
[box type=”bio”] What to Learn from this Article?[/box]
Concomitant rotator cuff tears associated with shoulder dislocations are rare in young patients but must be considered when high-impact trauma is involved, and a trapped long head of biceps tendon lodged within the glenohumeral joint should be considered when there is failed closed reduction of a posterior dislocation.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 82-86| En Loong Soon, Hamid Rahmatullah Bin Abd Razak, Andrew Hwee Chye Tan. DOI: 10.13107/jocr.2250-0685.762
Authors: En Loong Soon[1], Hamid Rahmatullah Bin Abd Razak[1], Andrew Hwee Chye Tan[1]
[1] Department of Orthopaedic Surgery, Singapore General Hospital, Singapore.
Address of Correspondence
Dr. En Loong Soon,
1A, Pine Grove, #16-03, 590001, Singapore.
E-mail: enloong@gmail.com
Abstract
Introduction: Massive rotator cuff tears (RCTs) in the context of shoulder dislocations are relatively uncommon in the young adult (<40 years) and if reported are more commonly described in association with acute traumatic anterior glenohumeral dislocations. They have rarely been described with posterior dislocations, regardless of patient age. This is the 1st case reported in the context of posterior dislocations, where a triad of biceps tendon rupture, posterior dislocation, and RCTs was observed during surgery. It provides an important reminder to readers about certain injuries commonly overlooked during the assessment of an acute traumatic shoulder.
Case Report: We report an atypical case of a massive RCT involving a 34-year-old Asian male who landed on his outstretched hand after falling off a bicycle. A tear involving the supraspinatus and subscapularis was visualized during surgery, along with long head of biceps (LHB) tendon rupture. This was after an initial failure to achieve closed reduction of the posteriorly dislocated left shoulder.
Conclusion: It is easy to miss the posterior instability, the associated RCTs or the biceps tendon injuries. Biceps tendon rupture should be a consideration when one is unable to reduce a posteriorly dislocated shoulder. The interposed torn LHB tendon trapped within the glenohumeral joint was the likely physical block in the initial failure to achieve closed reduction. With timely diagnosis, prudent physical examination, early imaging and surgery, and excellent results can potentially be achieved to return a young patient to full functionality.
Keywords: Biceps tendon rupture, massive rotator cuff tear, posterior shoulder dislocation, failure of closed reduction.
Introduction
Posterior shoulder dislocations result from axial loading of an adducted and internally rotated arm, violent muscle contractions resulting from fits or electrocution, or a posterior force applied directly to the anterior shoulder [1]. They are uncommon injuries, representing only 1-4% of all shoulder dislocations [2]. Massive rotator cuff tears (RCTs) are more commonly known to occur with traumatic anterior glenohumeral dislocations in patients older than 40 years of age [1, 3, 4], usually an elderly female who falls on her outstretched hand [4] or the very occasional young patient [5]. They rarely occur with posterior glenohumeral dislocations, regardless of patient age. There has only been one documented case involving a posteriorly subluxed shoulder and five involving posterior dislocated shoulders [2, 6, 7]. This case report is the first that describes a massive RCT occurring in conjunction with a posteriorly dislocated shoulder and a long head of biceps (LHB) tendon tear. Due to its rarity, sparse evidence exists to suggest when to suspect the condition and what dictates appropriate treatment [2]. In view of scarce existing literature pertaining to associations between these three injuries, we document a patient’s journey from diagnosis to surgery and recovery.
Case Report
A 34-year-old male, helmeted cyclist moving at approximately 10-20 mph sustained an injury of his left shoulder as he sought to break a fall with an outstretched upper extremity. The main symptoms initially described were pain and weakness in his left shoulder resulting in worsening range of motion. He struggled to complete various basic activities of daily living such as bathing or dressing, and hence visited our clinic 3 days later. Initial radiographs (anteroposterior (AP), lateral Y scapula view and axillary views) were all obtained (Fig. 1), with the diagnosis of posterior glenohumeral dislocation clinched after posterior instability was suspected clinically. Magnetic resonance imaging (MRI) of the shoulder was subsequently performed and further demonstrated a massive RCT with posterior dislocation.
