
[box type=”bio”] What to Learn from this Article?[/box]
Aggressive vertebral body hemangiomas can cause compressive myelopathy due to extra-osseous extension and can typically be identified by their corduroy cloth and polka dot appearance.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 7-10| Denver Steven Pinto, V Ravi Hoisala, Pavan Gupta, Parthasarathy Sarkar. DOI: 10.13107/jocr.2250-0685.724
Authors: Denver Steven Pinto[1], V Ravi Hoisala[1], Pavan Gupta[1], Parthasarathy Sarkar[1]
[1] Department of Radiodiagnosis, St. Johns Medical College, Koramangala, Bengaluru, Karnataka. India.
Address of Correspondence
Dr. Denver Steven Pinto,
Department of Radiology, St. Johns Medical College, Koramangala, Bengaluru – 560 034, Karnataka, India.
E-mail: dforever100@gmail.com
Abstract
Introduction: Hemangiomas are benign tumors characterized by proliferation of blood vessels. A few hemangiomas are aggressive, characterized by bone expansion and extraosseous extension. These benign tumors may be mistaken for metatasis resulting in unnecessary biopsies, which have a high risk of hemorrhage. These hemangiomas can spread not just into the paraspinal soft tissues but also into the epidural region of the spinal canal causing cord compression and paraparesis. These clinical symptoms can be relieved by surgical decompression of the posterior elements, embolization or radiotherapy.
Case Report: In this case report the authors describe the imaging features of two aggressive vertebral body hemangiomas in two patients with back pain. One patient had isolated motor deficit while the other patient had both sensory and motor deficit. On imaging this benign tumor was seen involving both the vertebral body and its posterior elements with paraspinal and epidural extension causing compressive myelopathy.
Conclusion: Thus, these case reports help identify the characteristic imaging features of an aggressive vertebral body hemangioma, preventing unnecessary and often risky biopsy. The clinical symptoms of the patient can be relieved by surgical decompression of the posterior elements or by radiotherapy. Use of onyx for intraarterial embolization is now believed to be the safest and most efficacious method for treatment of aggressive vertebral body hemangiomas. However, in the absence of definite guidelines, a multicentric study is warranted to prove that embolization with onyx is better than surgery with post-operative radiotherapy.
Keywords: Aggressive vertebral body hemangioma, compressive myelopathy, magnetic resonance imaging.
Introduction
Vertebral body hemangioma is a common condition with various case series reporting its incidence to be between 10% and 27% [1]. In the bone, they are of dysembryogenetic origin otherwise also called as hamartomatous lesions. They have high vascularity, intralesional oedema and intralesional fat [2]. Most hemangiomas are small, about a third are multiple and only 0.9-1.2% of hemangiomas cause symptoms [1, 3]. Very few hemangiomas are aggressive causing bony expansion and extraosseous extension, with extension into the paraspinal and epidural spaces [4, 5, 6]. New onset of back pain with subacute progression of a thoracic myelopathy has been reported as the most common presentation for patients with neurological deficit due to aggressive vertebral body hemangiomas [4]. Thus, it is important to recognize this entity, include it in the clinical differential diagnosis and to look for the extensions of such vertebral body hemangiomas.
Case Reports
Case 1
History and examination findings
Reported here is a case of a 48-year-old Indian woman with back pain, which was insiduous in onset, localized to the mid-back and aggravated on sitting, walking and change of posture, with progressive weakness of bilateral lower limbs, more severe in the distal muscles (power was 2/5 in the distal muscles at the time of presentation). The power was graded according to the Louisiana State Medical University Medical Centre grading for individual muscle power. The patient has increased tone, spasticity, clonus and extensor plantar reflex in the lower limbs.
Imaging
On magnetic resonance imaging (MRI) a T2 and short tau-inversion recovery (STIR) hyperintense (aggressive hemangiomas contain less fat and more vascular stroma thus producing a high signal on T2 weighted images) expansile, osseous lesion with trabecular thickening, with extraosseous intraspinal component was seen causing spinal cord compression with T2 hyperintensity of the spinal cord (Fig. 1).
