
[box type=”bio”] What to Learn from this Article?[/box]
Calcaneal osteochondroma growth in adults can be a differential diagnosis for retrocalcaneal bursitis, which can be optimally treated by excision.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 16-19| Rupesh Kumar, Anjana, Meghraj Kundan DOI: 10.13107/jocr.2250-0685.410
Authors: Rupesh Kumar[1], Anjana[2], Meghraj Kundan[3]
[1] Department of Orthopedics, IQ city Medical College, Durga pur, West Bengal. India.
[2] Department of Pathology, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand. India.
[3] Department of Orthopedics, V.M Medical College and safdarjung hospital, New Delhi. India.
Address of Correspondence
Dr. Rupesh Kumar, Road no 2 Shant Man Nagar, Imam Kothi, Deepatoli, Ranchi-834009. India.
E-mail: rupesh.rajesh@yahoo.co.in
Abstract
Introduction: Osteochondroma is the most common benign tumour of the bone and is considered as developmental lesion of the bone. Common site of osteochondroma presentation is around the knee but calcaneal osteochondroma as such is a rare entity. Osteochondromas grow during childhood through adolescence, but usually the growth of osteochondroma ends when the epiphyseal plates close. In an adult, growth of an osteochondroma suggests the diagnosis of a malignant transformation. However, it can also present as pressure symptom in later phase of life. Here, we presented a case of retrocalcaneal bursitis in late phase of life of a male farmer due to late growth of osteochondroma.
Case Presentation: We report a case of calcaneal osteochondroma which is an extremely rare site of occurrence with painful swelling of ankle causing limitation of walking in a 58-year-old male. Surgical excision of tumour followed by a histological confirmation reported negative for any malignant changes.
Conclusion: There may be chances of osteochondroma being a reason for retrocalcaneal bursitis. It is possible of late detection of benign osteochondromas which show symptomatic growth and pressure effect in skeletally mature patients without malignant transformation.
Key word: calcaneus, osteochondroma, retrocalcaneal bursitis.
Introduction
Osteochondroma is the most common benign tumour of the bone which is better known as skeletal developmental lesion. It usually arises from the metaphyseal or metadiaphyseal region of long bones of the appendicular skeleton and are most commonly seen around the knee [1, 2]. Osteochondromas grow during childhood through adolescence, but usuallytheir growth ends when the epiphyseal plates close [1, 3]. They are typically described in patients younger than 20 year-old and extensive osteochondroma growth into adulthood is rarely reported [3, 4]. In an adult, growth of an osteochondroma suggests the diagnosis of malignant transformation to a chondrosarcoma [3, 5]. However, Krieg et al [6] and Nogier et al [3] reported extensive growth of an osteochondroma in a skeletally mature patient whose tumour had no evidence of malignancy in histological examination. Osteochondromas are uncommon in the foot and ankle. Calcaneus is one of the most unusual region for an osteochondroma. In this study, we describe the clinical presentation of calcaneal osteochondroma with retrocalcaneal bursitis in a skeletally mature male.
