
[box type=”bio”] What to Learn from this Article?[/box]
Systemic capillary leak syndrome may result in severe lower limb deformity. Although it can be treated as a compartment syndrome sequelae, more serious intra- and post-operative complications have to be considered.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 52-56| Luis Sobral, Ana C Ângelo, Afonso Caetano, Joaquim Rodeia, Isabel Rosa. DOI: 10.13107/jocr.2250-0685.748
Authors: Luis Sobral[1], Ana C Ângelo[1], Afonso Caetano[1], Joaquim Rodeia[1], Isabel Rosa[1]
[1] Department of Traumatology and Orthopaedics, São Francisco Xavier Hospital, Estrada do Forte do Alto do Duque 1449-005, Lisboa, Portugal.
Address of Correspondence
Dr. Luis Filipe Loureiro Sobral,
Department of Traumatology and Orthopaedics, São Francisco Xavier Hospital, Estrada do Forte do Alto do Duque 1449-005, Lisboa, Portugal.
E-mail: luisflsobral@gmail.com
Abstract
Introduction: Systemic capillary leak syndrome (SCLS) is a rare condition of unknown etiology defined by sudden episode of hypotension, high hematocrit, and low serum protein concentration due to capillary hyperpermeability. Several treatments have been published for this pathology and eventual compartment syndrome but not for the disabling consequences. This clinical case highlights the negative orthopedic consequences of a severe systemic attack and reports a subsequent deformity treatment option that resulted in the patient quality of life improvement. To our knowledge, orthopedic surgery for SCLS induced foot and ankle deformity is presented for the first time.
Case Report: A 40-year-old Caucasian female patient was referred to our institution for bilateral foot and ankle deformity after compartment syndrome during SCLS attack. She presented a bilateral rigid equino-cavo-varus-adductus deformity causing walk impairment. Bilateral ankle fusion by retrograde nailing was performed in a two-staged procedure. Rigid claw toes were also surgically addressed in an additional procedure. Radiologically, apparent ankle fusion occurred at 3 months post-operative in both sides. Deformity correction allowed the patient to regain walking capacity. A right ankle tibiotalar failed arthrodesis was noticed at 24 months post-operative. Prophylactic human immunoglobulin therapy was initiated after the last surgery with no recurrent attack registered during the 38 months follow-up period.
Conclusion: Bilateral ankle fusion improved this patient quality of life by restituting walking capacity and lowering the probability of lower limb deformity related ulcers and infections. Major and minor complications are also discussed. This report contributes to the global knowledge about this syndrome and elicits the importance of the induced deformities surgical correction.
Keywords: Systemic capillary leak syndrome, compartment syndrome, equino-varus, ankle fusion, ankle retrograde nailing, human immunoglobulin.
Introduction
Systemic capillary leak syndrome (SCLS), described by Clarkson et al. in 1960 [1], is a rare condition defined by sudden episodes of hypovolemic shock, elevated hematocrit, and hypoalbuminemia without albuminuria [2, 3]. The etiology is still unknown, although several possible triggers have been reported as upper respiratory tract infections, sustained physical effort and menstruation [1, 4]. It results in generalized or segmental edema and, in severe cases, compartment syndrome requiring emergent fasciotomy [2, 3, 4, 5]. The sudden intracompartmental high pressure often originates vascular and neurological damage and consequent lower limb deformity [3, 6]. Prolonged hospital stay may also aggravate this condition with osteoporosis following a long-term immobilization or limb disuse. Deformity frequently leads to walk impairment and decreased quality of life [7]. A few retrospective studies report ankle fusion for correction of compartment syndrome induced deformity. None of them included SCLS etiology for compartment syndrome [6, 7]. Several treatments have been published for SCLS and compartment syndrome [1, 2, 3, 4, 5] but not for the disabling consequences. To our knowledge, orthopedic surgery for SCLS induced foot and ankle deformity is presented for the first time.
Case Report
A 40-year-old Portuguese woman complained of severe limitations in daily life activities due to bilateral foot and ankle deformity. She had been previously diagnosed with SCLS after sudden episode of hypotension, high hematocrit, and low serum protein concentration. This acute phase was managed by fluid resuscitation. The consequent generalized compartment syndrome was treated with extensive fasciotomies of both arms, forearms, hands, thighs, and legs. She stayed 3 weeks in the intensive care unit and 8 months hospitalized. Although an intense physical therapy program was applied, she was unable to walk and autonomy was limited to a wheelchair.
