
[box type=”bio”] What to Learn from this Article?[/box]
The early diagnosis of Pycnodysostosis (clinical and radiological) allows to avoid the complications that can be debilitating.
Case Report | Volume 6 | Issue 2 | JOCR April-June 2016 | Page 43-45 | Hayat Aynaou, Imane Skiker, Hanane Latrech. DOI: 10.13107/jocr.2250-0685.426
Authors: Hayat Aynaou[1], Imane Skiker[2], Hanane Latrech[1]
[1] Department of Endocrinology, Medical School, Mohamed the First University, Oujda, Morocco.
[2] Department of Radiology, Medical school, Mohamed the First University, Oujda, Morocco.
Address of Correspondence
Dr. Hanane Latrech,
Medical school, Hay El hikma, 60000 Oujda Morocco.
E-mail: hlatrech@hotmail.fr
Abstract
Introduction: Pycnodysostosis is a rare genetic disease characterized by osteosclerosis and bone fragility. The clinical aspects are varied including short stature, acro-osteolysis of distal phalanges, and dysplasia of the clavicles. Oral and maxillofacial manifestations of this disease are very clear. The head is usually large, a beaked nose, obtuse mandibular angle, and both maxilla and mandible are hypoplastic. Dental abnormalities are common. We report a case with the typical clinical and radiological characteristics of the Pycnodysostosis associated with a conductive hearing loss, an association rarely reported.
Case Presentation: A 12-year-female was admitted in our institute for short stature with a dysmorphic facies for evaluation. The patient reported a history of multiple fractures of the long bones after a trivial fall. On physical examination, she had the following features: short stature, limited mouth opening, short hands and feet with dysplastic nails; frontal and occipital bossing; and hypoplasia of the maxilla and mandible. Examination of the mouth: grooved palate, caries of the teeth, impacted and malposed teeth, persistent deciduous teeth and missing teeth. Laboratory investigations were normal. The radiographic examination showed a generalized increase in the bone density, slight condensation of the skull base and a very open mandibular angle. X-rays showed tapered phalanges with acro-osteolysis of the distal phalanges. A symptomatic treatment was proposed based on fracture prevention, oral hygiene, frequent dental visits and psychiatric support.
Conclusion: The clinical and radiological features are the bases for the diagnosis of this disease. It is important to make the diagnosis as early as possible in order to plan the treatment and to provide a better life quality to the patients.
Key Words: Pycnodysostosis, dysmorphy, deafness.
Introduction
Pycnodysostosis was first described in 1962 by Maroteaux and Lamy [1]. This disorder was also named “Toulouse- Lautrec Syndrome” after the French artist Henri de Toulouse-Lautrec who had this disease [1]. The main characteristics of this syndrome are: a short stature, dysplasia of the skull, obtuse mandibular angle, dysplastic clavicles, and short hands and feet [2, 3]. The main oral aspects are: midfacial hypoplasia, a grooved palate, and dental abnormalities [2, 3]. As a radiological characteristic, generalized osteosclerosis, open fontanelles and cranial sutures, absence of facial sinuses is observed. The disease is often diagnosed at a very early stage in patients consulting for an open anterior fontannelle and a short stature and sometimes belatedly by fractures. The pycnodysostosis is a rare autosomal recessive genetic disorder caused by mutation in the gene that codes the enzyme cathepsin K. We report a case of pycnodysostosis revealed by fracture and short stature associated with a conductive hearing loss, data rarely reported in the literature with description of morphological and radiographic features.
