
[box type=”bio”] What to Learn from this Article?[/box]
Tumours have varied presentations.Patellar tumours although rare should be considered as a differential diagnosis in patellar pathologies presenting with knee pain.
Case Report | Volume 5 | Issue 3 | JOCR July-Sep 2015 | Page 72-74 | Abhinav S. Bhatnagar, Kaushal Malhan, Sonu Mehta. DOI: 10.13107/jocr.2250-0685.314.
Authors: Abhinav S. Bhatnagar[1], Kaushal Malhan[1], Sonu Mehta[1].
[1] Department of Orthopaedics, Fortis Hospital, Mumbai. Maharashtra. India.
Address of Correspondence
Dr. Abhinav S. Bhatnagar,
C/O Fortis Hospital,Mulund (w),Mumbai-78. Maharashtra. India.
E-mail: b_abhinav@hotmail.com
Abstract
Introduction: Osteochondroma (OC) is the most common benign tumor of the skeleton. However, patellar OC is very rare. Only five case reports have been published yet and only 1 after the year 1972. OCs grow during childhood through adolescence, but usually growing ends when the epiphyseal plates close. In an adult, the growth of an OC suggests the diagnosis of malignant transformation to a chondrosarcoma. However, enlargement of a patellar OC reported as benign after skeletal maturity is present in literature.
Case Report: CWe report the clinical and radiologic findings of a patellar OC in a 50-year-old female, with a 3-year progression of swelling, not painful, well-defined margins, normal skin, and no neurovascular deficits or functional impairment. The tumor was surgically resected, and histopathological examination did not show malignancy. After 2 years of follow-up, the patient has no complaints and no signs of recurrence.
Conclusion: Patellar OCsare extremely rare with only a few reports published. It should be kept in mind that benign OCs can show symptomatic growth in skeletally mature patients without malignant transformation.
Keywords: Patella, osteochondroma, benign.
Introduction
Osteochondroma (OC) is the most common bone tumor, which constitutes 20-50% of all benign bone tumors [1]. WHO 2002 defined OC as a cartilage capped bony projection arising from the external surface of bone containing a marrow cavity that is continuous with that of the underlying bone [2]. Malignant transformation of OCs can occur later in adulthood but rarely metastasize. Primary tumors of the patella account for <0.06% of bone tumors [3]. Patellar OC is a very rare entity. Only five case reports have been published yet and only 1 after the year 1972. The purpose of our study was to report a rare case of patellar OC, its course of progression, and management.
Case Report
The patient was a 50-year-old female. She reported that around 5 years earlier, she had noted a painless swelling in her left knee that gradually progressed from approximate size of 2 cm × 2 cm to the current size in a span of 3 years, when she first reported to our hospital. On physical examination, it was a non-tender bony swelling with well-defined margins, lobulated surface, measuring 15 cm × 8 cm × 10 cm (Fig. 1), adhered to the patella. It moved together with the patella when flexion-extension knee movements were made. There was no neurovascular deficit, and the range of motion of the knee was not impaired.
In the radiological evaluation, tumor with bone density in the lower center of the patella of the left knee was shown. The tumor appears to be continuous with the patella. Flecks of calcification were seen in the tumor. Computed tomography (CT) scan confirmed the continuity of the mass with patella and magnetic resonance imaging (MRI) was helpful in confirming its benign nature (Figs. 2 and 3).  The diagnosis of patellar OC was made, and surgical resection was planned because of the tumor growth.