Computed tomography (CT) was done for confirmation and showed thickened vertically oriented trabeculae in D7 vertebral body with epidural extraosseous extension into the spinal canal and the paravertebral soft tissues giving rise to a polka dot (axial) and corduroy cloth appearance (saggital images). The hemangioma was seen to involve the laminae and pedicles of the vertebra (Fig. 2).
Follow-up
A clinical decision to perform surgical decompression was taken for the first patient. Intraoperatively, a mass was seen arising from the vertebral body and extending into the spinal canal. Tumor showed a tuft of vessels in the bony tissue which had very high vascularity. Histopathology confirmed the lesion to be a hemangioma. Laminectomy was done for the patient to cause spinal decompression. Pedicle screw was placed into the vertebral body affected by the aggressive vertebral body hemangioma. Difficulty was faced while passing the pedicle screw into the normal vertebra (superior) during the surgery, and one of the pedicle screws inadvertently indented the cord after being displaced into the spinal canal (Fig. 3). Displacement of the pedicle screws is a known complication which can cause spinal cord compromise. This case report reiterates the need for the use of alternate treatment modalities like radiotherapy and embolization in aggressive vertebral body hemangiomas.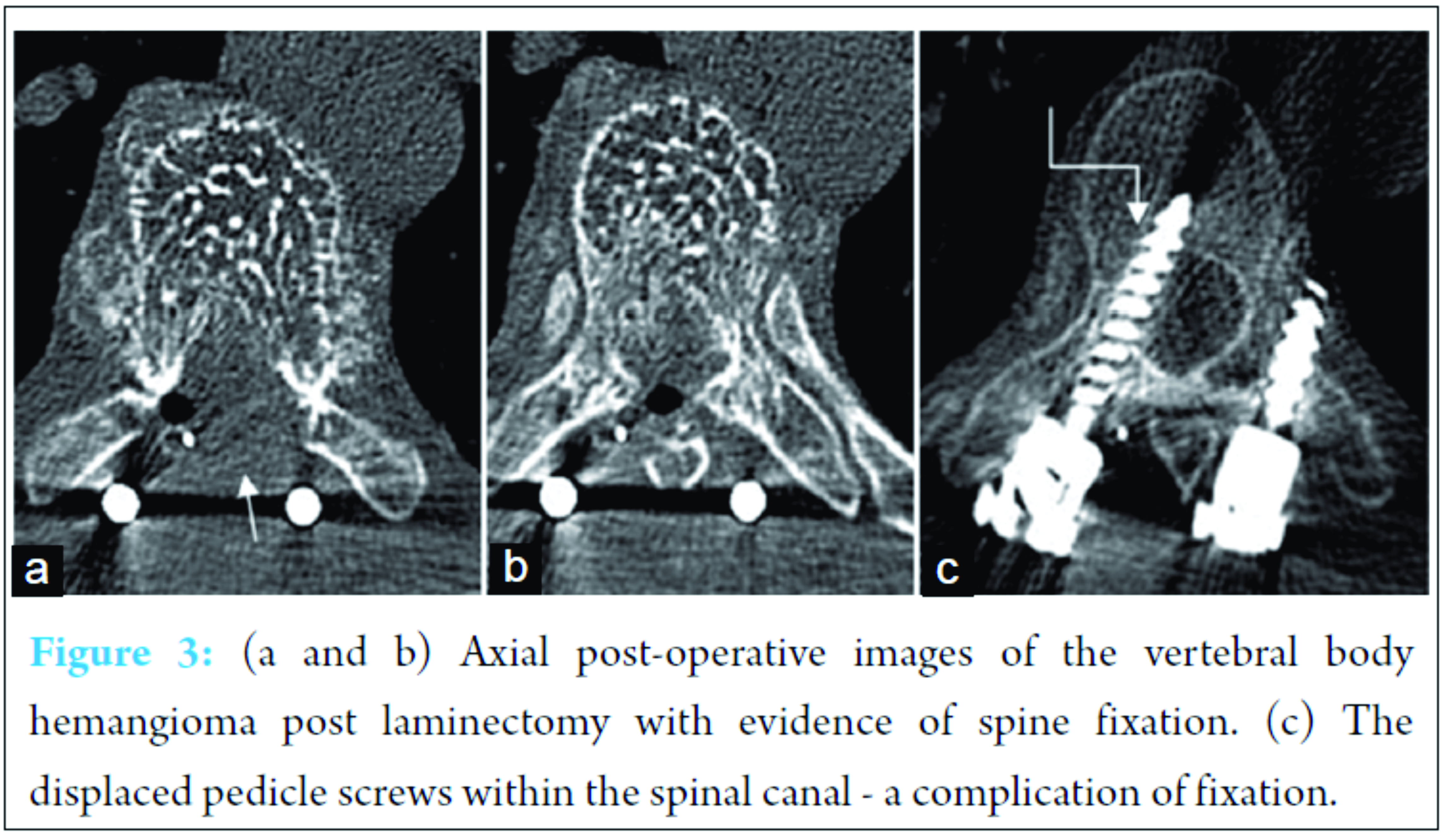
In the immediate post-operative period the power of the lower limbs reduced to Grade 2. However after the inflammation subsided at 6 months of follow-up, the power had increased to Grade 4. The patient is currently undergoing physiotherapy for her symptoms.
Case 2
History and examination findings