Case Report
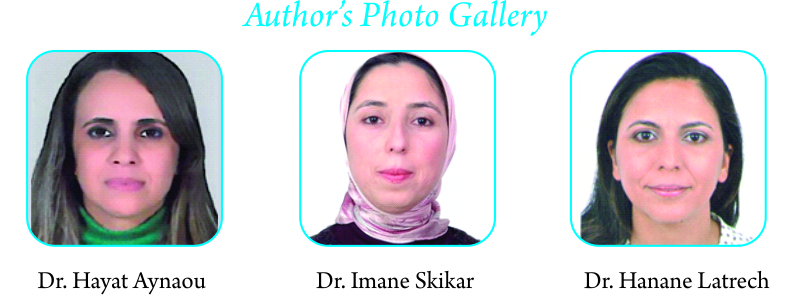
A 12-year-old girl was referred to our university hospital for short stature with a dysmorphic facies for evaluation. She was the second child of four siblings, of parents who were first-degree cousins. The maternal and neonatal history was uneventful. There was no history of similar illness in the family. The patient reported loss of teeth and nails at the age of 2 years and gave a history of multiple fractures of the long bones resulting after trivial fall: two of the right tibia and one of the left tibia. On physical examination, she had the following features: standing height at 117 cm (- 5 SDS), the cranial perimeter was 47.5 cm, sexual maturity rating showed pre-adolescent stage, presenting facial dysmorphia, limited mouth opening, short hands and feet with dysplastic nails (Fig. 1); frontal and occipital bossing; and hypoplasia of the maxilla and mandible (Fig. 2 ). Examination of the mouth: grooved palate, caries of the teeth, impacted and malposed teeth, persistent deciduous teeth and missing teeth (Fig. 3). Audiometry showed mild conductive hearing loss. Fundus examination was normal. Laboratory investigations such as complete blood count, serum calcium, phosphate, 25- hydroxyvitamin D, alkaline phosphatase, and hormonal balance (tetraiodothyronine, cortisol, and insulin growth factor 1) were normal. The radiographic examination showed a generalized increase in the bone density (Fig. 4) and horizontal fissure in the middle portion of the tibial shaft, but without obliteration of the medulary canals. (Fig. 5). Radiography of the skull showed sutures and fontanelles closed, slight condensation of the skull base and a very open mandibular angle (Fig. 6). X-rays showed tapered phalanges with acro-osteolysis of the distal phalanges of the 1st and 2nd row (Fig. 7). The bone age was 11.5 years. These clinical and radiological characteristics are in favor of a pycnodysostosis. Since there is no specific treatment, and for the financial constraints of the patient (not allowing her a growth hormone therapy), a symptomatic treatment was proposed based: on fracture prevention, oral hygiene, frequent dental visits and psychiatric support.
Discussion
Pycnodysostosis is a rare genetic disease characterized by osteosclerosis and bone fragility. The first case was reported in 1923 by Montanari, but this author reported his observation as an unusual clinical form of achondroplasia [3]. The Pycnodysostosis term was created in 1962 by Maroteaux Lamy [1]. The disorder is also known as Toulouse-Lautrec syndrome, named after the French artist who suffered from pycnodysostosis [1]. It is a rare autosomal-recessive disorder caused by genetic defect located on chromosome 1q21 in the gene that codes for the enzyme cathepsin K (CTSK) involved in the degradation of collagen type 1[4]. This mutation leads to an inhibition of the normal osteoclasts functioning and a low bone remodelling. The genetic study was not performed in our patient due to financial constraints. Several mutations have been reported to date, 45 mutations have been described: nonsense, missense, frameshift, and splice site mutations as well as small deletions, small and big insertions [5].