The diagnosis of patellar OC was made, and surgical resection was planned because of the tumor growth.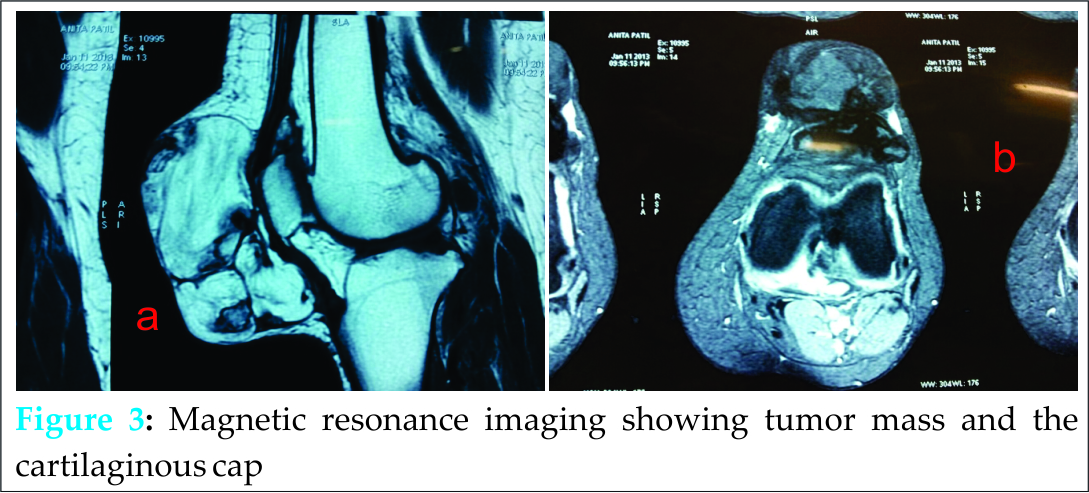 During the operation, we observed that there was a bone lesion arising from the patella, surrounded by a cartilaginous coating, and simple resection of the tumor was performed (Figs. 4 and 5).
During the operation, we observed that there was a bone lesion arising from the patella, surrounded by a cartilaginous coating, and simple resection of the tumor was performed (Figs. 4 and 5).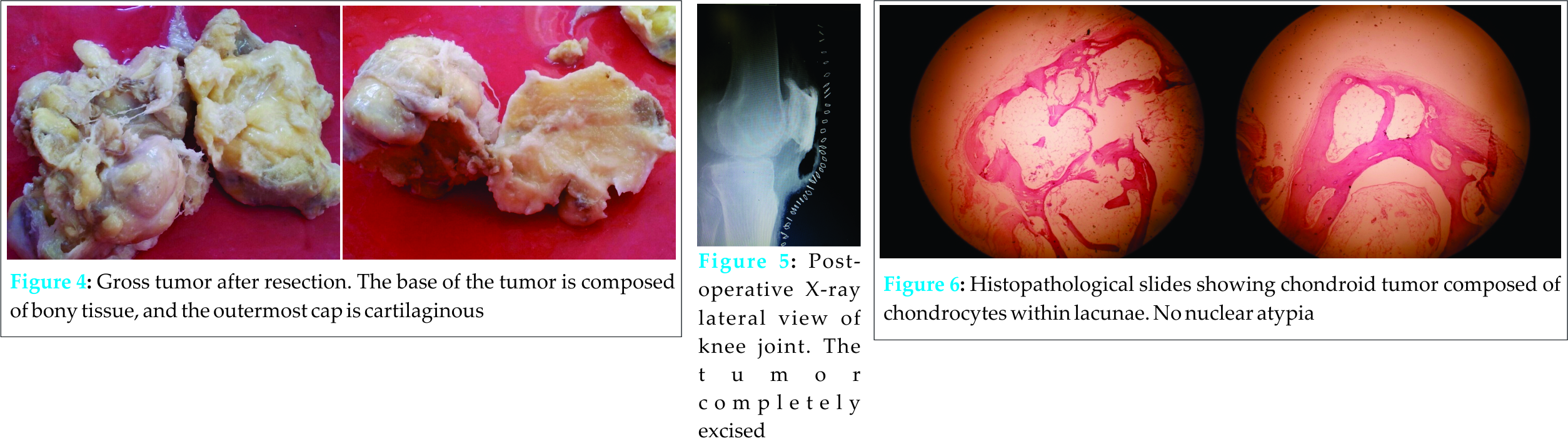 The tumor mass was sent for histopathological examination, and the diagnosis of patellar OC without signs of malignant transformation was confirmed (Figs. 6). Over the course of the 2-year follow-up since surgery, the patient did not present with any symptoms and signs of recurrence.
The tumor mass was sent for histopathological examination, and the diagnosis of patellar OC without signs of malignant transformation was confirmed (Figs. 6). Over the course of the 2-year follow-up since surgery, the patient did not present with any symptoms and signs of recurrence.
