. 5 recon titanium plate. Intraoperatively under C-arm guidance AC joint appeared to be reduced.
Postoperatively patient was put on arm sling for a week. Patient was started on pendulum exercises on third day postoperatively(after second surgery). Gradual range of movement exercises were started at two weeks and at two months patient was allowed to do light duties. At 3 months, patient was allowed to resume his daily duties and his routine work. Seven months post operatively, patient had good functional out come with near normal range of movements and patient never complained of pain in AC joint. Functional assessment was done with Constant-Murley Clinical Method of Functional Assessment of the Shoulder and it showed a score of 96(out of 100).
Xrays taken at 4, 12 and 24 weeks. At six months, complete radiological union was seen(Fig 5). CT postoperatively showed minimal persistence of AC joint opening(Fig 6,7,8). This could be because of comminution at fracture site at clavicle which could have reduced its length.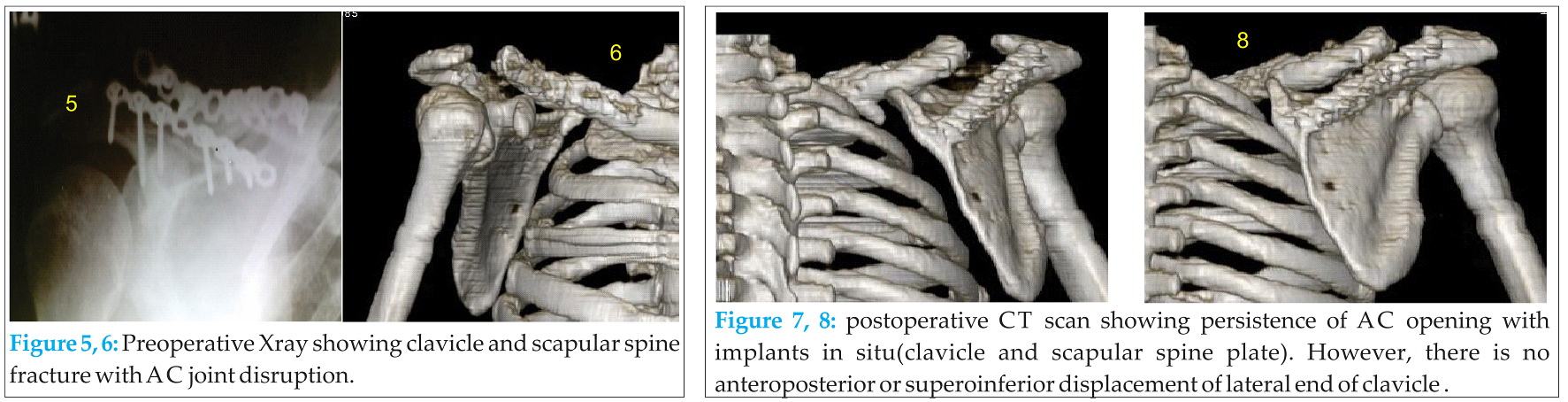
Discussion
Clavicle fractures are one of the most common fractures in Orthopaedics. Most common site of clavicle fracture is middle one-third[5], where the greatest of change in direction of the bone occurs. This results in the sternocleidomastoid muscle lifting the medial aspect superiorly after the fracture and lateral fragment being pulled inferiorly by the weight of arm and also by pull of trapezius and deltoid. This was similar in our case. Lateral fragment was pulled inferiorly and medial fragment superiorly . Scapular fractures, on other hand are relatively uncommon and generally represent 0. 5–1% of all fractures[6] Of these, fractures of the body and neck are the most common and account for more than two-thirds of the cases, with intra-articular fractures of the glenoid cavity (rim and fossa) making up approximately 10%[7]. Fractures of the acromial and coracoid processes account for 9% and 7% respectively, while those of the scapular spine only represent about 6%[8,9]. Mode of injury of clavicular fractures include person falling horizontally on the shoulder or with an outstretched hand. A direct hit to the clavicle will also cause a break[10]. Scapular spine fractures which are very uncommon fractures results from high energy direct trauma[11] . In our patient also, it was a direct injury on the back of shoulder, hit by a heavy four wheeler while walking on the roadside and patient later fell on outstretched hand. This possible mode of injury explains both fractures.
The AC joint is a diarthrodial joint . Along with the sternoclavicular (SC) joint, it provides the upper extremity a connection to the axial skeleton. The AC joint is surrounded by a thin capsule which is rerinforced by four AC ligaments namely anterior, posterior, superior and inferior AC ligaments. AC ligaments are strengthend by muscular attachement of superior AC ligaments to deltoid and trapezius muscle[12]. AC stability is further maintained by the CC ligaments (conoid and trapezoid) in addition to the AC capsule and ligaments. The disruption of this ligament is assessed by measuring interval between clavicle and tip of corocoid process on plain X-ray. Any widening in this distance compared to other side shows that CC ligament has been ruptured. In our case there has not been increase in coraco-clavicular distance.
Rockwood classified AC joint dislocations into six types. Regarding their treatment, most literature has supported conservative management for Rockwood’s grade I and II injuries, whereas there is a general consensus that grade IV, V, and VI injuries are best treated with surgery [13]. The management of grade III injuries, however, remains controversial with proponents for and against surgical treatment. In our case,it did not fit into any particular type of Rockwood’s classification since Xrays and CT evaluation showed opening in AC joint space without migration of lateral end of clavicle anteroposteriorly or supero-inferiorly. This was possibly explained by intact CC ligament and also concomitant fracture in scapular spine due to which acromion process was displaced inferiorly along with lateral end of clavicle(Fig 2,3,4).