Reported here is a case of a 24-year-old Indian woman in the post natal period who had progressively increasing back pain and loss of sensation in the limbs following delivery of her first child by a lower segment Caesarian section. Patient on examination had loss of sensation in both the legs, with power of 3/5 in the distal muscles of the lower limb with increased tone and spasticity. The proximal muscles of the lower limb had a power of 4/5.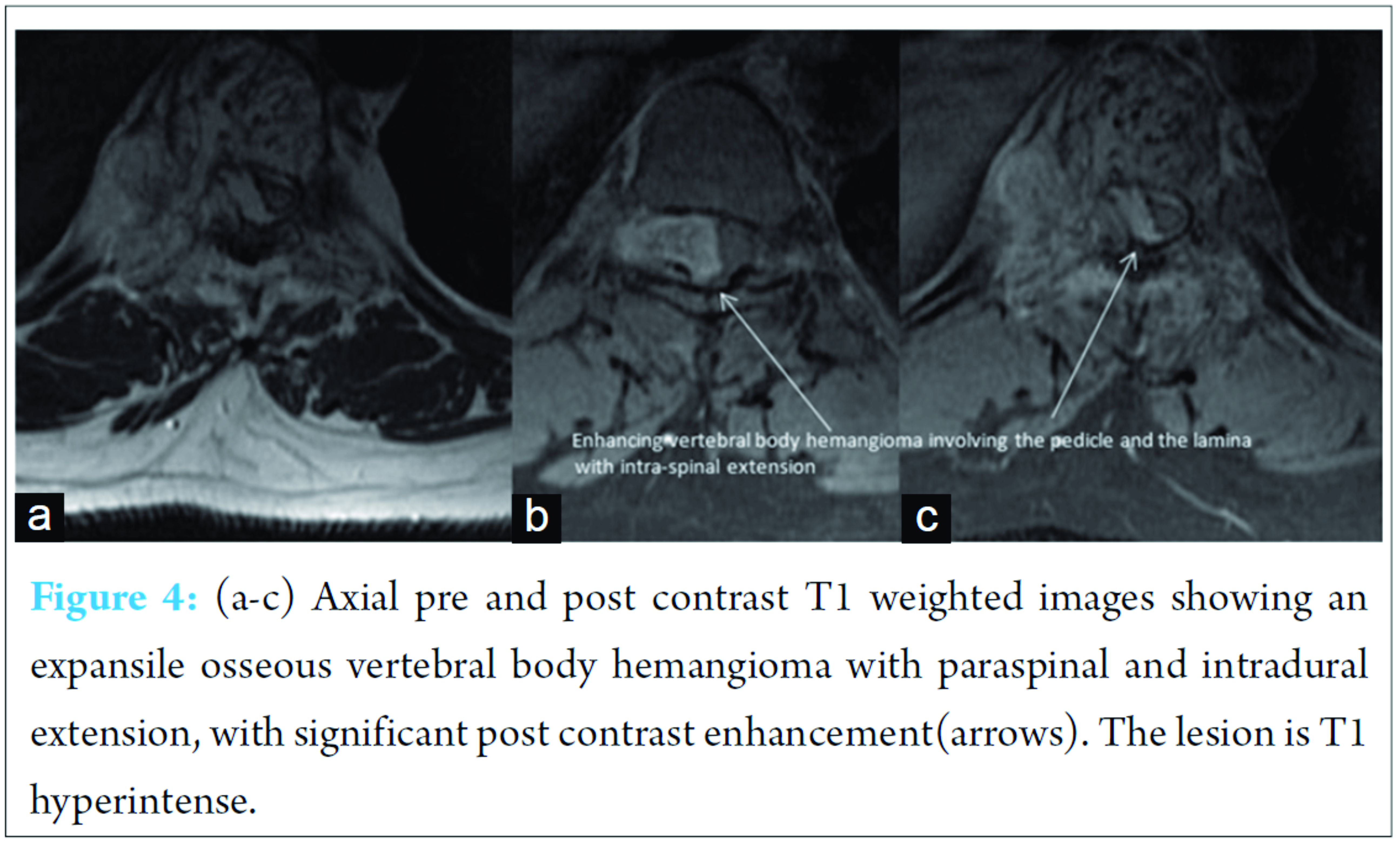
Imaging
MRI with contrast was done which showed a D10 T2 and STIR hyperintense expansile, osseous lesion with trabecular thickening as seen in the previous case with paravertebral and intraosseous extension causing compressive myelopathy. Significant enhancement was seen in the right paravertebral region involving the lamina and the pedicles with epidural extension (Fig. 4).
Compressive myelopathy was seen as T2 hyperintensity of the cord with reduced intraspinal space secondary to bone expansion (Fig. 5).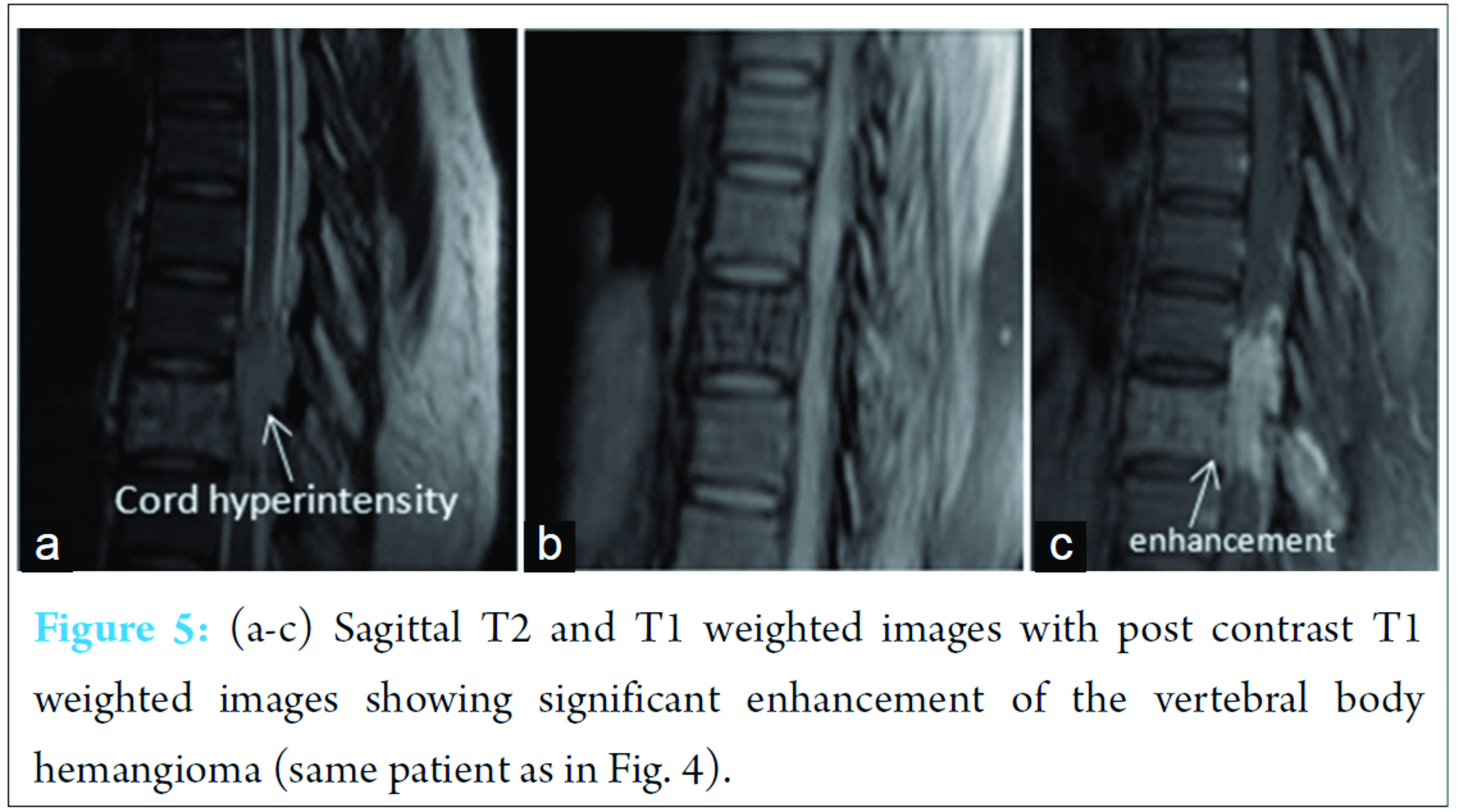
This pattern on MRI was considered typical and a diagnosis of an aggressive vertebral body hemangioma causing compressive myelopathy was given.
Follow-up
This patient was offered embolization or radiotherapy for treatment. The patient opted for radiotherapy and chose to undergo radiotherapy at a centre in her city of residence. The patient was then lost to follow-up.
Discussion
Vertebral body hemangiomas causing compression of the spinal cord can occur at any age and they have been noted to have a predilection for the thoracic spine. Hemangiomas are known to cause rarefaction of the bone with exaggerated vertical striations representing reinforced trabeculae [2]. The vascularity, interstitial oedema and intralesional fat determine the signal intensity of the hemangioma [7]. A review of literature showed that the differential diagnosis of compressive hemangiomas with a coarse reticular pattern and extradural extension includes rare differentials like hemangioblastoma, lymphangioma, and Ewing sarcoma [2]. However, in