The incidence of this anomaly is estimated to be 1.7 per 1 million births. Actually, fewer than 200 cases have been reported since the first description in 1962 [6]. The pycnodysostosis can be confused with other diseases, such as osteopetrosis and cleidocranial dysostosis, because they present some clinical and radiographically similar signs. Osteopetrosis is characterized by generalized increased bone density. The malignant forms are recessive, in which there is severe aplastic anemia caused by the obliteration of the medullary canals and early death [7]. Cleidocranial dysostosis is characterized by a usually normal stature and normal texture.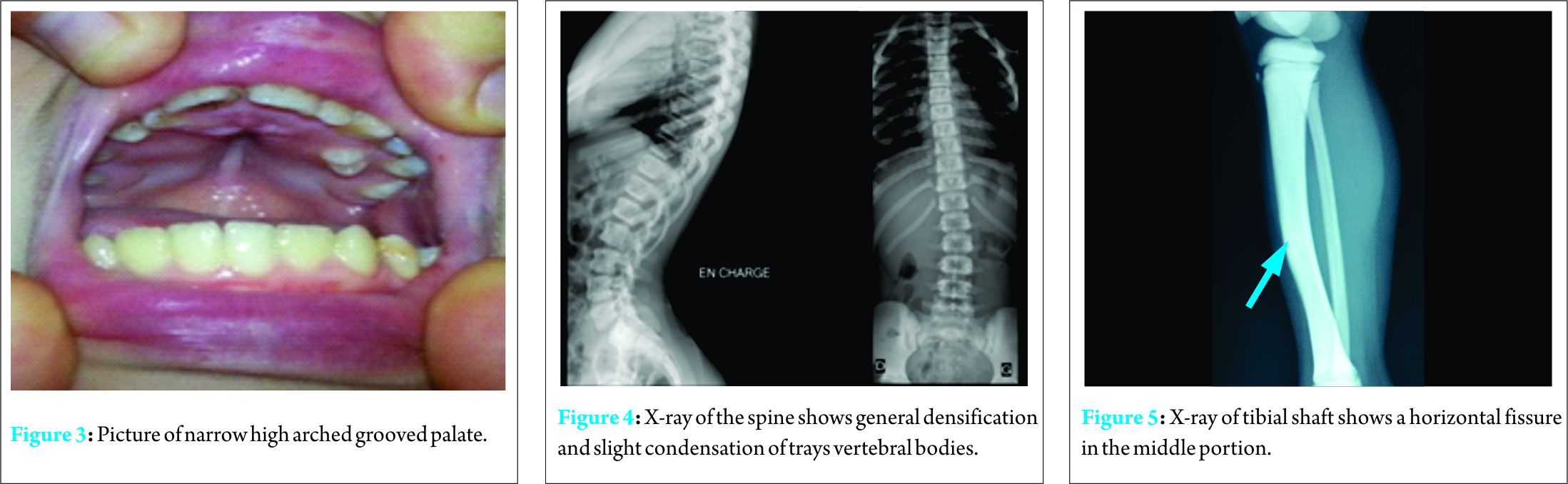
Usually the age of Pycnodysostosis’s discovery is variable ranging from 9 months to 50 years. Our patient aged 12. In our country, the Pycnodysostosis seems to be favored by the high rate of consanguinity , data already reported in the literature review in 38 % of cases. This disorder associates a characteristic appearance with an increase of bone fragility. The short stature is a constant feature; it was present in our case and also in 90.32% according to data from the literature ranging from (-1.5 DS to -6 DS) [8, 9]. Through our review of the literature, we found the following main features [2]: obtuse mandibular angle (87.09%); frontal, parietal and occipital bossing (70.96%); open fontanels and cranial sutures (64.51%); grooved palate (48.38%); midfacial hypoplasia (45.16%); acro-osteolysis of distal phalanges (38.70%); narrow palate (19.35%); open bite (16.12%). Our patient had the same characteristics except parietal bossing and open fontanels. The following dental findings were observed: premature eruption of teeth, persistence of deciduous teeth, loss of permanent teeth, malposition of teeth [2, 3]. The presence of caries probably due to dental crowding, is also reported [10]. All of these abnormalities were found in our patient. Bone fracture caused by osteosclerosis was frequent (48.8%), and in most cases a transverse fracture was present at the midshaft of a long bone [2, 9, 10]. However, mandibular fracture was seen only occasionally [9]. Our patient reported multiple episodes of fractures after trivial fall: two of the right tibia, and one of the left tibia. Usually, the medullary hematopoise [10] is respected and there are no visceral manifestations [11], although cases of