Case presentation
A 58-year-old male patient who belongs to Jharkhand was admitted to our hospital with painful swelling and stiffness in his right ankle. The swelling was present in a smaller form for many years but past three to four years there was progressive swelling at the back of ankle joint and now he was unable to walk properly. He was not able to walk more than 200-300 metre at a stretch. He is farmer by profession. He ignored the symptoms many a times, and had been taking analgesics as prescribed by the local doctor but was never investigated properly before except an X-ray of ankle joint. Since last two weeks, the pain had increased tremendously without any precipitating reason along with inflammatory sign over the ankle joint. At the time of presentation, pain was severe and he was unable to stand, and there was enough pain at rest also. No family history of such type of condition was noted. No past history of trauma or any other illness which can affect its course was observed. 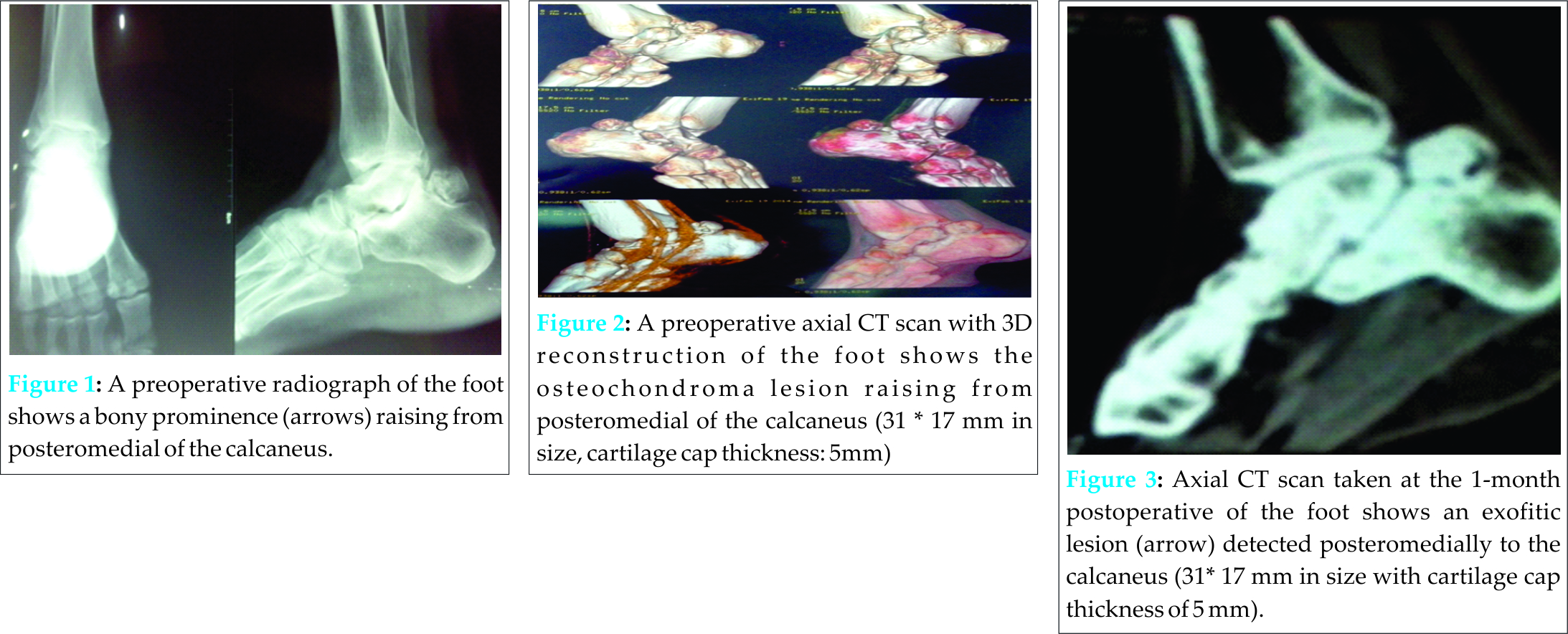
On physical examination, about 3.5 × 2 cm stiff, immobile, painful mass placed between tendoachilis and plafond of tibia was palpated. Mass was tender, fixed with calcaneus , boggy swelling. Skin over swelling showed features of inflammation. Movements at the ankle were severely compromised. Knee joint was clinically normal. Clinical features and X-ray picture suggested metastatic calcification, ostrigonous or osteochondroma. The antero-posterior and lateral view plain X-ray radiography and plane computed tomography (CT) revealed a bony prominence 31 × 17 mm (cartilage cap thickness: 5 mm app) in size raising from superior part of the calcaneus near posterior margin of talo calcaneus joint and reported as a higher possibility of an osteochondroma (Fig. 1, 2, 3). However, features suggestive of malignancy were not seen. Ankle and other joints of foot were normal except for inflammatory reactive effusion. In addition, retrocalcanealbursitis features were observed. As the pain was of moderate to severe grade and caused major limitation in activities of daily living, it was decided to excise the osseous mass. 
Complete surgical excision of the bony mass was planned. Intraoperatively, it was observed that the lesion rose from the posteromedial side of the calcaneus and grew through the surface pushing the soft tissues more posteromedially. Posterolateral approach chosen as it was safer and mass was pushing all the soft tissue on lateral side and it was easy to remove adhesion on posterolateral approach. The bony mass was excised as much as possible from its attachment to calcaneus; stalk was not differentiated as this was very compressed. Bony material along with soft tissue was sent for pathologic examination, inflamed bursa was also removed. Histopathological examination of the bony mass reported it as osteochondroma (cartilage cap 4mm) but there was no evidence of malignancy. Report was re-evaluated and confirmed by another histopathologist. Intraoperative and post operative period was uneventful. After surgery, patient was put on below knee slab which was removed after 21 days to get adequate soft tissue healing. Wound healed well. At 6 months follow up, there was no recurrence of lesion and patient was comfortably walking without pain. Currently, the patient is asymptomatic and has no pain, but there is limitation of motion at the ankle joint.
