
[box type=”bio”] What to Learn from this Article?[/box]
In patient with osteoporotic bone undergoing total hip arthroplasty, it is important to monitor patients for post‑operative stress fractures. These patients may have an atraumatic onset of persistent pain and should have radiographs and possibly CT scans to evaluate for potential stress fractures.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 87-89| Oluwaseun Akinbo, Vineet Tyagi. DOI: 10.13107/jocr.2250-0685.764
Authors: Oluwaseun Akinbo[1], Vineet Tyagi[2]
[1] Department of Orthopaedics, Yale-New Haven Hospital, New Haven, CT, USA, 2Department of Orthopaedics and Rehabilitation, Yale School of Medicine, New Haven, CT, USA.
Address of Correspondence
Dr. Vineet Tyagi,
47 College Street, New Haven, CT, USA.
E-mail: vineet.tyagi@yale.edu
Abstract
Introduction: Acute hip pain following total hip arthroplasty (THA) could have numerous causes to include stress fracture of the pelvis. Stress fractures of the pelvis are rare and have been reported to involve the medial wall and the pubic ramus. A unique case is presented demonstrating the clinical presentation and management of an acute stress fracture of ilium and anterior column following a THA.
Case Report: A 72-year-old man underwent an uncomplicated right THA. He was noted to have femoral head resorption and thin osteoporotic bone intraoperatively. He initially did well postoperatively and ambulating without pain or assistive devices. Within 1 month of surgery, he returned with acute right hip pain without any traumatic event. Radiographs showed migration of the acetabular component and computed tomography scan confirmed a fracture through the ilium. The patient underwent revision surgery, where the fracture was reduced and internal fixation was achieved with a reconstruction plate and acetabular cage construct. At 9 months postoperatively, the patient remained pain-free with full weight bearing and with stable radiographs.
Conclusion: Elderly patients who undergo THA may have low bone mineral density. These patients can develop stress fractures in their pelvis after surgery. These fractures may involve the medial wall, posterior column, or posterior wall. In patients who develop atraumatic pain postoperatively, it is important to consider for potential stress fractures of the ilium and evaluate appropriately with imaging. In these cases, revision surgery can be necessary to provide fixation of the stress fracture.
Keywords: Stress fracture, total hip arthroplasty, periprosthetic fracture, acetabulum, pelvis, pelvic.
Introduction
Acute hip pain following total hip arthroplasty (THA) is typically unusual, and the onset of pain related to a recent increase in activity should raise suspicion for stress fractures [1]. Stress fractures following a THA are rare and have been reported to involve the pubis, the medial wall, the posterior wall, and posterior column [1, 2, 3, 4, 5]. To our knowledge, this is the only report in the literature of a patient who suffered from a stress fracture of the ilium and anterior column following a THA.
Case Report
A 72-year-old man presented with symptoms of end-stage degenerative changes of his right hip. Right THA was performed. Intraoperatively, it was noted that the patient’s femoral head was resorbed, his bone was significantly osteopenic and thin, and he had a loss of his abductor tendons. He was noted to have a defect in the posterior wall of his acetabulum likely from impingement of his femoral neck on the acetabulum. He did not have a prior history of rheumatoid arthritis or osteoporosis. The acetabulum was inspected after preparation and before prosthesis implantation and no fractures were identified. Frozen sections were taken and were negative for infection. Intraoperatively, the cup did not have a great press-fit; the acetabulum was examined, and no fracture could be identified. As such, a cup was implanted and fixed with three screws. The lack of abductors was compensated for by constructing a tripolar construct – bipolar head on lateralized and anteverted polyethylene liner in acetabular component (Fig. 1).