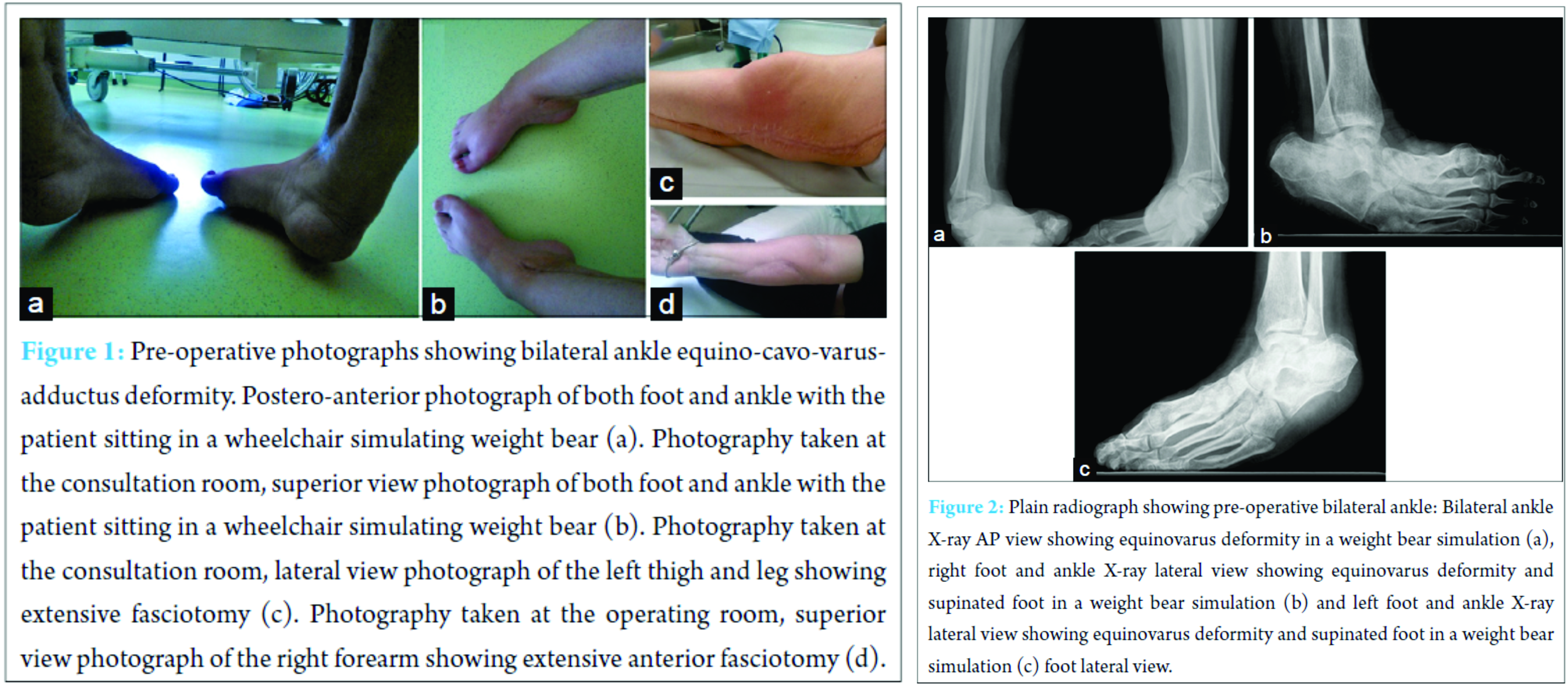
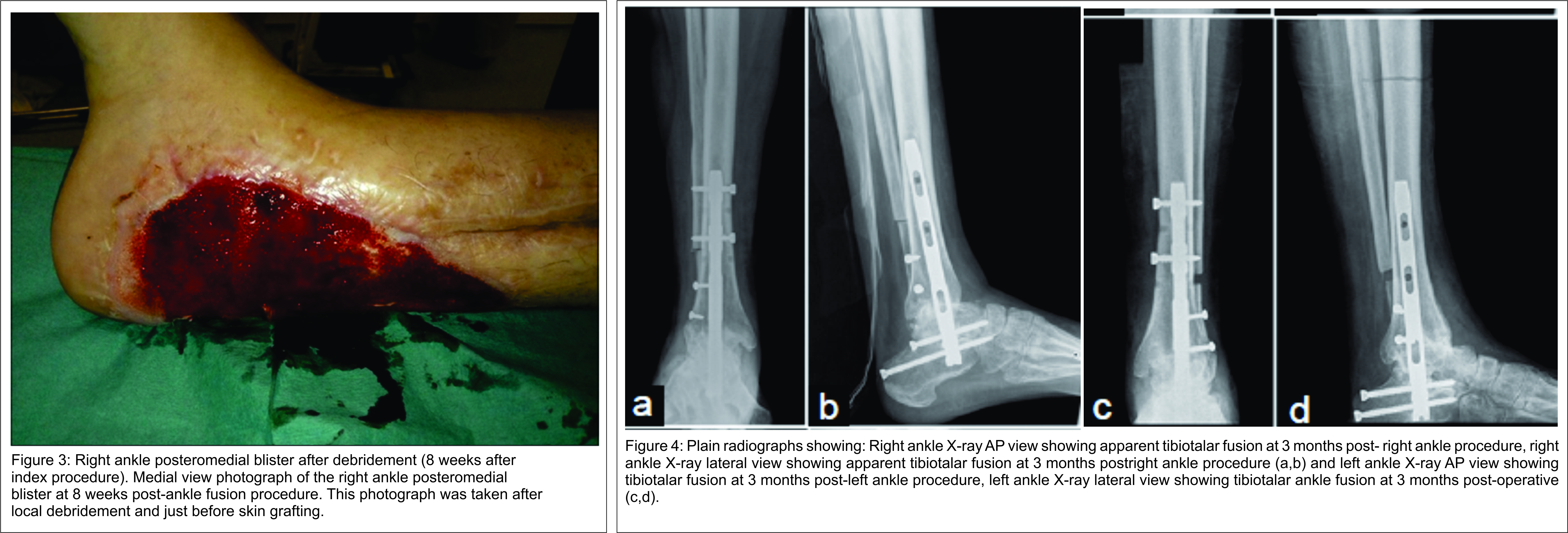
On examination, she presented a bilateral severe stiff equino-cavo-varus-adductus deformity with retraction due to subcutaneous and muscle scarring and neurological deficit. Claw hallux and lesser toes were also present bilaterally. Plantigrade weight bearing was not possible (Fig. 1). American Orthopaedic Foot and Ankle Society (AOFAS) score was 20 points. Plain radiographs showed bilateral equinovarus ankle deformity with supinated feet (Fig. 2). Achilles, posterior tibial, and flexor digitorum longus tendons lengthening were performed by medial approach associated to right tibiotalocalcaneal arthrodesis with a retrograde locked intramedullary nail (PANTA® – IntegraTM) by lateral approach. Distal fibula bone was used as an autograft. At 8 weeks of follow-up, plastic surgery applied a free skin graft over a persistent post-operative medial blister (Fig. 3). Apparent fusion was obtained at 3 months postoperatively (Fig. 4). At 6 months after the initial surgery, fusion surgery of the left ankle was performed in exactly the same fashion. As in the first procedure, clinical and radiological follow-up was done at 2, 6 weeks and every 3 months. Surgical wound dehiscence was the short-term complication and was resolved with dressing changes at 6 weeks post-operative. Fusion was obtained at 3 months postoperatively (Fig. 4).