Discussion
Osteochondromas are developmental lesions rather than true neoplasms and they may occur solitary or as multiple lesions, associated with the syndrome multiple hereditary exostoses [1]. Osteochondroma is seen in 2% to 3% of the general population and represents approximately 36% to 41% of benign bone tumours [7, 8]. The hand and feet bones, including the calcaneus comprise only 10% of osteochondromas [3].
The evaluation of osteochondromas can generally help clinical findings, and imaging methods such as plain radiography, ultrasonography, CT, MR imaging and bone scanning [1, 3]. Osteochondromas are usually asymptomatic, and are seen incidentally on radiography [3]. The most common symptom is a non-tender, painless cosmetic deformity secondary to the slowly enlarging exophytic mass. Additional complications that cause symptoms include osseous deformity, fracture, vascular-nerve compression, neurologic sequelae, bursa formation, and malignant transformation [3, 7]. Malignant transformation is seen in less than 1% to 2% of patients of solitary osteochondroma [2, 9] and in 5%-25% of patients with multiple hereditary exostoses [1, 2, 10].
Clinical features suspicious for malignant transformation comprise new onset of pain in a previously stable lesion, rapid or new growth, growth after skeletal maturity, and/or large lesions [2, 11]. These lesions are usually a low-grade chondrosarcoma or less often a secondary osteosarcoma [12, 13]. In our case, the first complaint was pain that was progressively increasing with limitation of movement. Although, radiography alone is often diagnostic, other imaging modalities may be necessary for surgical planning and to exclude sarcomatous degeneration. The radiographic appearance of this tumour is often diagnostic and reflects its pathologic characteristics. The lesion is composed of native cortical and medullar bone protruding from and continuous with the underlying bone and they appear as sessile or pedunculated [1, 2]. However, if there is no extensive mineralization, the thickness of the cartilage cap is usually not well evaluated with radiography [1]. In our case, because of the unusual posteroinferior placement to calcaneus, AP and lateral radiographies did not reveal a satisfactory view. Ultrasonography can be used in the measurement of the hyaline cartilage cap thickness [14, 15]. However, it is an operator-dependent examination with often limited value in obese patients and lack of evaluation of the osseous components of the lesion [1]. Bone scanning is directly correlated with the degree of enchondral bone formation [16, 17]. MR imaging is the best radiologic imaging method evaluating hyaline cartilage cap. It also important for visualizing the effect of the lesion on surrounding structures and shows cortical and medullary continuity between the parent bone and osteochondroma.
Multiplanar reconstruction and three-dimensional imaging features of CT give important information about determining these lesions. It allows optimal demonstration of the pathognomonic cortical and medullary continuity of the lesion and parent bone as in our case. Murphey et al [1] believed that very thin sections available with CT are often superior to MR imaging, especially in complex areas of anatomy, in osteochondroma cases. Mineralization in the cartilage cap allows a correct CT measurement. However, it can be very difficult to correctly measure the thickness of a totally nonmineralized cartilage cap because it cannot be easily differentiated from surrounding muscle or bursa. Cartilage cap thickness greater than 1 to 2 cm in adults and 2 to 3 cm in growing children suggests malignant transformation [1, 2].
The treatment of osteochondromas in the foot is conservative or surgical (excision). Stable, small asymptomatic lesions can be treated conservatively. If the lesion is painful and growing after skeletal maturity and exhibits signs of malignant transformation, it should be treated surgically. A marginal resection is adequate and shows a low rate of recurrence. Any remaining cartilage cap may result in recurrence, especially in growing lesions [1].
In our case, osteochondroma was slowly growing in size, there was only minimal increase in size of swelling in due course of time. But there was progressive increase in intensity of pain as well limitation of movement at ankle joint radiograph and CT scan showing osteochondroma with cartilage cap but there was no obvious sign of any malignancy. Feature of retrocalcaneal bursitis was increasing and causing hindrance to normal walking. Therefore, it was decided to surgically excise the osseous mass. Later it was confirmed with histopathological examination for malignancy.