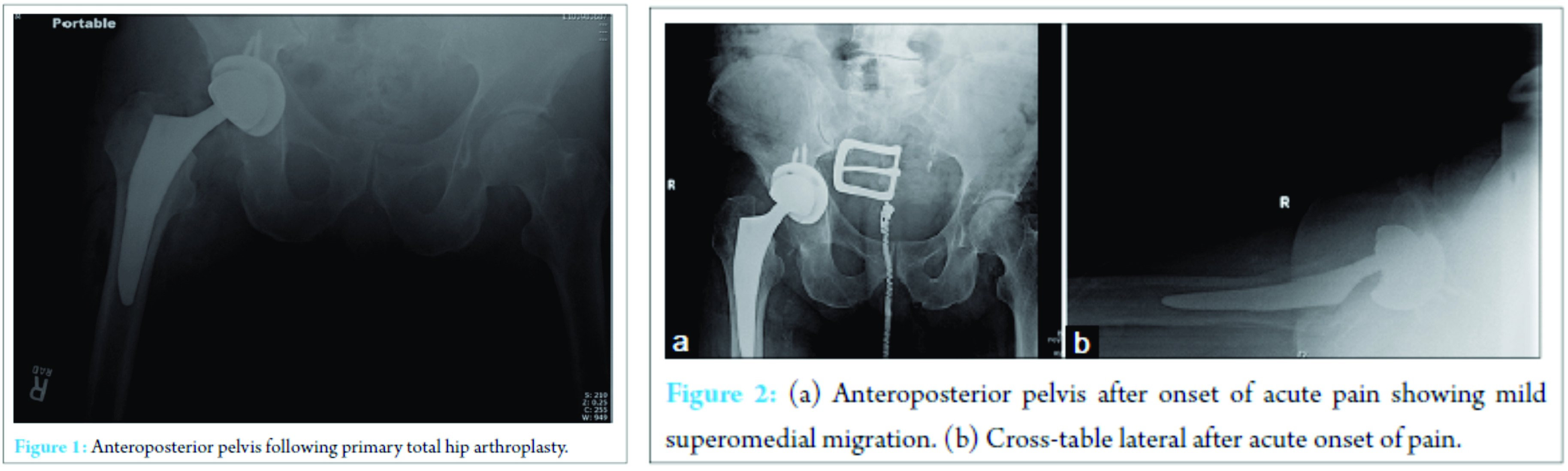
The patient’s post-operative course was uneventful and he was discharged accordingly. He was ambulating comfortably and transitioned away from the use of his assistive device. However, 1 month later, he presented with acute and worsening right hip pain with ambulation. There was no inciting event. Radiographs obtained suggested mild superomedial migration of the acetabular component (Fig. 2a and b). He was diagnosed with a presumed insufficiency fracture. Weight bearing was immediately restricted. He subsequently dislocated the THA construct (Fig. 3a and b), and was closed reduced in the emergency room. Computed tomography scan was obtained. This confirmed a fracture through the ilium just above the acetabulum, and superomedial migration of the acetabular component through the anterior column (Fig. 4a-d).