the presence of typical imaging features as described above there is no need for any differential diagnosis. While the first patient underwent surgery, the second patient opted for radiotherapy for the treatment of the lesion. Few cases of pregnancy causing symptomatic vertebral body hemangiomas with epidural component have been reported in literature. Vascular, hemodynamic and endocrinal causes have been postulated to cause increase of hemangioma size during pregnancy. Inferior venecaval compression by the gravid uterus causes decreased venous outflow resulting in expansion of the hemangioma. High progesterone level with plasma volume expansion and endothelial proliferative activity of estrogen causes increase in the size of the hemangioma [8]. In the second patient reported the progression occured in the post natal period during lactation. Treatment options for aggressive vertebral body hemangiomas include interventional radiology options like embolization or ethanol injection, radiotherapy or surgery. Literature shows all these modalities to be effective in treatment [3, 4, 5, 9, 10]. As early as 1994, intralesional ethanol injection was advocated for treatment [11]. However, ethanol dosage of <15 ml was recommended. A case series of aggressive vertebral body hemangiomas described increased volume of ethanol injection due to interstitial injection of ethanol secondary to inability to inject into an arterial feeder or due to excessive bleeding [12]. A CT angiography prior to ethanol injection is also desirable to localize the vascular part of the tumor because success of the procedure depends upon placement of the needle tip and injection of the ethanol into the vascular part of the tumor [12]. Though initially embolization was found to be useful as an adjunct to surgery, currently embolization with onyx is believed to be the effective treatment for aggressive