
[box type=”bio”] What to Learn from this Article?[/box]
Isolated dislocation of the fifth carpometacarpal joint can be managed conservatively with good outcome if diagnosed early; however, if the initial reduction is unstable or there is a delay in diagnosis or presentation, it is imperative to use K-wires for fixation after closed/open reduction.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 14-16| Rashid Anjum, Amit Roy, Kamran Farooque, Vijay Sharma. DOI: 10.13107/jocr.2250-0685.728
Authors: Rashid Anjum[1], Amit Roy[1], Kamran Farooque[1], Vijay Sharma[1]
[1] Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi. India.
Address of Correspondence:
Dr. Rashid Anjum,
D 30 MMU Residential Complex Mullana, Ambala – 133 207, Haryana. India.
E-mail: raashidanjum@gmail.com
Abstract
Introduction: Isolated pure dislocation of the fifth carpometacarpal (CMC) joint is a very rare injury and classified depending on displacement of the metacarpal base. This rare injury is often difficult to recognize and is liable to be overlooked. The purpose of this case report is to present a patient with an isolated dislocation of the fifth CMC joint that was satisfactorily treated with closed reduction and ulnar gutter pop slab.
Case Report: A 21-year-old male presented with severe pain on the right carpus following a fall with injury to right hand. There was a mild swelling at fifth CMC joint region and a bony prominence was felt dorsally, little finger presented an abduction deformity, and there was apparent shortening of the fifth ray. A diagnosis of isolated dislocation of fifth CMC dislocation was made based on radiographs. Immediate closed reduction was done in emergency room by applying longitudinal traction and direct pressure on metacarpal base dorsally, reduction was stable and confirmed by postreduction radiographs.
Conclusion: Isolated pure dislocation of the fifth CMC joint is very rare injury and is prone to be missed in emergency room and particular attention should be made to diagnose it in polytrauma patients.
Keywords: Carpometacarpal dislocation, ulnopalmar, fifth carpometacarpal.
Introduction
Isolated dislocation of the carpometacarpal (CMC) joints is usually high-energy injuries with the involvement of associated structures, often neurovascular. Isolated dislocation of fifth CMC joint is very uncommon injury, and particular care must be given to the examination of ulnar nerve function because of its proximity to the fifth CMC joint [1]. We report a case of isolated dislocation of fifth CMC joint successfully managed non-operatively. The mechanism of this injury, clinical presentation, and treatment options are discussed, with a review of the literature.
Case Report
A 21-year-old male presented to the Emergency Department with severe pain on right carpus following a fall with injury to the right hand. There was a mild swelling at fifth CMC joint region and a bony prominence was felt dorsally, little finger presented an abduction deformity, and there was apparent shortening of the fifth ray. Standard radiographs were obtained which revealed isolated pure dislocation of the fifth CMC joint without any other associated injury or fracture of other metacarpals or wrist (Fig. 1a and b). A diagnosis of isolated dislocation of fifth CMC dislocation was made based on radiographs. Immediate closed reduction was done in emergency room by applying longitudinal traction and direct pressure on metacarpal base dorsally, reduction was stable and confirmed by postreduction radiographs (Fig. 2a and b), an ulnar gutter pop slab was applied for 4-6 weeks. At last follow-up, the patient was doing all routine activities with normal grip strength and full range of motion at wrist without pain.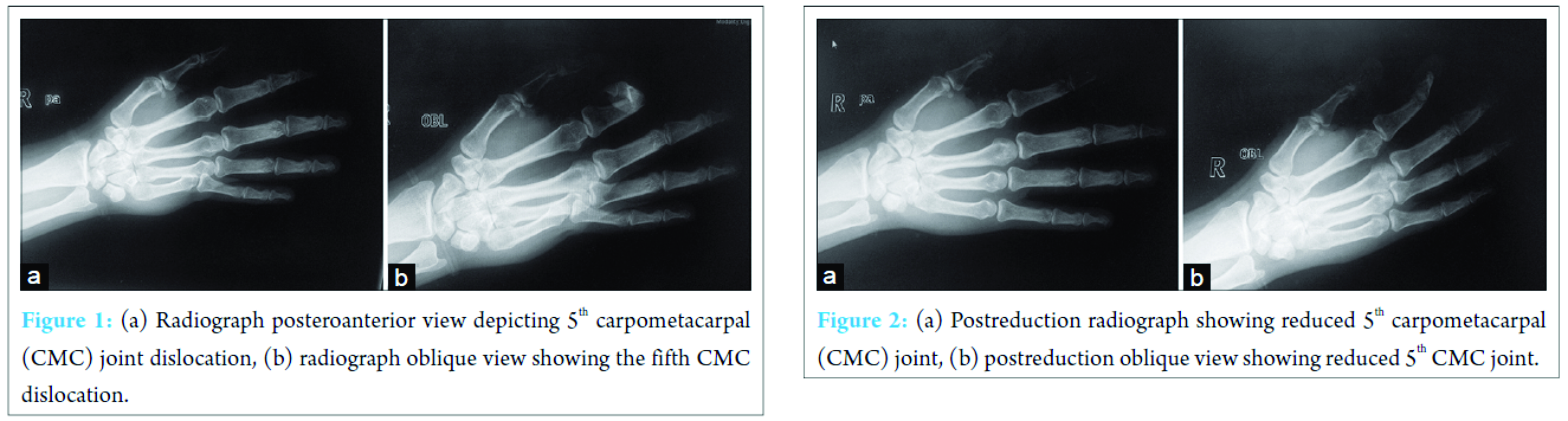
Discussion
An isolated pure dislocation of fifth CMC joint is a relatively rare injury first reported by McWhorter in 1918. This injury has been recognized to be of two types depending on dorsal or volar displacement, which may be easily missed on routine radiographs in a trauma patient [2, 3, 4, 5, 6]. Stability at the finger CMC joints is provided by a system of four ligaments. There is a high degree of variation with dorsal, multiple palmar, and two sets of interosseous ligaments (only one between the long and ring metacarpals) [7, 8]; furthermore, the ECU tendon inserts on the fifth metacarpal base. Dorsal dislocations of the CMC joints are relatively more frequent as compared to volar, affecting commonly the fourth and fifth fingers [9]. CMC dislocations associated with fifth or other metacarpal fracture or hamate