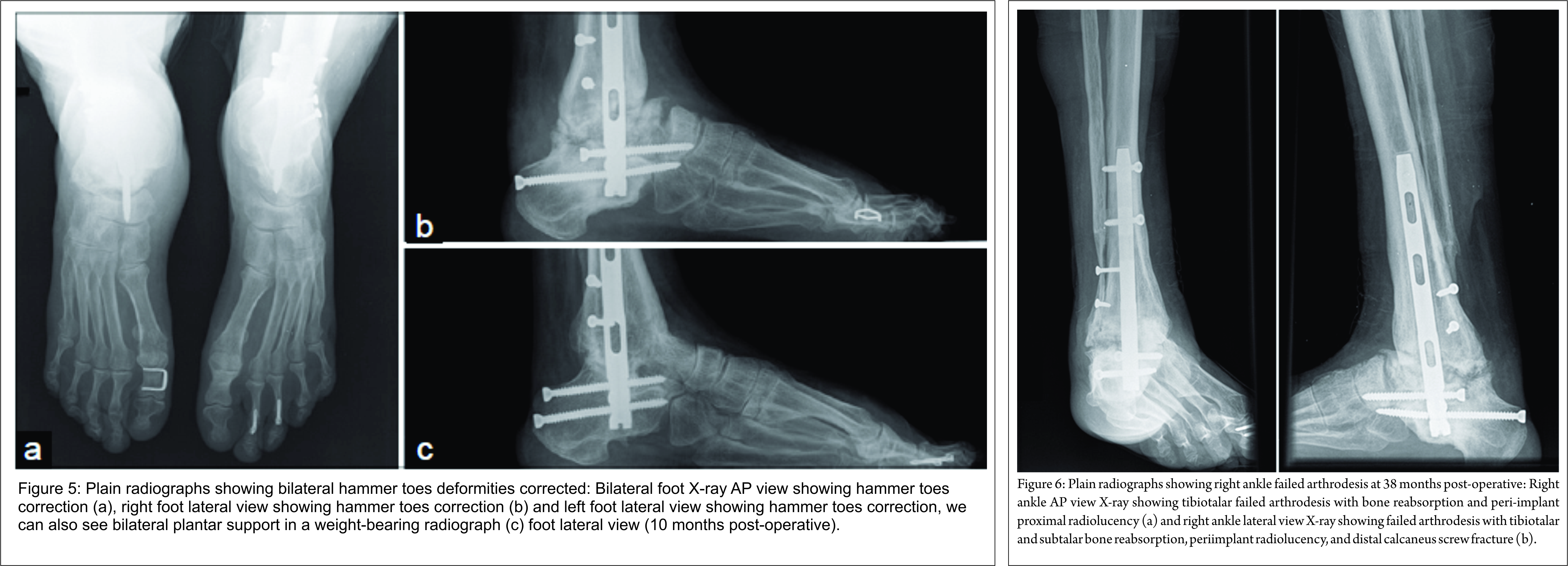
At 12 months after the first surgery, we documented recurrent dorsal proximal interphalangeal (PIP) joints inflammation with shoe wear. Right foot Moberg osteotomy, resection arthroplasty of PIP joints, and flexor tendon tenotomy of all the lesser toes were performed. Left foot Moberg osteotomy, PIP joints fusion of the 2nd and 3rd toes with intramedullary guide implant (Ipp-On® – IntegraTM), PIP joints resection arthroplasty of the 4th toe, and flexor tendon tenotomy of all the lesser toes were performed 14 months after the index surgery. Hardware-related pain caused Moberg osteotomy staple removal at 6 weeks post-operative (Fig. 5). The rehabilitation protocol included progressive weight-bearing with walking boots and lower limb drainage for 6 months. Prophylactic human immunoglobulin therapy was initiated after the last surgery. She regained walking capacity with balanced shoes and returned to work 4 months after left foot surgery. AOFAS score improved to 61 points. No toes related complaints, pressure ulcers or terminal necrosis of the toes were found. At 24 months after initial surgery, she complained of right ankle pain de novo with weight bear and local swelling. Radiologically, failed arthrodesis with tibiotalar and subtalar bone reabsorption, peri-implant proximal radiolucency, and distal calcaneus screw fracture were shown. No local drainage or blood test infection parameters were found. Only symptomatic treatment and nonsteroidal anti-inflammatory drugs were prescribed. At 38 months of follow-up, the patient refers no significant right ankle pain, and no SCLS attacks recurrence was registered (Fig. 6).