vertebral body hemangiomas [13, 14, 15]. A preoperative digital subtraction angiography is ideal and necessary to detect arterial feeders. Though the surgical option is effective, it always raises the risk of intra-operative (as in the first patient) or anesthetic complications. A percutaneous vertebroplasty may be offered to the patient when the patient has a secondary compression fracture. Here, polymethyl metha-acrylate is injected into the bone. This results in pain relief and bone strengthening and may reduce the need for aggressive surgery [16]. Radiotherapy following surgery was found to cause complete regression of the tumor in a few cases [17]. Radiotherapy alone was found to cause total or near total regression of symptoms of aggressive vertebral body hemangiomas in 77% of patients in a case series of 9 patients. However this involved administering a radiation dose of 3000-4000 rad, with 200 rad/day, with five fractions a week for upto 62 months [18]. Malignant transformation has also been reported in patients subjected to repetitive irradiation for treatment [19]. A multicentre study involving 96 patients with a median follow-up of 68 months, showed that with doses of about 3400 rad the response rate of patients was 90.5% with 62% of patients showing a complete response. This multicentric study concluded that radiotherapy was easy, safe and effective for pain relief [20]. Thus, with myriad treatment options available it is not only necessary to arrive at an accurate diagnosis of this condition, avoiding unnecessary biopsy, it is also important to decide on the most suitable modality or the best combination of modalities for treatment. Though there may not be definite guidelines for management of aggressive vertebral body hemangiomas surgery is always accompanied by risk of intraoperative spinal cord injury and radiotherapy is limited by the radiation dose [3]. Embolization with onyx is considered effective and safe with more controlled injection with shorter injection times [14, 21]. Reflux into the epidural venous plexus may occur without significant morbidity confirming the safety of embolization with onyx [21].