Injuries involving lateral end of clavicle with acromioclavicular disruption are common injuries. On the other hand midshaft clavicle fractures with acromioclavicular joint(AC) disruption are relatively rare and have been described only few times[2,3,4]. Furtheremore mid shaft clavicle fracture with acromioclavicular joint disruption in association with scapular spine fracture has never been documented in English literature. Midshaft clavicular fractures with AC joint disruption, which have been described only few times on literature have been managed surgically. In such cases,AC joint have been stabilized either by transfixation with Stienmann pin or Kirschner-wire or reconstruction of CC ligaments or CC screw fixation, after been found that AC joint is still unstable after clavicle plating[2,3,4,14]. In our case, AC joint appeared stable after clavicular fixation without supero-inferior displacement which was probably due to intact CC ligament and hence, no attempt was made to fix AC joint. In acromion fractures, with fractures distal to the acromial angle can be successfully treated with K- wire and tension-band wiring. On the other hand, it is more appropriate to use plate fixation for more proximal and medially displaced fractures involving the spine[15]. Similarly, we used 3. 5 titanium recon plate fixation for scapular spine fracture fixation as a second procedure after fixation of clavicle with similar plate. However, postoperative CT scan revealed persistence in AC joint opening(Fig 6,7,8). This could have been because of comminution at clavicular fracture which could have reduced its length. We did not open AC joint in any stage of surgery. However, functional assessment with Constant-Murley clinical method of functional assessment of the shoulder revealed score of 96(out of 100) with no pain at AC joint.
Conclusion
Ipsilateral clavicle fracture with scapular spine fracture with acromioclavicular disruption is one of the rarest injury. But when managed properly, with proper preoperative planning, staged procedures and strict physiotherapy protocol, its possible to achieve good functional outcome.
Clinical
This case report highlights on rare nature of shoulder injury which has not been described so far. The difficulty in management of ipsilateral clavicle with scapular spine and acromioclavicular joint disruption include the need of staged procedures due to two different operative position requirement. This case report also signifies importance of strict postoperative physiotherapy protocol to avoid stiffness at shoulder to achieve good functional outcome.
References
1. Neer CS. , II Fractures of the distal third of the clavicle. Clin Orthop Relat Res. 1968;58:43–50. [PubMed]
2. Heinz WM, Misamore GW. Mid-shaft fracture of the clavicle with grade III acromio clavicular separation. J Shoulder Elbow Surg. 1995;4:141–2. [PubMed]
3. Wurtz LD, Lyons FA, Rockwood CA. Fracture of the middle third of the clavicle and dislocation of the acromioclavicular joint. A report of four cases. J Bone Joint Surg Am. 1992;74:133–7. [PubMed]
4. Yeh PC, Miller SR, Cunningham JG, Sethi PM. Midshaft clavicle fracture and acromioclavicular dislocation: a case report of a rare injury. J Shoulder Elbow Surg. 2009;18(5):e1–4. [PubMed] . Int J Shoulder Surg. 2008 Jul-Sep; 2(3): 64–67.
5. Kyle J. Jeray. Acute Midshaft Clavicular Fracture. J Am Acad Orthop Surg April 2007 vol. 15 no. 4 239-248
6. Hardegger FH, Simpson LA, Weber BG. The operative treatment of scapular fractures. J Bone Joint Surg Br. 1984;66:725–9. [PubMed]
7. Goss TP. Fractures of the glenoid cavity. J Bone Joint Surg Am. 1992;74:299–305. [PubMed]
8. Armstrong CP, Van der Spuy. The fractured scapula: Importance and management based on a series of 62 patients. Injury. 1984;15:324–9. [PubMed]
9. Kuhn JE, Blasier RB, Carpenter JE. Fractures of the acromion: A proposed classification system. J Orthop Trauma. 1994;8:6–13. [PubMed]
10. Stanley D1, Trowbridge EA, Norris SH. The mechanism of clavicular fracture. A clinical and biomechanical analysis. J Bone Joint Surg Br. 1988 May;70(3):461-4
11. Ada JR, Miller ME. Scapular fractures: Analysis of 113 cases. Clin Orthop Relat Res. 1991;269:174–80. [PubMed]
12. Rockwood CA, Jr, Young DC. Disorders of the acromioclavicular joint. In: Rockwood CA Jr, Matsen FA, editors. The shoulder. Philadelphia: WB Saunders; 1990. pp. 413–76
13. Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separations: useful and practical classification for treatment. Clin Orthop Relat Res. 1963;28:111–9. [PubMed]
14. Spyridon A. Psarakis, Olga D. Savvidou, Sofia M. Voyaki, Michail Beltsios, and John N. Kouvaras. A rare injury of ipsilateral mid-third clavicle fracture with acromioclavicular joint dislocation. Hand (N Y). Jun 2011; 6(2): 228–232.
15. Ogawa K, Naniwa T. Fractures of the acromion and the lateral scapular spine. J Shoulder Elbow Surg. 1997;6:544–8. [PubMed]
| How to Cite This Article: Kembhavi RS, James B. Ipsilateral Closed Clavicle and Scapular Spine Fracture with Acromioclavicular Joint Disruption. Journal of Orthopaedic Case Reports 2015 April-June;5(2): 58-61. Available from: https://www.jocr.co.in/wp/2015/04/20/2250-0685-276-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