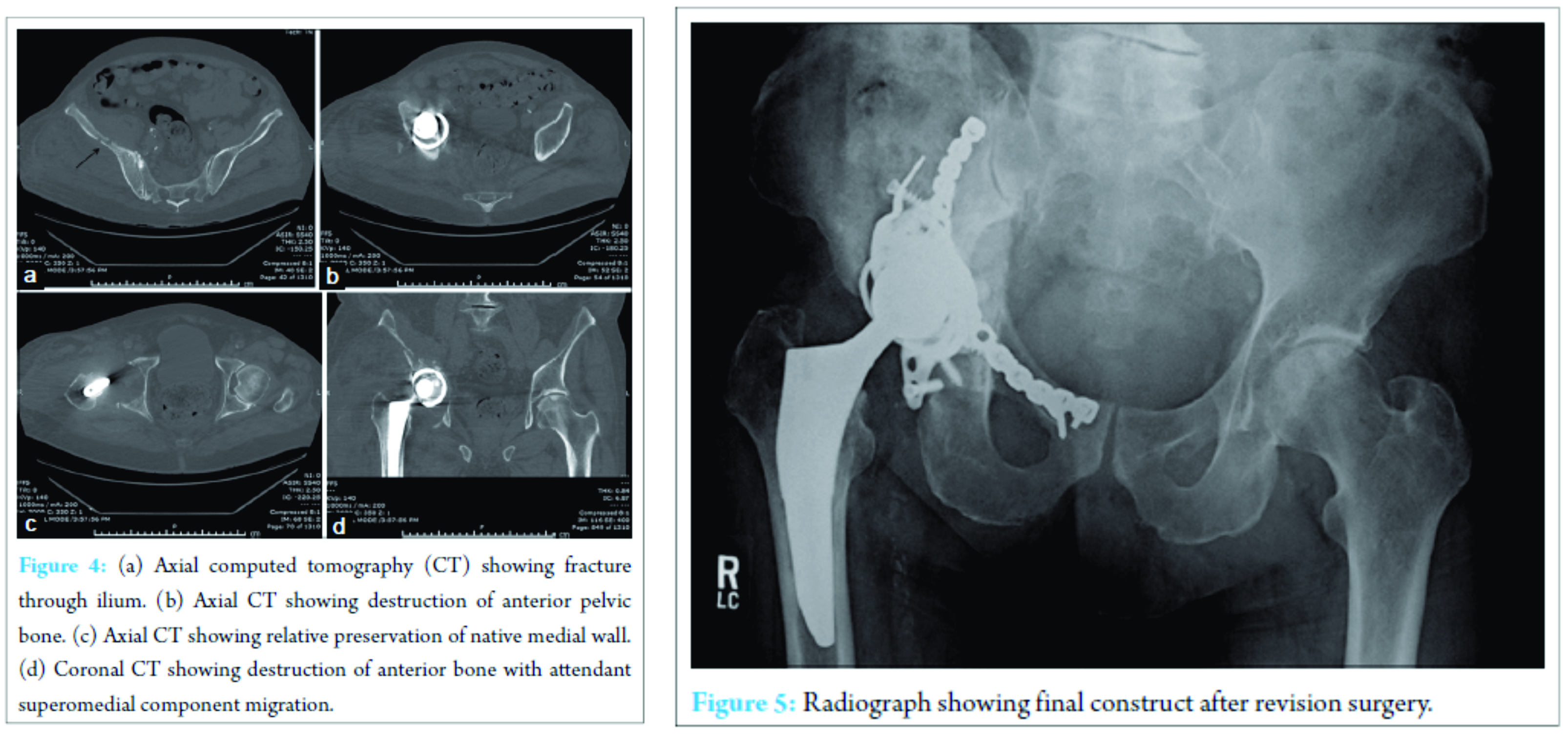
A revision was planned and performed with an acetabular trauma surgeon. The anterior pelvic fracture was approached anteriorly and bridged with a 3.5 reconstruction plate. There was significant comminution noted with a large anterior column defect. The hip arthroplasty was then exposed via an extensile posterior approach. The femoral component was well fixed. The pelvic defect was grafted through the acetabulum with a femoral head allograft. A reconstruction cage was then implanted and fixed to the pelvis with multiple screws. A constrained liner was then cemented in place. Intraoperative cultures were negative. The patient was non-weight bearing for 3 months. He, unfortunately, developed a post-operative hematoma with wound drainage and was returned to the operating room 12 days later for an aggressive irrigation and debridement with retention of components. Intraoperative cultures grew methicillin-resistant Staphylococcus aureus and Enterococcus species. He was appropriately treated with intravenous antibiotics. At his most recent follow-up 9 months postoperatively, he was ambulating with a cane, without pain of functional issues. He reported some residual subjective weakness but had 5/5 hip flexion strength and stable radiographs (Fig. 5).
