
[box type=”bio”] What to Learn from this Article?[/box]
The case report aims at recognition of acute traumatic ulnar nerve subluxation, a rare entity and briefly highlights its diagnosis and management.
Case Report | Volume 5 | Issue 4 | JOCR Oct-Dec 2015 | Page 47-49| Sangeet Gangadharan, Padma Shetty. DOI: 10.13107/jocr.2250-0685.344 .
Authors: Sangeet Gangadharan[1], Padma Shetty[2]
[1] Department of Orthopaedicss, Gulf Medical College hospital, Ajman, UAE.
[2] General practitioner, Gulf Medical College hospital, Ajman, UAE
Address of Correspondence
Dr. Sangeet Gangadharan
403, D-16, Shanti Vihar, Mira Road, Thane 401107, Maharashtra
E mail – drsangeetgangadharan@gmail.com
Abstract
Introduction: Acute traumatic subluxation of the ulnar nerve at the cubital tunnel is rare or under-reported
Case Report: A 31 year old Asian man presented with severe, radiating pain from the elbow to forearm, following a fall on his outstretched hand. He had swelling and severe tenderness at the posteromedial aspect of the elbow. Pain aggravated with elbow flexion beyond 80 degrees.
There was no neurological deficit. Dynamic ultrasound demonstrated subluxation of ulnar nerve with elbow flexion. Broad arm sling immobilization was given for three weeks. At final follow up, he was asymptomatic with full range of pain free motion at the elbow.
Conclusion: Our case report summarizes the presentation, management and pathomechanism of a rare clinical entity.
Keywords: acute ulnar nerve subluxation, cubital tunnel, Osborne’s ligament.
Introduction
Ulnar nerve, being in close proximity to the elbow joint is predisposed to trauma and entrapment neuropathy where it courses through the cubital tunnel. Subluxation or dislocation of the nerve at this site could occur as a result of trauma or variations in the anatomical structures posterior to elbow joint. While recurrent or chronic subluxation of ulnar nerve has been commonly reported, acute traumatic subluxation is rare or under-reported.
Case report