fractures are more frequent than pure dislocations [10, 11, 12]. It is also necessary in patients with a fracture of fourth metacarpal to examine a possible association of the occult fifth CMC joint dislocation. Simultaneous divergent CMC joint dislocation involving different digits is another rare injury pattern reported in literature [13]. Saleemi reported a variety of these injuries including an isolated fifth CMC joint dislocation to the ulnar side, visualized only in the posteroanterior view of hand X-ray [14]. Nalebuff classified the volar dislocations into two groups according to the displacement of the fifth metacarpal base: Radial palmar and ulnopalmar. In radial palmar type, the fifth metacarpal base is completely denuded of attachments; whereas in ulnopalmar type, the pisometacarpal ligament and tendon attachments are intact [6, 7]. Although it is difficult for the patients to remember the exact mechanism of trauma, this injury is thought to be caused by a direct blow transmitted to the dorsal and ulnar aspect of the fifth metacarpal [8]. Clinical findings are those of pain and swelling at the base of fifth metacarpal and an apparent shortening of the affected metacarpal. The apparent shortening in our case was assessed using Indian salutation test. Roberts and Holland treated three patients of fifth CMC dislocation by closed reduction and splintage; however, in one patient, partial redisplacement occurred after the removal of the splint. Berg and Murphy reported successful management of an ulnopalmar dislocation of the fifth CMC joint by closed means in a splint [2].
Conclusion
Isolated pure dislocation of the fifth CMC joint is very rare injury and is prone to be missed in emergency room and particular attention should be made to diagnose it in polytrauma patients. It can be managed conservatively with good outcome if diagnosed early as in our case; however, if the initial reduction is unstable or there is delay in diagnosis or presentation, it is imperative to use K-wires for fixation after closed/open reduction.
Clinical Message
Isolated pure dislocation of fifth CMC joint is very rare and is likely to be missed in the setting of polytrauma, careful evaluation is required for early diagnosis and management.
References
1. Kumar R, Malhotra R. Divergent fracture-dislocation of the second carpometacarpal joint and the three ulnar carpometacarpal joints. J Hand Surg Am 2001;26(1):123-129.
2. Berg EE, Murphy DF. Ulnopalmar dislocation of the fifth carpometacarpal joint-successful closed reduction: Review of the literature and anatomic re-evaluation. J Hand Surg Am 1986;11(4):521-525.
3. Chen VT. Dislocation of carpometacarpal joint of the little finger. J Hand Surg Br 1987;12(2):260-263.
4. Fischer JW, Waseem M, Gambhir A, Creedon RJ. Ulnopalmar dislocation of the fifth carpometacarpal joint. A rare injury. Acta Orthop Belg 2002;68(2):175-177.
5. Ker HR. Dislocation of the fifth carpometacarpal joint. J Bone Joint Surg Br 1955;37-B:254-256.
6. Henderson JJ, Arafa MA. Carpometacarpal dislocation. An easily missed diagnosis. J Bone Joint Surg Br 1987;69(2):212-214.
7. Dzwierzynski WW, Matloub HS, Yan JG, Deng S, Sanger JR, Yousif NJ. Anatomy of the intermetacarpal ligaments of the carpometacarpal joints of the fingers. J Hand Surg Am 1997;22(5):931-934.
8. Nakamura K, Patterson RM, Viegas SF. The ligament and skeletal anatomy of the second through fifth carpometacarpal joints and adjacent structures. J Hand Surg Am 2001;26(6):1016-1029.
9. Fisher MR, Rogers LF, Hendrix RW. Systematic approach to identifying fourth and fifth carpometacarpal joint dislocations. AJR Am J Roentgenol 1983;140(2):319-324.
10. Dennyson WG, Stother IG. Carpometacarpal dislocation of the little finger. Hand 1976;8(2):161-164.
11. McWhorter GL. Isolated and complete dislocation of the fifth carpometacarpal joint: Open operation. Surg Clin Chic 1918;2(1):793-796.
12. Roberts N, Holland CT. Isolated dislocation of the base of the fifth metacarpal. Br J Surg 1936;23(91):567-571.
13. Busa R, Internullo G, Caroli A. Divergent dislocation of the fourth and fifth carpometacarpal joints. J Hand Surg Am 1998;23(3):529-531.
14. Saleemi AJ, Iqbal MJ. Ulnar dislocation of fifth carpometacarpal joint. Hand Surg 2005;10(1):87-90.
 |
 |
 |
 |
| Dr. Rashid Anjum | Dr. Amit Roy | Prof. Kamran Farooque | Dr. Vijay Sharma |
| How to Cite This Article: Anjum R, Roy A, Farooque K, Sharma V. An Isolated Pure Dislocation of Fifth Carpometacarpal Joint: Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):14-16 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