Discussion
This high-risk patients and the unpredictable course of the disease required a multidisciplinary treatment options discussion. The patient never accepted irreversible autonomy loss and was aware of all the possible negative surgery consequences when she signed the surgery consent. There are few treatment options for long-term sequelae of compartment syndrome that include arthroscopic assisted arthrodesis, fusion with an external fixator or internal devices such as plates or intramedullary nails. Arthroscopic arthrodesis is an excellent option when sparing the soft tissues is needed; however, this correction is limited to mild deformities. External fixation represents a serious risk of pin tract infection with no consensus about prevention treatment [8], and therefore we advocate as a potential risk for SCLS relapse. Fusion with plate and screws implies a considerable aggression to the already damaged soft tissues, although it represents a high stiffness construct. The authors managed this clinical case as an equino-varus-cavo-adductus deformity after lower extremity compartment syndrome. Retrograde nailing avoided extensive striping and Berend et al. have demonstrated better biomechanics stiffness compared to crossed screws [9]. Wang et al. [6] described excellent satisfaction rate after retrograde nailing for lower extremity compartment sequelae. No tendinous transfers were considered due to neurological deficit, scarred muscles, and stiff joints. Claw toes deformity has a high risk of pressure ulcers by shoe wear conflict. Local infection in SCLS patients may represent a potential trigger for relapse and therefore must be corrected. Considering the stiff interphalangeal joints, hallux claw deformity was managed by bilateral Moberg osteotomy. Lesser toes were addressed by resection arthroplasty of PIP joints with the exception of the stiffer left second and third toes that were fixated with an intramedullary guide implant [10]. Fusion rate of only 50% (1/2 ankles) was low compared to another published study that shows rates around 91% of the primary bony union after bilateral ankle arthrodesis. However, none of these patients had post compartment syndrome ankle deformity and related sequelae [11]. With no signs of infection, late failed arthrodesis may be related to compartment syndrome, local vascular and neurological damage, technical error or even SCLS per se. Three minor complications were registered. One large posteromedial blister required skin grafting 6 weeks after right ankle procedure. A left ankle lateral surgical wound dehiscence healed by secondary intention only with dressing changes. Failure of left hallux Moberg osteotomy staple was managed by hardware removal. These complications are relatively common and have been previously described in foot and ankle deformity correcting arthrodesis [6, 12]. They are usually due to poor skin and vascular conditions. No delayed weight bearing was noticed in rehabilitation program due to prompt and successful treatment. Concerning deformity correction, the results were very satisfactory. The AOFAS score increased from 20 to a total of 61 points even after tibiotalocalcaneal arthrodesis that does not allow any hind foot movement. Moreover, the painless plantar support permitted walking without crutches after 24 months confined to wheelchair. Returning to work was also an important milestone for this patient. At 38 months of follow-up, the patient is now asymptomatic with minor local right ankle edema and no walking limitation. Radiologically, the bone reabsorption appears to have stabilized (Fig. 6). Anecdotal evidence has shown good results in ankle arthrodesis revision after compartment syndrome [6]. However, one must consider unpredictable consequences of fusion revision in a SCLS patient, including a severe attack during the anesthesia or post-operative infection with potential lethal consequences. This patient has been diagnosed with idiopathic form of SCLS. Although no direct cause was identified, she had been taking azithromycin for a respiratory tract infection which may represent a potential trigger [4, 13]. Monoclonal gammopathy was also present at follow-up lab blood tests as seen in more than 90% of cases [2, 4]. There are several possible prophylactic treatments, which include B2-agonists, thalidomide, calcium channel blockers and chemotherapy with limited evidence considering the rarity of the disease. Intravenous immunoglobulin was administered in the past 12 months of follow-up with no relapses adding to the hypothesis that this may represent an effective prophylaxis [4, 14].
Limitations of the study
This study has several limitations: (1) It presents the results of only one patient and therefore lacks the ability to generalize, (2) low quality evidence-based knowledge about the syndrome and its treatment limits the possibility to establish cause-effect relationship, (3) we present a limited follow-up time of 38 months with a late failed arthrodesis that has not been reoperated yet, and (4) it is not possible to predict the result of right ankle failed arthrodesis revision.
Conclusion
Bilateral ankle fusion improved this SCLS patient functional outcome by restituting the walking capacity. One late failed arthrodesis was the major complication and may require a secondary procedure although the patient is currently asymptomatic. Four surgeries were performed with no SCLS attacks recurrence registered at 38 months follow-up period. Prophylactic human immunoglobulin may have contributed to the absence of relapses.