extramedullary hematopoiesis and hepatosplenomegaly were reported [12]. In our case, there was no anemia or organomegaly and the audiometry showed mild conductive hearing loss. The deafness is exceptional in pycnodysostosis and has been reported in only two cases in the literature [6, 11]. The fundus examination was normal. Outside the ocular proptosis, ophthalmic reach has been reported only in one case in the literature and was represented by bilateral vitreous hyperplasia with lots of fibrous bands [11]. In adulthood: the problem is mostly functional consisting of a persistent short stature [8]. Although maxillomandibulaires abnormalities are a factor favoring upper airway obstruction, sleep apnea has rarely been documented [8]. The main radiographic maxillofacial features were [2]: obtuse mandibular angle (94.28%), large head with frontal, parietal and occiptal bossing (80%), open soft cranial sutures and fontanelles (77.14%), multiple impacted teeth (48.57%), absence or hypopeumatization of the paranasal sinuses (42.85%), wormian bones (20%), elongation of the coronoid process (14.28%) and the condyle (11.42%), supernumerary teeth (5.71%). Most of these elements were present in our patient. To date, there is no specific treatment and the management of this disease remains only symptomatic. The bone fractures are the main threat to patients affected by Pycnodysostosis, thus it is important to prevent or minimize the risk of fracture. Dental hygiene and regular dental checkups are particularly useful for those affected due to various dental abnormalities [13]. 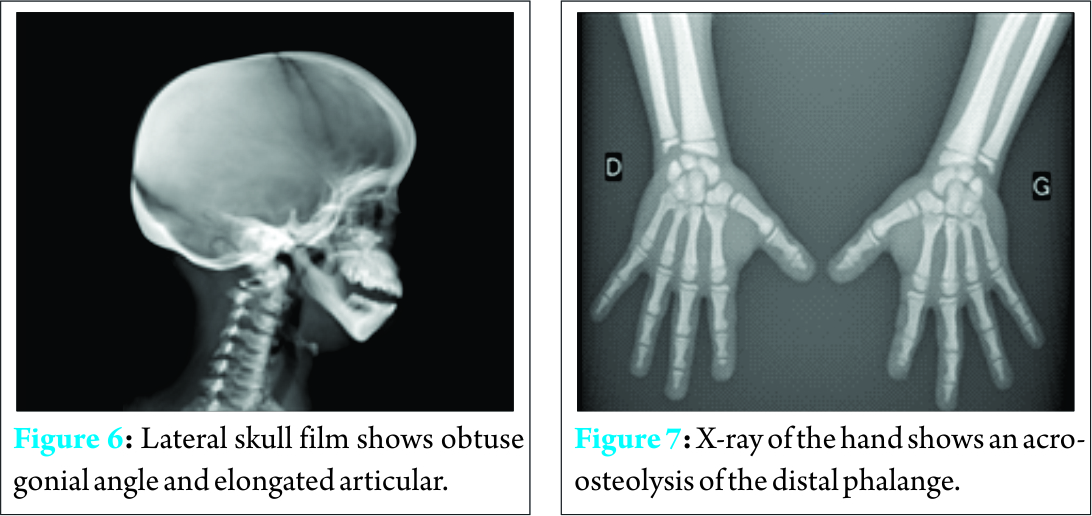
Osteomyelitis [9] is a serious complication that may be due to oral conditions of the patient, poor bone vascularity after teeth extraction, or result of iatrogenic fracture. The short size of pycnodysostosis is caused by the increased bone volume of the sella turcica that is responsible for pituitary hypoplasia and growth hormone deficiency. Recently, growth hormone therapy has resulted in a significant improvement in final height in pycnodysostosis [14]. We proposed also a psychological management to help her to accept her dysmorphic appearance and control her fear of fracture risk. Therefore, prenatal diagnosis when the mutation is known might be an appropriate approach by direct sequencing of the gene from fetal DNA [15]. Life expectancy for a pycnodysostosis patient is normal.