Conclusions
Aggressive vertebral body hemangiomas can have epidural extension and cause parapareisis due to compressive myelopathy. The clinical symptoms of the patient can be relieved by surgical decompression of the posterior elements or by radiotherapy. Use of onyx for intraarterial embolization is now believed to be the safest and most efficacious method for treatment of aggressive vertebral body hemangiomas. However, in the absence of definite guidelines a multicentric study is warranted to prove that embolization with onyx is better than surgery with post-operative radiotherapy.
Clinical Message
Aggressive vertebral body hemangiomas must not be mistaken for vertebral metastasis causing spinal cord compression. For patients with aggressive vertebral body hemangiomas treatment option of embolization and must be offered before surgery and radiotherapy
References
1. Barzin M, Maleki I. Incidence of vertebral hemangioma on spinal magnetic resonance imaging in Northern Iran. Pak J Biol Sci 2009;12(6):542-544.
2. Rodallec MH, Feydy A, Larousserie F, Anract P, Campagna R, Babinet A, et al. Diagnostic imaging of solitary tumors of the spine: what to do and say. Radiographics 2008;28(4):1019-1041.
3. Aich RK, Deb AR, Banerjee A, Karim R, Gupta P. Symptomatic vertebral hemangioma: treatment with radiotherapy. J Cancer Res Ther 2010;6(2):199-203.
4. Fox MW, Onofrio BM. The natural history and management of symptomatic and asymptomatic vertebral hemangiomas. J Neurosurg 1993;78(1):36-45.
5. Laredo JD, Reizine D, Bard M, Merland JJ. Vertebral hemangiomas: radiologic evaluation. Radiology 1986;161(1):183-189.