Discussion
Skeletal OCs or osteocartilaginous exostoses constitute 10-15% of all bone tumors [1]. OCs are solitary or multiple, pedunculated or sessile exophytic outgrowths from the bone surface that are composed of cortical and medullary bone with an overlying hyaline cartilage cap. Marrow and cortical continuity with the underlying parent bone defines the lesion [4,5]. OC arise in any bone that develops from endochondral ossification [4,5]. However, patella develops through membranous ossification, and an OS arising from patella as in our case is a rare occurrence. Solitary skeletal OCs are usually located in the metaphyses of the long bones, extending away from the adjacent joint, forming the typical pattern of stalactites and stalagmites. The long bones of the lower extremities are most frequently involved [4,6-8]; the knee (40%) [6,7] followed by the humerus (10-20%) [6,8] are more frequently involved. Other more unusual locations include the small bones of the hands and feet (10%), scapula (4%), pelvis (5%), and cranial base and jaw [6]; the spine is affected in 1.3-4.1% of cases. However, patellar OC, as reported in our study, is a very rare entity with only five reported cases yet. The vast majority of solitary OCs are asymptomatic and diagnosed incidentally [7,8]. Clinical symptoms may be related to mechanical effects, cosmetic deformity, neurovascular impingement, pseudoaneurysm formation, fracture, overlying bursa formation, or malignant transformation. Painless swelling and cosmetic deformities related to the slowly enlarging mass are the most common complaints [9,10], which were similar to the complaints our patient reported with. In adults, growth or imaging alterations of an OC suggest the rare diagnosis of malignant transformation; however, extensive growth of OCs without histological evidence of malignancy has been reported [11,12]. In our case too, although there was the extensive growth of tumor clinically, radiologically, and histologically, the benign nature of the tumor was confirmed. Although radiography is often diagnostic alone, other imaging modalities may be necessary for surgical planning and to exclude sarcomatous degeneration. The areas of osseous continuity between parent bone and OC may be broad (sessile OC) or narrow (pedunculated OC). Pedunculated lesions usually point away from the nearest joint owing to the forces of the overlying tendons and ligaments forming the stalactites and stalagmites [13]. CT scanning using three-dimensional imaging reformation allows optimal depiction of the pathognomonic cortical and marrow continuity of the lesion and parent bone, especially for OCs in complex areas of the anatomy [14,15]. MRI is the best imaging modality for evaluating cortical and medullary continuity between OC and parent bone. MRI may be the optimal method for evaluating the cartilaginous cap and identify lesions suspicious for malignant transformation [16]. CT and MRI both were done for our case to confirm the diagnosis. Malignant transformation is seen in <0.4-2.2% of patients of solitary OC and up to 27% of patients with multiple hereditary exostoses. Clinical features suspicious for malignant transformation comprise new onset of pain in a previously stable lesion, rapid or new growth, growth after skeletal maturity, and/or large lesions [17-19]. There were no signs of malignant transformation of the tumor in our patient, and the duration of 3 years that the tumor took to reach the size presented was also indicative of its benign nature that was further confirmed on histopathological findings.
Surgery to resect the tumor is not essential in all cases. Its main indications are when the exostosis is interfering with the growth of the extremity, which leads to functional and mechanical alterations; in the presence of malignant transformation, which is characterized by a thick coating of more than 2 cm in adults; and in the presence of bone erosion, vascular compression and/or nerve compression with symptoms and joint locking promoted by the OC. The relative indications are esthetic complications, which often give rise to post-operative skin scarring that is worse than the esthetic deformity itself; and pain, which may occur because of bursitis or after fracturing, depending on the patient’s symptoms [19]. In our patient, since patient only had an esthetic problem and tumor being of benign nature, we only resected the tumor, with no complications and recurrence in 2 years of follow-up.
Conclusion
Ocs although arise in bones developing through endochondral ossification, its growth on the patella (membranous ossification) makes it a rare occurrence. Furthermore, the growth of the tumor in spite of its benign nature after skeletal maturity differs from its usual presentation.
Clinical Message
This case report is yet another example to show that tumors can present with varied presentations and locations. Patellar tumors, though rare should always be considered in differential diagnosis of patellar pathology.
Reference
.
| How to Cite This Article: Bhatnagar AS, Malhan K, Mehta S. A rare case report of Patellar Osteochondroma. Journal of Orthopaedic Case Reports 2015 July – Sep;5(3):72-74 . Available from: https://www.jocr.co.in/wp/2015/07/10/2250-0685-314-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