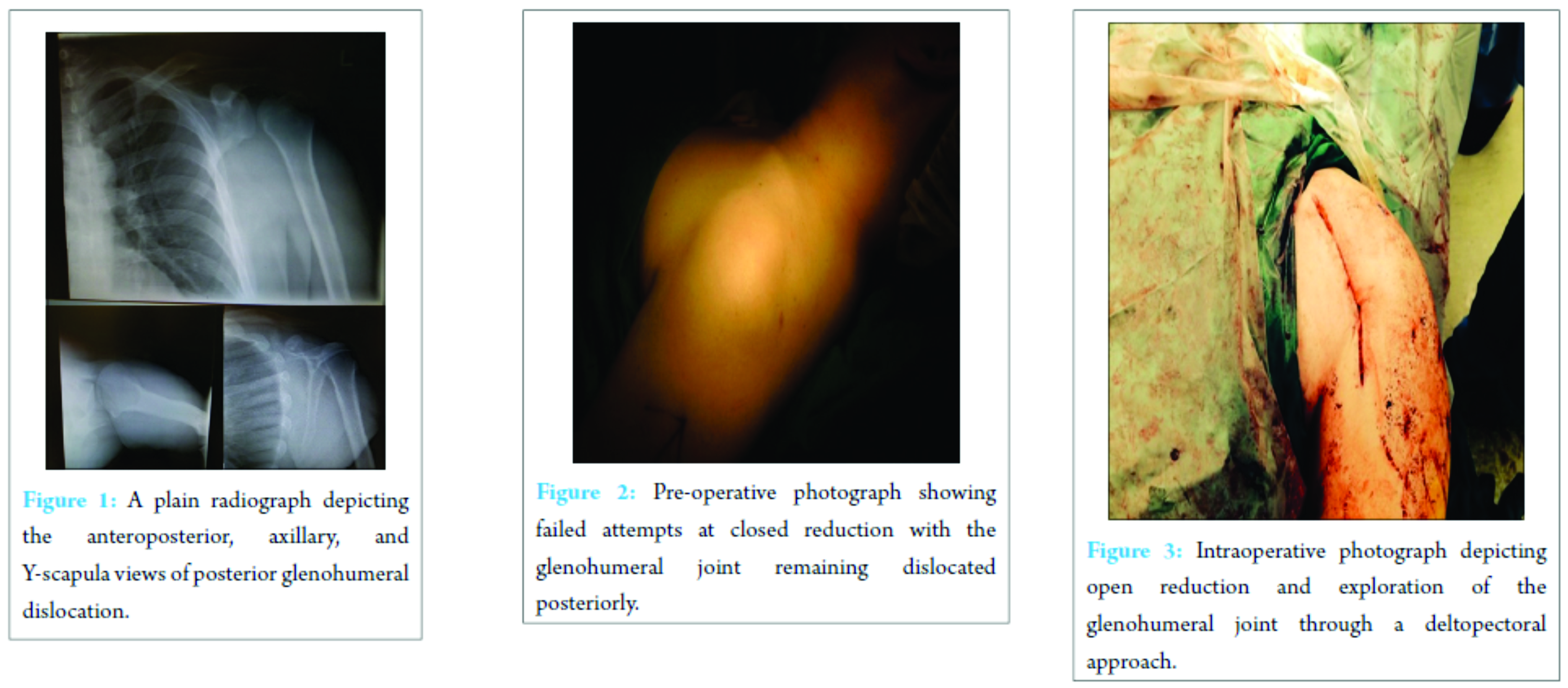
Surgical manipulation and operative treatment
A decision was made to proceed with open reduction through a deltopectoral approach because initial closed manipulation was unsuccessful (Fig. 2 and 3). Exploration of the region revealed a massive full-thickness RCT involving both the supraspinatus and subscapularis tendons, with the glenohumeral capsule avulsed from the humeral head (Fig. 4). The teres minor and infraspinatus tendons were intact. A very significant intraoperative observation was an LHB tear, trapped and interposed within the glenohumeral joint (Fig. 5). This was the most likely impediment to initial closed reduction. The torn subscapularis tendon was mobilized, and a secondary approach through the anterior deltoid raphe to visualize and mobilize the supraspinatus tendon was adopted. The supraspinatus and subscapularis were repaired with two and three 4.5 mm suture anchors, respectively (Fig. 6). As the LHB was torn too proximally, the decision was made not to reattach it to the humerus with tenodesis. The surgical site was thoroughly irrigated with adequate wound closure and antibiotic/analgesia cover to minimize infection.