6. Schrock WB, Wetzel RJ, Tanner SC, Khan MA. Aggressive hemangioma of the thoracic spine. J Radiol Case Rep 2011;5(10):7-13.
7. Baudrez V, Galant C, Vande Berg BC. Benign vertebral hemangioma: MR-histological correlation. Skeletal Radiol 2001;30(8):442-446.
8. Gupta M, Nayak R, Singh H, Khwaja G, Chowdhury D. Pregnancy related symptomatic vertebral hemangioma. Ann Indian Acad Neurol 2014;17(1):120-122.
9. Chen HI, Heuer GG, Zaghloul K, Simon SL, Weigele JB, Grady MS. Lumbar vertebral hemangioma presenting with the acute onset of neurological symptoms. Case report. J Neurosurg Spine 2007;7(1):80-85.
10. Jankowski R, Nowak S, Zukiel R, Szymas J, Sokól B. Surgical treatment of symptomatic vertebral haemangiomas. Neurol Neurochir Pol 2011;45(6):577-582.
11. Heiss JD, Doppman JL, Oldfield EH. Brief report: relief of spinal cord compression from vertebral hemangioma by intralesional injection of absolute ethanol. N Engl J Med 1994;331(8):508-511.
12. Doppman JL, Oldfield EH, Heiss JD. Symptomatic vertebral hemangiomas: Treatment by means of direct intralesional injection of ethanol. Radiology 2000;214(2):341-348.
13. Smith TP, Koci T, Mehringer CM, Tsai FY, Fraser KW, Dowd CF, et al. Transarterial embolization of vertebral hemangioma. J Vasc Interv Radiol 1993;4(5):681-685.
14. Hurley MC, Gross BA, Surdell D, Shaibani A, Muro K, Mitchell CM, et al. Preoperative Onyx embolization of aggressive vertebral hemangiomas. AJNR Am J Neuroradiol 2008;29(6):1095-1097.
15. Acosta FL Jr, Sanai N, Chi JH, Dowd CF, Chin C, Tihan T, et al. Comprehensive management of symptomatic and aggressive vertebral hemangiomas. Neurosurg Clin N Am 2008;19(1):17-29.
16. Cotten A, Boutry N, Cortet B, Assaker R, Demondion X, Leblond D, et al. Percutaneous vertebroplasty: state of the art. Radiographics 1998;18(2):311-320.
17. Bremnes RM, Hauge HN, Sagsveen R. Radiotherapy in the treatment of symptomatic vertebral hemangiomas: technical case report. Neurosurgery 1996;39(5):1054-1058.
18. Faria SL, Schlupp WR, Chiminazzo H. Radiotherapy in the treatment of vertebral hemangiomas. Int J Radiat Oncol Biol Phys 1985;11(2):387-390.
19. Obana Y, Tanji K, Furuta I, Yamazumi T, Hashimoto S, Kikuchi H, et al. A case of malignant transformation in thoracic vertebral hemangioma following repetitive irradiation and extraction. Pathol Int 1996;46(1):71-78.
20. Heyd R, Seegenschmiedt MH, Rades D, Winkler C, Eich HT, Bruns F, et al. Radiotherapy for symptomatic vertebral hemangiomas: results of a multicenter study and literature review. Int J Radiat Oncol Biol Phys 2010;77(1):217-225.
21. Sedora-Roman NI, Gross BA, Reddy AS, Ogilvy CS, Thomas AJ. Intra-arterial Onyx embolization of vertebral body lesions. J Cerebrovasc Endovasc Neurosurg 2013;15(4):320-325.
 |
 |
 |
 |
| Dr. Denver Steven Pinto | Dr. V Ravi Hoisala | Dr. Pavan Gupta | Dr. Parthasarathy Sarkar |
| How to Cite This Article: Pinto DS, Hoisala VR, Gupta P, Sarkar P. Aggressive Vertebral Body Hemangioma Causing Compressive Myelopathy – Two Case Reports. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):7-10 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