A 31 year old, obese businessman presented to the emergency with complaints of severe pain in the left elbow, radiating to the forearm. He also had pain and swelling of the left ankle. His left foot turned inwards and he sustained a fall onto his left hand with the elbow bent. Immediately after the fall, he experienced an electric shock like sensation which radiated along the inner aspect of the forearm. Clinically, there was swelling around postero-medial aspect of left elbow. Tenderness was elicited in the posterior aspect of the medial epicondyle. He experienced severe radiating pain along ulnar nerve distribution whenever the elbow was flexed beyond 80 degrees. Valgus stress test of elbow was negative. There was no sensory or motor deficit along ulnar nerve distribution. A medial epicondyle fracture was suspected. Orthogonal views of the elbow did not reveal any fracture or abnormality of medial epicondyle. Traumatic subluxation of ulnar nerve was thus suspected. Dynamic ultrasound of the elbow revealed subluxation of the ulnar nerve as evidenced by increased distance between the floor of the cubital tunnel and the nerve, in comparison to the opposite elbow. It stayed in close proximity to the tip of the medial epicondyle. The nerve was found to subluxate from the cubital tunnel with elbow flexion beyond 90 degrees. Elbow effusion was present. Fig. 1.( Ultrasound image of posterior elbow)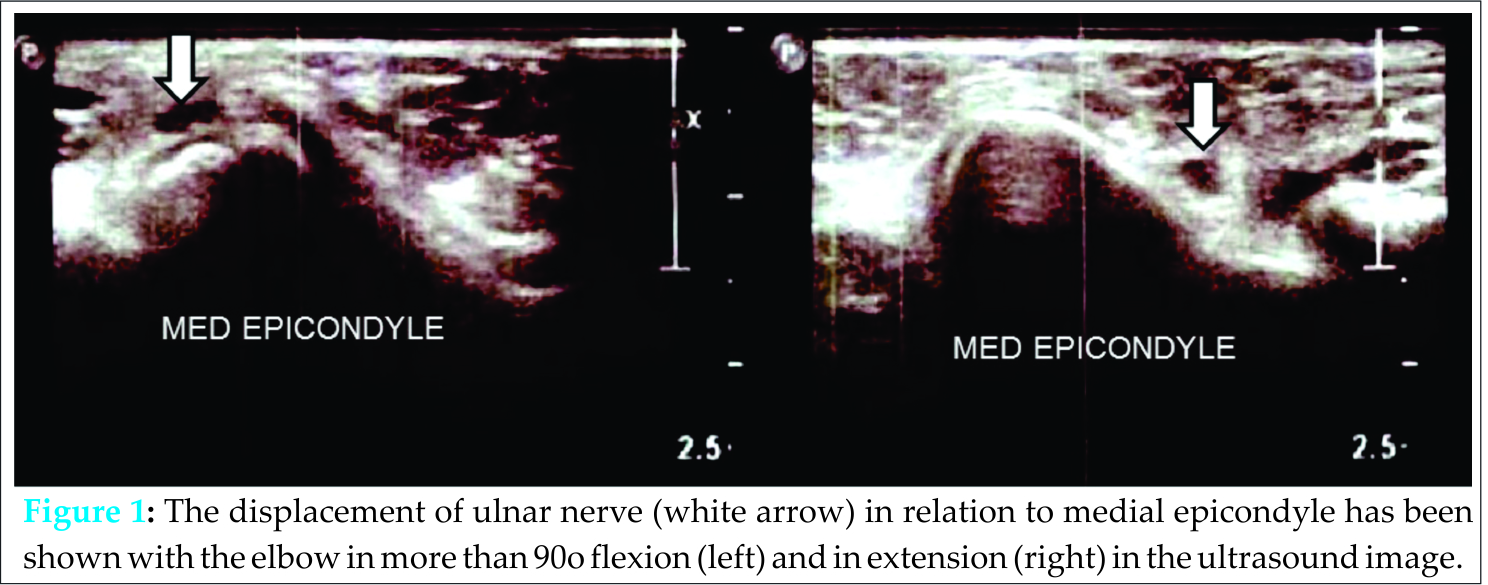
The arm was rested in a broad arm sling for three weeks in 45 degrees flexion, a position in which he had no pain. He also had a grade I/II lateral collateral ligament sprain of the ipsilateral ankle which was treated by below knee cast.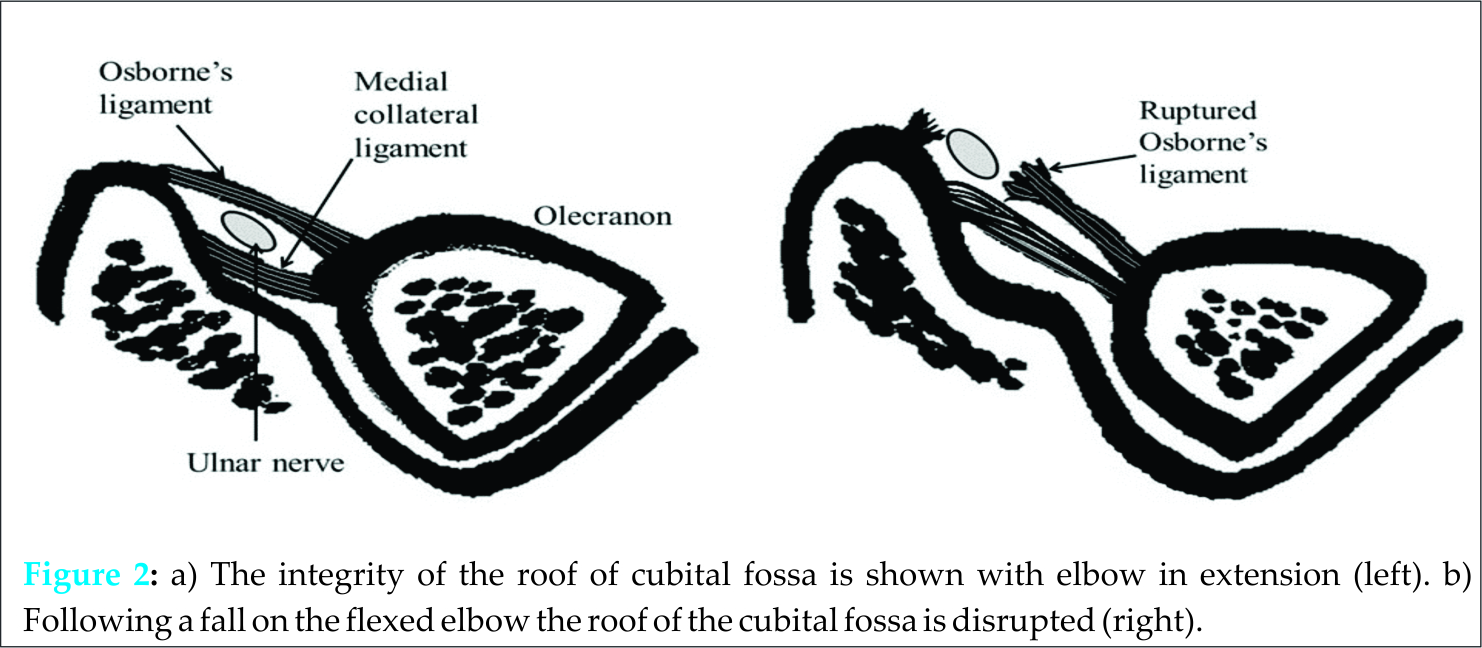
At three weeks follow up, the patient had no pain but a fixed flexion deformity of 15 degrees at the elbow. He was advised active range of motion exercises and the sling was discontinued. At final follow up, one year after the injury, patient was asymptomatic and had full range of pain free motion at the elbow and with no neurological deficit in the upper limb.
Discussion