Post-operative recovery
The patient was placed in an external rotation sling with his arm in neutral and specifically instructed not to move his arm or engage in physiotherapy for fear of a retear of his rotator cuff. 2-week post-operatively, his range of motion was 90° of passive flexion as compared to 180° in the opposite shoulder, with the wound well healed and the shoulder stable. The patient was advised to start engaging in gentle passive pendulum exercises but was still kept in the external rotation sling. 6-week post-operatively, pain and stiffness were significantly diminished, with much improved rotator cuff strength compared to the opposite shoulder. He was encouraged to start engaging in full active range of motion exercises and physiotherapy. 6-month post-operatively, the patient was fully recovered with full range of motion and strength (5/5 on Medical Research Council [MRC] grading scale) in terms of internal and external rotation, abduction, flexion, and extension compared to the opposite shoulder (Fig. 7).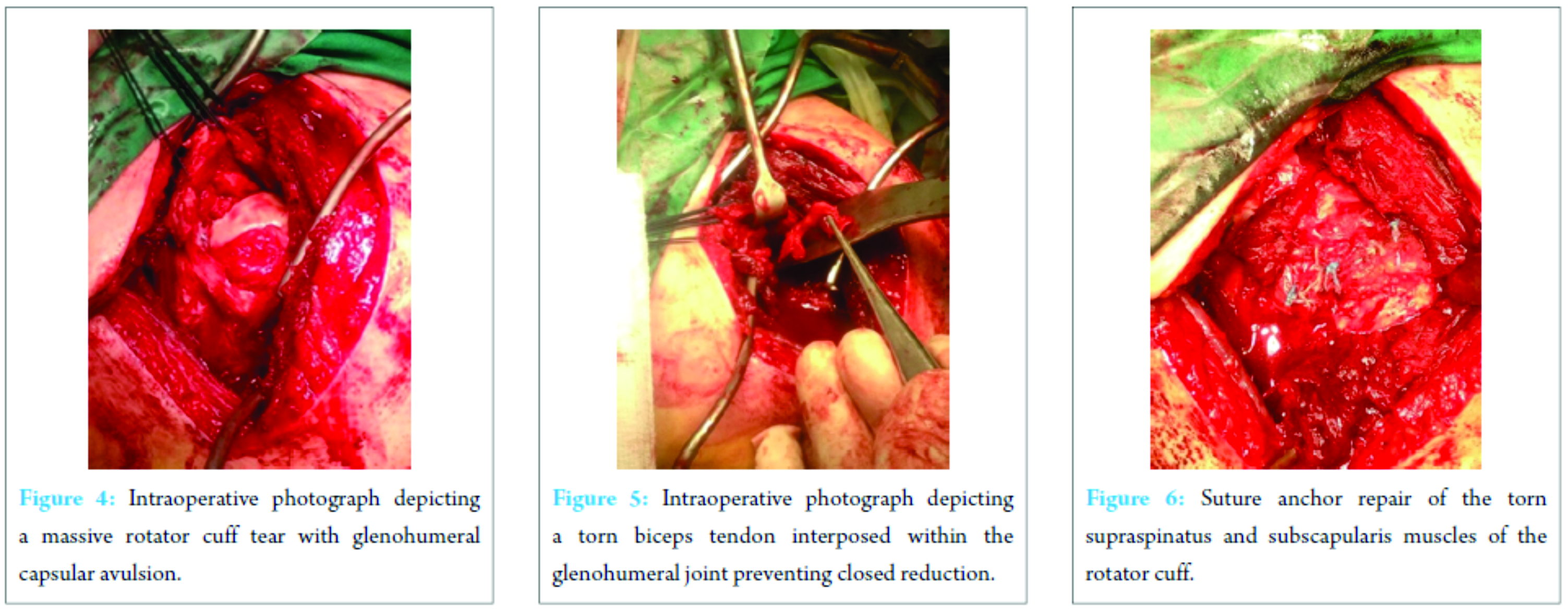 At 2-year post-surgery, the patient was noted to have recovered fully with a return to pre-injury activity levels and did not exhibit any symptoms or signs of instability. Range of motion of the affected shoulder was full at 180° of flexion (180° in the opposite shoulder), 40° of extension (40° in the opposite shoulder), 160° of abduction (165° in the opposite shoulder), 80° of external rotation (80° in the opposite shoulder), and 60° of internal rotation (60° in the opposite shoulder). Power grading was MRC 5/5 in both shoulders for flexion, extension, abduction, and internal and external rotation.