Discussion
Pentecost describes a stress fracture as one that results from the inherent inability of bone to withstand stress applied without violence in a rhythmical, repeated, and subthreshold manner [6]. Stress fractures can be classified as fatigue fractures which occur when abnormal stress is applied to normal bone; insufficiency fractures which occur when normal or physiological stress is applied to deficient bone. Pathologic fractures are fractures in bone weakened by tumor [6]. In this case, our patient sustained an insufficiency fracture. He was ambulating without difficulty and pain postoperatively, and then acutely developed pain without any trauma or inciting event. This fracture likely happened because the patient’s osteoporotic bone was subjected to a more significant stress level than it had been preoperatively. It is unclear what impact implanting a tripolar component had on the development of his stress fracture. It is possible that this fracture could have been prevented if the patient’s weight bearing status had been gradually advanced over time as opposed to immediate full weight bearing following surgery. This complication could have been anticipated given the osteoporotic nature of his bone at time of initial surgery as osteoporosis is a significant risk factor for stress fractures. During surgery in patients with osteoporotic bone, care must be taken to avoid creating stress risers or intraoperative fractures; forceful acetabular shell impaction for great acetabular component press-fit should be done with care. If press-fit is not good (i.e. the cup not stable), but the acetabular preparation is appropriate and the component well seated, adjunct fixation with screws should be considered rather than continued forceful impaction. Stress fractures of the acetabulum can be managed conservatively with anti-inflammatory medications and restricted weight bearing [1, 5]. However, the patient in this case ultimately underwent surgical management because of the bony destruction of the pelvis, and component migration. Column destruction, pelvic discontinuity, and component migration should prompt consideration of surgical management of pelvic stress fractures. It may be necessary in certain cases to address these cases as a joint case between an arthroplasty surgeon and an acetabular trauma surgeon [7]. To our knowledge, this is the first reported case of an acute stress fracture of the ilium and anterior column following a THA.
Clinical Message
It is important to monitor THA patients postoperatively for signs of stress fractures. Although iatrogenic fractures may occur intraoperatively, stress fractures can also occur postoperatively. These patients may have an atraumatic onset of persistent pain and should have radiographs and possibly CT scans to evaluate for potential stress fractures.
References
1. Andrews P, Barrack RL, Harris WH. Stress fracture of the medial wall of the acetabulum adjacent to a cementless acetabular component. J Arthroplasty 2002;17(1):117-120.1. Andrews P, Barrack RL, Harris WH. Stress fracture of the medial wall of the acetabulum adjacent to a cementless acetabular component. J Arthroplasty 2002;17(1):117-120.
2. McElfresh EC, Coventry MB. Femoral and pelvic fractures after total hip arthroplasty. J Bone Joint Surg Am 1974;56(3):483-492.
3. Chatoo M, Parfitt J, Pearse MF. Periprosthetic acetabular fracture associated with extensive osteolysis. J Arthroplasty 1998;13(7):843-845.
4. Smith D, Zuckerman JD. Bilateral stress fractures of the pubic rami following THA – An unusual case of groin pain. Bull NYU Hosp Jt Dis 2010;68(1):43-45.
5. Kanaji A, Ando K, Nakagawa M, Fukaya E, Date H, Yamada H. Insufficiency fracture in the medial wall of the acetabulum after total hip arthroplasty. J Arthroplasty 2007;22(5):763-767.
6. Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA 1964;187:1001-1004.
7. Chitre A, Jones HW, Shah N, Clayson A. Complications of total hip arthroplasty: Periprosthetic fracture of the acetabulum. Curr Rev Musculoskelet Med 2013;6(4):357-363.
 |
 |
| Dr. Oluwaseun Akinbo | Dr. Vineet Tyagi |
| How to Cite This Article: Akinbo O, Tyagi V. Acute Stress Fracture of the Pelvis after Total Hip Arthroplasty: A Case Report. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):87-89. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