Although surgical correction of SCLS skeletal deformities sequelae represents an orthopedic challenge, we believe that this treatment should be considered in previously autonomous highly motivated active patients.
Clinical Message
SCLS is a rare condition that can lead to lower limb deformity, walk impairment and decreased quality of life. Although deformity correction surgery may represent life-threatening complications, life-changing results are possible and should be pursued.
References
1. Clarkson B, Thompson D, Horwith M, Luckey EH. Cyclical edema and shock due to increased capillary permeability. Am J Med 1960;29:193-216.1. Clarkson B, Thompson D, Horwith M, Luckey EH. Cyclical edema and shock due to increased capillary permeability. Am J Med 1960;29:193-216.
2. Atkinson JP, Waldmann TA, Stein SF, Gelfand JA, Macdonald WJ, Heck LW, et al. Systemic capillary leak syndrome and monoclonal IgG gammopathy; Studies in a sixth patient and a review of the literature. Medicine (Baltimore) 1977;56(3):225-239.
3. Sanghavi R, Aneman A, Parr M, Dunlop L, Champion D. Systemic capillary leak syndrome associated with compartment syndrome and rhabdomyolysis. Anaesth Intensive Care 2006;34(3):388-391.
4. Gousseff M, Arnaud L, Lambert M, Hot A, Hamidou M, Duhaut P, et al. The systemic capillary leak syndrome: A case series of 28 patients from a European registry. Ann Intern Med 2011;154(7):464-471.
5. Kyeremanteng K, D’Egidio G, Wan C, Baxter A, Rosenberg H. Compartment syndrome as a result of systemic capillary leak syndrome. Case Rep Crit Care 2016;2016:4206397.
6. Wang X, Ma X, Zhang C, Huang JZ, Gu XJ, Jiang JY. Ankle fusion with a retrograde locked intramedullary nail for sequela of lower extremity compartment syndrome. Chin J Traumatol 2012;15(3):140-144.
7. Lintz F, Colombier JA, Letenneur J, Gouin F. Management of long-term sequelae of compartment syndrome involving the foot and ankle. Foot Ankle Int 2009;30(9):847-853.
8. Jennison T, McNally M, Pandit H. Prevention of infection in external fixator pin sites. Acta Biomater 2014;10(2):595-603.
9. Berend ME, Glisson RR, Nunley JA. A biomechanical comparison of intramedullary nail and crossed lag screw fixation for tibiotalocalcaneal arthrodesis. Foot Ankle Int 1997;18(10):639-643.
10. Coillard JY, Petri GJ, van Damme G, Deprez P, Laffenêtre O. Stabilization of proximal interphalangeal joint in lesser toe deformities with an angulated intramedullary implant. Foot Ankle Int 2014;35(4):401-407.
11. Henricson A, Kamrad I, Rosengren B, Carlsson Å. Bilateral arthrodesis of the ankle joint: Self-reported outcomes in 35 patients from the Swedish ankle registry. J Foot Ankle Surg 2016;55(6):1195-1198.
12. Asomugha EU, Den Hartog BD, Junko JT, Alexander IJ. Tibiotalocalcaneal fusion for severe deformity and bone loss. J Am Acad Orthop Surg 2016;24(3):125-134.
13. Amoura Z, Papo T, Ninet J, Hatron PY, Guillaumie J, Piette AM, et al. Systemic capillary leak syndrome: Report on 13 patients with special focus on course and treatment. Am J Med 1997;103(6):514-519.
14. Marra AM, Gigante A, Rosato E. Intravenous immunoglobulin in systemic capillary leak syndrome: A case report and review of literature. Expert Rev Clin Immunol 2014;10(3):349-352.
 |
 |
 |
 |
 |
| Dr. Luis Filipe Loureiro Sobral | Dr. A C Ângelo | Dr. A Caetano | Dr. J Rodeia | Dr. I Rosa |
| How to Cite This Article: Sobral L, Ângelo AC, Caetano A, Rodeia J, Rosa I. Bilateral Ankle Fusion in Leak Syndrome Induced Deformity: A Case Report. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):52-56 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