At 2-year post-surgery, the patient was noted to have recovered fully with a return to pre-injury activity levels and did not exhibit any symptoms or signs of instability. Range of motion of the affected shoulder was full at 180° of flexion (180° in the opposite shoulder), 40° of extension (40° in the opposite shoulder), 160° of abduction (165° in the opposite shoulder), 80° of external rotation (80° in the opposite shoulder), and 60° of internal rotation (60° in the opposite shoulder). Power grading was MRC 5/5 in both shoulders for flexion, extension, abduction, and internal and external rotation.
Discussion
Reports of traumatic massive RCTs in young adults exist in very small numbers in literature [7]. Cuff tears in the young are usually partial thickness tears or contusions due to chronic overuse in athletes [7]. A massive RCT, in the context of dislocations and trauma, is more often seen in older patients, who may already have frail rotator cuff muscles due to overuse. Lin suggests that the injury preceding full-thickness RCTs in young, high-demand patients is usually high-energy trauma [8], with the few studied being associated with anterior dislocations.
Characteristics and features of a posterior shoulder dislocation and its associated injuries
Massive RCTs associated with posterior dislocation/subluxations in young people (<40 years old) are even more uncommon. Typical pathologic findings seen on MRI after an acute traumatic posterior shoulder dislocation are tearing or shredding of the posterior labrum [9], which is termed a reverse Bankart lesion [10]. Damage to other posterior supporting structures is considered uncommon [11]. In terms of diagnosis, a widened joint space and a lack of overlap between the glenoid and humeral head can be appreciated on the AP X-ray projection (Fig. 1), with the shoulder rotated such that the humeral head has a characteristic light bulb appearance. Axillary and Y-scapula views are, especially, valuable in demonstrating the relationship between the glenoid and the humeral head as subtle posterior subluxations can be missed in the absence of frank dislocations. Common injuries associated with posterior dislocations such as a fractured posterior glenoid rim, humeral shaft, head, and tuberosity or the “reverse Hill-Sachs lesion/reverse Bankart” which one should be aware of were not present in this case.
Diagnosing and managing RCTs in posterior shoulder dislocations
Arun concludes that the pertinent finding that should raise an examiner’s index of suspicion for concomitant massive RCTs is persistent severe pain after reduction of a dislocation [2]. Goubier et al. suggest that the failure of abduction post-reduction should be considered as a red flag for potential rotator cuff rupture [12]. Young patients demonstrate a particular need for prompt diagnosis, given the dire consequences of both long- and short-term disabilities if the tears are not adequately managed [13]. Robinson et al. proposed that surgeons should lower their threshold for performing early ultrasounds or MRIs if RCTs were suspected, despite a much-decreased prevalence of these injuries among young patients [10, 14]. In terms of treatment, the young patient have several mechanical and biological traits which increase the probability of a successful rotator cuff repair, likely due to superior vascular supply and tendon quality. Krishnan et al. explained that in patients younger than 40 years old with traumatic RCTs, repairs culminated in excellent relief of pain and recovery of pre-injury functional levels [15]. Lazarides et al. further elaborated that these good outcomes were similar in both open and arthroscopic repairs in terms of pain relief and self-reported outcome scores post-operatively [13]. Incarcerated LHB tendon resulting in locked posterior dislocations We postulate that the interposed torn LHB could have resulted in the initial failure to achieve closed reduction. This has not been reported in literature pertaining to posterior dislocations to date and should perhaps be a consideration when one is unable to achieve closed reduction (locked posterior dislocation) in an acute traumatic setting. While we proceeded with open glenohumeral arthrotomy and repair of the structures, there may also be a role for arthroscopic evaluation although this would be extremely challenging in a subluxed or dislocated joint.
Conclusions
We present this atypical case of a traumatic posterior shoulder dislocation with associated massive RCT and LHB tear in a young patient. Like other uncommon conditions, these injuries can easily be missed if not suspected. Careful clinical assessment to look for rotator cuff injuries and shoulder instability should be performed in conjunction with early radiological investigations, especially in young patients who present with high impact injuries. Failure of closed reduction of a posterior dislocation could also point to the possibility of a torn LHB tendon being incarcerated and trapped within the joint. This has not been described before in the context of posterior dislocations. With timely diagnosis, prudent physical examination, imaging and surgery, and excellent results can potentially be achieved to return young patients who present with similar injuries to full functionality.