Ulnar nerve subluxation was first reported by Blattmann in 1851 [1] Knowledge of the pathoanatomy and dynamic relationship of the ulnar nerve in cubital tunnel is crucial in understanding this pathology. At the elbow, the ulnar nerve lies in the cubital tunnel; the posterior wall of which is formed proximally by the fascial aponeurosis between the two heads of flexor carpi ulnaris and distally by its muscle belly. This aponeurosis blends with the arcuate ligament of Osborne [2]. Childress, in his study of 1000 patients found ulnar neuritis in 21% of those with ulnar nerve subluxation. Recurrent ulnar nerve subluxation has been associated with laxity of the cubital tunnel roof, congenital hypoplasia of medial epicondyle, variations in muscular anatomy or post-traumatic changes [3-8]. Richard MJ et al found various muscular anomalies in his retrospective review of 18 elbows [9]. Dellon noted large medial head of triceps extending into the floor of cubital tunnel in 28% of cadavers, 77% of which had demonstrable subluxation of ulnar nerve [10]. Friction neuritis explains ulnar nerve symptoms in recurrent ulnar nerve subluxation [6].
However acute traumatic ulnar nerve subluxation still remains a poorly understood clinical entity due to scarcity of data. There are a very few reports worldwide and a single report in English literature on acute traumatic subluxation of ulnar nerve.
We propose a possible explanation of the mechanism of traumatic ulnar nerve subluxation in our patient. The patient fell onto his non-dominant hand with the elbow in flexion. Flexion at the elbow stretches the Osborne’s ligament [6]. A sudden upward thrust on the flexed elbow will further stress this ligament and cause tear. This renders the ulnar nerve susceptible to subluxation or dislocation. With elbow flexion beyond 90 degrees, the strain on ulnar nerve increases and it tends to translate anteriorly over the medial epicondyle as shown in Fig. 2 (Diagram showing transverse section of the elbow at the cubital fossa.) [11, 12]. In the absence of an intact Osborne’s ligament, the ulnar nerve is vulnerable to subluxation or dislocation. This could explain reproduction of symptoms of ulnar neuropathy with increasing elbow flexion. We believe that splinting the elbow for three weeks, in our patient lead to healing of Osborne’s ligament which thereby prevented nerve subluxation thereafter.