Conclusion
In conclusion, we should keep in mind that benign osteochondromas can represent as symptomatic growth in skeletally mature patients even in 5th or 6th decade without a malignant transformation.
Clinical Message
Calcaneal osteochondroma is a rare condition, which can present as retro calcaneal bursitis due to growth without malignant change in late phase of life. Excison of Osseous mass is a treatment option with optimum result.
References
1. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-1434.
2. Blitz NM, Lopez KT. Giant solitary osteochondroma of the inferior medial calcaneal tubercle: a case report and review of the literature. J Foot Ankle Surg 2008;47:206-212.
3. Nogier A, De Pinieux G, Hottya G, Anract P. Case reports: enlargement of a calcaneal osteochondroma after skeletal maturity. ClinOrthopRelat Res 2006; 447:260-266.
4. Greger G, Catanzariti AR. Osteochondroma: review of the literature and case report. J Foot Surg 1992;31:298-300.
5. Garrison RC, Unni KK, McLeod RA, Pritchard DJ, Dahlin DC. Chondrosarcoma arising in osteochondroma. Cancer 1982; 49:1890-1897.
6. Krieg JC, Buckwalter JA, Peterson KK, El-Khoury GY, Robinson RA: Extensive growth of an osteochondroma in a skeletally mature patient: a case report. J Bone Joint Surg 1995;77:269-273.
7. Karasick D, Schweitzer ME, Eschelman DJ. Symptomatic osteochondromas: imaging features. AJR Am J Roentgenol 1997;168:1507-1512.
8. Griffiths HJ, Thompson RC Jr, Galloway HR, Everson LI, Suh JS. Bursitis in association with solitary osteochondromas presenting as mass lesions. Skeletal Radiol 1991;20:513-516.
9. Mehta M, White LM, Knapp T, Kandel RA, Wunder JS, Bell RS. MR imaging of symptomatic osteochondromas with pathological correlation. Skeletal Radiol 1998.27:427-433.
10. Blanton SH, Hogue D, Wagner M, Wells D, Young ID, Hecht JT. Hereditary multiple exostoses: confirmation of linkage to chromosomes 8 and 11. Am J Med Genet 1996;62:150-159.
11. Malik R, Kapoor N, Malik R. Transformation of solitary osteochondromacalcaneum to chondrosarcoma-a case report. Indian J PatholMicrobiol 2004.47:42-43.
12. Van Lerberghe E, Van Damme B, Van Holsbeeck M, Burssens A, Hoogmartens M. Case report 626: osteosarcoma arising in a solitary osteochondroma of the femur. Skeletal Radiol 1990;19:594-597.
13. Nojima T, Yamashiro K, Fujita M, Isu K, Ubayama Y, Yamawaki S. A case of osteosarcoma arising in a solitary osteochondroma. ActaOrthopScand 1991;62:290-292.
14. Malghem J, Vande Berg B, Noel H, Maldague B. Benign osteochondromas and exostoticchondrosarcomas: evaluation of cartilage cap thickness by ultrasound. Skeletal Radiol 1992;21:33-37.
15. Hudson TM, Springfield DS, Spanier SS, Enneking WF, Hamlin DJ. Benign exostoses and exostoticchondrosarcomas: evaluation of cartilage thickness by CT. Radiology 1984;152:595-599.
16. Glassman SB, Delbeke D. Nuclear medicine case of the day: hereditary multiple exostoses. AJR Am J Roentgenol 1992;158:1384.
17. Kobayashi H, Kotoura Y, Hosono M, Sakahara H, Hosono M, Yao ZS, Tsuboyama T, Yamamuro T, Endo K, Konishi J. Diagnostic value of Tc-99m (V) DMSA for chondrogenictumors with positive Tc-99m HMDP uptake on bone scintigraphy. ClinNucl Med 1995;20:361-364.
| How to Cite This Article: Kumar R, Anjana, Kundan M. Retrocalcaneal Bursitis due to Rare Calcaneal Osteochondroma in Adult Male : Excision and Outcome. Journal of Orthopaedic Case Reports 2016 April-June;6(2): 16-19. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-410-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