Clinical tip
The possibility of an incarcerated LHB should therefore be a consideration for clinicians having difficulties reducing and managing posteriorly dislocated shoulder joints, during surgical planning for open reduction.
Clinical Message
Clinicians should always be aware of the possibility of rotator cuff tears in young patients who sustain posterior dislocations. If there is failed closed reduction of a posterior dislocation, a trapped long head of biceps tendon lodged within the glenohumeral joint should also be a consideration.
References
1. Schoenfeld AJ, Lippitt SB. Rotator cuff tear associated with a posterior dislocation of the shoulder in a young adult: A case report and literature review. J Orthop Trauma 2007;21(2):150-152.1. Schoenfeld AJ, Lippitt SB. Rotator cuff tear associated with a posterior dislocation of the shoulder in a young adult: A case report and literature review. J Orthop Trauma 2007;21(2):150-152.
2. Arun G. Concurrent shoulder dislocation with rotator cuff tear and coracoid process fracture. MOJ Orthop Rheumatol 2015;2(2):45.
3. Luenam S, Kosiyatrakul A. Massive rotator cuff tear associated with acute traumatic posterior shoulder dislocation: Report of two cases and literature review. Musculoskelet Surg 2013;97(8):273-278.
4. Atef A, El-Tantawy A, Gad H, Hefeda M. Prevalence of associated injuries after anterior shoulder dislocation: A prospective study. Int Orthop 2016;40(3):519-524.
5. Throckmorton T, Albright J. Case report: Concurrent anterior shoulder dislocation and rotator cuff tear in a young athlete. Iowa Orthop J 2001;21:76-79.
6. Moeller JC. Compound posterior dislocation of the glenohumeral joint. Case report. J Bone Joint Surg Am 1975;57(7):1006-1007.
7. Turman KA, Anderson MW, Miller MD. Massive rotator cuff tear in an adolescent athlete: A case report. Sports Health 2010;2(1):51-55.8. Lin YP, Huang TF, Hung SC, Ma HL, Liu CL. Rotator cuff tears in patients younger than 50 years of age. Acta Orthop Belg 2012;78(5):592-596.
9. Bhatia DN, de Beer JF, van Rooyen KS, du Toit DF. The reverse terrible triad of the shoulder: Circumferential glenohumeral musculoligamentous disruption and neurologic injury associated with posterior shoulder dislocation. J Shoulder Elbow Surg 2007;16(9):e13-e17.
10. Steinitz DK, Harvey EJ, Lenczner EM. Traumatic posterior dislocation of the shoulder associated with a massive rotator cuff tear: A case report. Am J Sports Med 2003;31(6):1010-1012.
11. Hottya GA, Tirman PF, Bost FW, Montgomery WH, Wolf EM, Genant HK. Tear of the posterior shoulder stabilizers after posterior dislocation: MR imaging and MR arthrographic findings with arthroscopic correlation. AJR Am J Roentgenol 1998;171(3):763-768.
12. Goubier JN, Duranthon LD, Vandenbussche E, Kakkar R, Augereau B. Anterior dislocation of the shoulder with rotator cuff injury and brachial plexus palsy: A case report. J Shoulder Elbow Surg 2004;13(3):362-363.
13. Lazarides AL, Alentorn-Geli E, Choi JH, Stuart JJ, Lo IK, Garrigues GE, et al. Rotator cuff tears in young patients: A different disease than rotator cuff tears in elderly patients. J Shoulder Elbow Surg 2015;24(11):1834-1843.
14. Robinson CM, Shur N, Sharpe T, Ray A, Murray IR. Injuries associated with traumatic anterior glenohumeral dislocations. J Bone Joint Surg Am 2012;94(1):18-26.
15. Krishnan SG, Harkins DC, Schiffern SC, Pennington SD, Burkhead WZ. Arthroscopic repair of full-thickness tears of the rotator cuff in patients younger than 40 years. Arthroscopy 2008;24(3):324-328.
 |
 |
 |
| Dr. En Loong Soon | Dr. Hamid Rahmatullah Bin Abd Razak | Dr. Andrew Hwee Chye Tan |
| How to Cite This Article: Soon EL, Razak HRBA, Tan AHC. A Rare Case of Massive Rotator Cuff Tear and Biceps Tendon Rupture with Posterior Shoulder Dislocation in a Young Adult – Surgical Decisionmaking and Outcome. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):82-86 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