Ultrasound is a useful tool in diagnosis of ulnar nerve subluxation as it detects real time translation of the nerve with changing elbow flexion [12]. Though the ulnar nerve was found subluxated in our patient, tear in Osborne’s ligament couldn’t be well visualized. An MRI of the elbow can detect tear in the Osborne’s ligament and also assess integrity of medial collateral ligament at the same time.
There is no consensus or evidence for the best treatment for chronic or recurrent ulnar nerve subluxation and data for traumatic nerve subluxation is scarce. Patients with persistent symptoms or painful snapping or those refractory to conservative line of management could be considered for surgery [11]. Various modes of treatment have been suggested in the management of recurrent ulnar nerve subluxation. Few authors have suggested conservative line of management in the form of splinting or physiotherapy initially followed by surgical treatment if the former fails. Splinting the elbow in 30-45 degrees of flexion has been recommended in various studies [2]. Our patient was treated by splinting in 50 degrees flexion followed by range of motion exercises. He showed resolution of symptoms at three weeks. Splinting relieves traction neuritis as well as reduces the inflammation in the cubital fossa. We believe that splinting followed by physiotherapy restores the integrity of the roof of cubital tunnel.
Conclusion
Acute ulnar nerve subluxation is a rare clinical entity. Diagnosis can be confirmed by dynamic ultrasonography. In the absence of neurological deficit, it can be managed conservatively by splinting the elbow in mid-flexion.
Clinical Message
Electric shock like pain in the elbow, following trauma which aggravates with flexion should suggest possibility of acute ulnar nerve subluxation. Failure to recognize this injury and avoiding splinting may lead to recurrent subluxation of the nerve.
References
1. Blattman A: Habitual luxation of the ulnar nerve. Deutsche Klinic 1851; 435.
2. Robertson C, Saratsiotis J. A Review of Compressive Ulnar Neuropathy at the Elbow. J Manipulative Physiol Ther. 2005;28(5):345.
3. Childress HM. Recurrent ulnar-nerve dislocation at the elbow. J Bone Joint Surg Am. 1956;38-A(5):978–84.
4. Lazaro L. Ulnar nerve instability: ulnar nerve injury due to elbow flexion. South Med J. 1977;70(1):36–40.
5. Rayan GM. Recurrent anterior dislocation of the ulnar nerve at the cubital tunnel. Plast Reconstr Surg. 1990;86(4):773–5.
6. Childress HM. Recurrent ulnar-nerve dislocation at the elbow. Clin Orthop. 1975;(108):168–73.
7. Pike J, Goetz T. Traumatic transposition of the ulnar nerve in a patient with posteromedial varus rotatory instability of the elbow: a case report. J Shoulder Elb Surg Am Shoulder Elb Surg Al. 2008;17(1):e5–8.
8. Spinner RJ, O’Driscoll SW, Davids JR, Goldner RD. Cubitus varus associated with dislocation of both the medial portion of the triceps and the ulnar nerve. J Hand Surg. 1999;24(4):718–26.
9. Richard MJ, Messmer C, Wray WH, Garrigues GE, Goldner RD, Ruch DS. Management of Subluxating Ulnar Nerve at the Elbow. Orthopedics [Internet]. 2010 Sep 7 [cited 2014 Sep 23]; Available from: http://www.slackinc.com/doi/resolver.asp?doi=10.3928/01477447-20100722-04
10. Dellon AL. Musculotendinous variations about the medial humeral epicondyle. J Hand Surg Edinb Scotl. 1986;11(2):175–81.
11. Xarchas KC, Psillakis I, Koukou O, Kazakos KJ, Ververidis A, Verettas DA. Ulnar nerve dislocation at the elbow: review of the literature and report of three cases. Open Orthop J. 2007;1:1.
12. Grechenig W, Clement H, Mayr J, Peicha G.. Ultrasound detection of dislocation of the ulnar nerve from the sulcus of the elbow joint. Praxis. 2003; 92(24):1129–32.
| How to Cite This Article: Gangadharan S, Shetty P.Acute Traumatic Ulnar Nerve Subluxation: A Case Report and Pathomechanism. Journal of Orthopaedic Case Reports 2015 Oct-Dec;5(4): 47-49. Available from: https://www.jocr.co.in/wp/2015/10/01/2250-0685-344-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