Conclusion
The clinical and radiological features are the bases diagnosis of this disease. It is important to make the diagnosis as early as possible in order to plan the treatment and to provide a better life quality to the patients. We suggest an active screening of all patients diagnosed with Pycnodysostosis for hearing defects and ophthalmological evaluation as a new clinical feature of this disorder.
Clinical Message
The clinical and radiological features are the bases diagnosis of this disease. It is important to make the diagnosis as early as possible in order to plan the treatment and to provide a better life quality to the patients. We suggest an active screening of all patients diagnosed with Pycnodysostosis for hearing defects and ophthalmological evaluation as a new clinical feature of this disorder.
References
1. Maroteaux P, Lamy M. The malady of Toulouse Lautrec. JAMA 1965;191(9):715–7.
2. Alves N, Oliveira RJ, Deana NF, Sampaio JC. A Morphological Features of Pycnodysostosis with Emphasis on Clinical and Radiographic Maxillofacial Findings. Int. J. Morphol 2013;31(3):921-924.
3. Elmore SM. Pycnodysostosis: a review. J. Bone Joint Surg. 1967:49(1):153-162.
4. Fujita Y, Nakata K, Yasui N, Matsui Y, Kataoka E, Hiroshima K, Shiba RI, Ochi T. Novel mutation of the cathepsin K gene in patients with pyknodysostosis and their characterization. J Clin Endocrinol Metab 2000:85(1):425–31.
5. Serap T. Current research on pycnodysostosis. Intractable Rare Dis Res. 2014;3(3):91–93.
6. Ebtesam M, Matrawy K, Shwel Y. pycnodysostosis: Clinical and radiological two new Egyptian families. Journal of pediatric sciences. 2012;4 (1)”e124.
7. Kneal E, Sante LR. Osteopetrosis; report of a case with special reference to early roentgenologic and pathological findings. AMA Am J Dis Child. 1951;81(5):693–707.
8. Nardi J, Meslier N. Pycnodysostosis and obstructive sleep apnea syndrome. Médecine du sommeil. 2010 ;7(2):63—65.
9. Muto T, Michiya H, Taira H, Murase H, Kanazawa M. Pycnodysostosis: Report of a case and review of the Japanese literature, with emphasis on oral and maxillofacial findings. Oral Surg Oral Med Oral Pathol. 1991;72(4):449-55.
10. Barnard B, Hiddema W. Pycnodysostosis with the focus on clinical and radiographic findings. S Afr J Rad 2012;16(2):74-76.
11. Mujawar Q, Naganoor R, Patil H, Thobbi AN, Ukkali S, Malagi. Pycnodysostosis with unusual findings: a case report. N Cases J. 2009;23(2):6544.
12. Santhankrishanan BR, Pannearselvam S, Ramesh S. Pyknodysostosis with visceral manifestation and rickets. Clin Paediatric. 1986: 25 (8):416–8.
13. Fukada H, Uehara S, Ando S, Shinoda K. A case of pycnodysostosis: its oral aspects. J. Nihon Univ. School of Dent. 1967;9(4): 164-169.
14. Karamizadeh Z, Ilkhanipoor H, Bagheri F. Effect of Growth Hormone treatment on Height Velocity of Children with Pycnodysotosis. Iran J Pediatr 2014;24(2):161-165.
15. Azagui Y, Zaidane A, Belmoubarek A, Ahed K, Haddoun AR, Ouarab M. Diaphyseal femur fracture in pycnodysostosis: a case report. Rev Mar Rhum 2013;24:52-5.
| How to Cite This Article: Aynaou H, Skiker I, Latrech H. Short Stature Revealing a Pycnodysostosis: A Case Report. Journal of Orthopaedic Case Reports 2016 April – June;6(2): 43-45. Available from: https://www.jocr.co.in/wp/2016/04/01/2250-0685-426-fulltext/ |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


