
[box type=”bio”] What to Learn from this Article?[/box]
Patients with kissing lesions of the knee can be treated successfully with autologous chondrocyte implantation performed to multiple sites.
Case Report | Volume 7 | Issue 3 | JOCR May – June 2017 | Page 41-44| Taylor J Ridley, Christopher T Rud, Jeffrey A Macalena. DOI: 10.13107/jocr.2250-0685.798
Authors:
[1] Department of Orthopaedic Surgery, University of Minnesota, 2450 Riverside Avenue South, Suite R200, Minneapolis, MN 55454, USA.
[2] Department of Orthopaedic Surgery, College of Osteopathic Medicine, Marian University, Indianapolis, IN 46222, USA.
Address of Correspondence
Dr. Jeffrey A Macalena,
Department of Orthopaedic Surgery, University of Minnesota,
2450 Riverside Avenue South, Suite R200, Minneapolis, MN 55454, USA.
E-mail: maca0049@umn.edu
Abstract
Introduction: Autologous chondrocyte implantation (ACI) is an effective treatment for chondral defects of the knee; however, its use in kissing lesions is less well documented.
Case Report: A 23-year-old female with a kissing lesion of the patellofemoral compartment on magnetic resonance imaging underwent two-stage ACI to her medial patella (20 mm × 22 mm) and medial trochlea (27 mm × 18 mm). At 1-year follow-up, the patient had returned to all activities with near-complete resolution of symptoms and substantial improvement in clinical outcome scores.
Conclusion: Patients with kissing lesions of the knee can be treated successfully with ACI performed to multiple sites.
Keywords: Chondral defect, knee, kissing lesion, chondroplasty, autologous chondrocyte implantation.
Introduction
Full-thickness chondral kissing lesions have been documented in young patients, but the varying treatment modalities remain controversial. Studies have shown that articular cartilage lesions are prevalent in the knee joints of young, active persons, with the prevalence of chondral lesions found during knee arthroscopy ranging from 60% to 66% [1, 2, 3]. In a study of 993 knee arthroscopies, full-thickness lesions suitable for cartilage repair procedures were found in 11% of patients [1]. In one study, the prevalence of kissing lesions was found to be 6.3%, with half of these associated with concomitant anterior cruciate ligament (ACL) tears [4]. Current treatments for isolated osteochondral defects include microfracture, osteochondral autograft transfer (OAT), autologous chondrocyte implantation (ACI), osteochondral allograft, and unicompartmental arthroplasty. Treatment of osteochondral kissing lesions with ACI is an established treatment; however, the results have been less favorable than that of single isolated lesions [5, 6, 7]. In addition, studies have previously excluded ACI as a treatment for kissing lesions [8]. We present a case of a kissing lesion in the knee treated successfully with ACI evaluated at 36-month follow-up with pre- and post-operative outcome scores.
Case Report
A 23-year-old female presented with an extensive right knee history, including allograft ACL reconstruction 9 years before presentation, with subsequent graft failure and revision ACL reconstruction with bone-patellar tendon-bone autograft 7 years prior. On initial presentation, the patient complained of pain and crepitation anteriorly in her knee. Her pain was worse with stairs and worse after sitting for prolonged periods. The patient also endorsed catching, but stated that no frank locking of her knee had occurred. Clinical examination revealed Lachman of 1A and no pivot shift. Marked tenderness to palpation was present over the medial patellar facet and trochlear groove. Patellar grind test was positive and loading of the patella recreated her primary complaint of anterior knee pain as well as produced marked patellofemoral crepitus. Magnetic resonance imaging showed full-thickness cartilage loss covering the majority of the medial patellar facet, with full-thickness cartilage loss along the medial aspect of the trochlea (Fig. 1). A two-stage reconstruction of her cartilage was planned. Initially, the patient underwent arthroscopic chondroplasty of the patellofemoral compartment and Carticel® (Aastrom Biosciences, Ann Arbor, MI) biopsy was obtained. Arthroscopy revealed a near full-thickness (Grade III) chondral defect of the medial patellar facet measured 15 mm × 10 mm. Evaluation of the trochlea showed a 20 mm × 10 mm area of Grade III and IV cartilage loss. The lateral trochlea was intact. A second Grade IV defect of the medial trochlea was noted that measured 8 mm × 15 mm. This was separated from the other defect by a thin rim of Grade II chondrosis. The medial and lateral femoral condyles and tibial plateau showed largely intact chondral surfaces with just some Grade I softening (Fig. 2). The patient was allowed to bear weight as tolerated and to initiate motion exercises when able. Running, jumping, and return to sports were limited for 6 weeks. At 6-week post-surgery, the patient denied noticeable improvement in her symptoms. Subsequent open ACI implantation (second generation with Type I/III bilayer collagen membrane [Bio-Gide®, Getistlich Pharma North America Inc., Princeton, NJ]) was performed. At the time of implantation, the defect of her medial patella facet measured 20 mm × 22 mm while the medial trochlea measured 27 mm × 18 mm. Both defects were combined creating a single lesion (Fig. 3).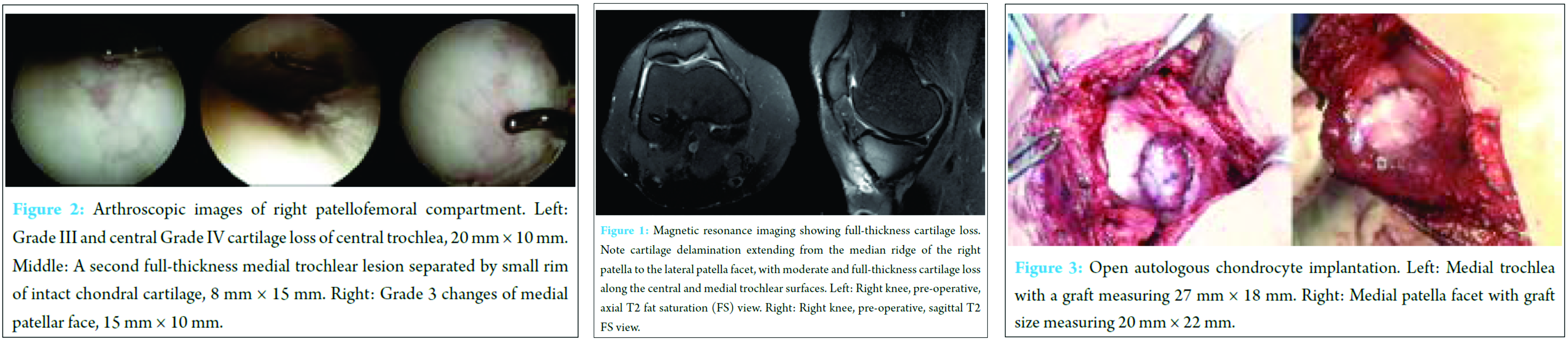
Postoperatively, the patient was made toe-touch weight bearing for 4 weeks followed by weight bearing as tolerated in a locked knee brace until the 6-week mark. Motion was initiated on postoperative day 1 with the initiation of continuous passive motion machine. This was started at 30° and advanced as tolerated to a goal of 90° by 4 weeks. At 6-week postoperative, she no longer had any crepitation and was able to range her knee 0°-110° flexion/extension. At the 1-year visit, she reported doing extremely well with no crepitus on examination and range of motion back to her baseline of 0-130°. She was able to return to coaching both volleyball and softball at a local high school. Her pre- and post-operative patient-reported outcomes at 12 and 36 months demonstrated considerable improvement (Table 1).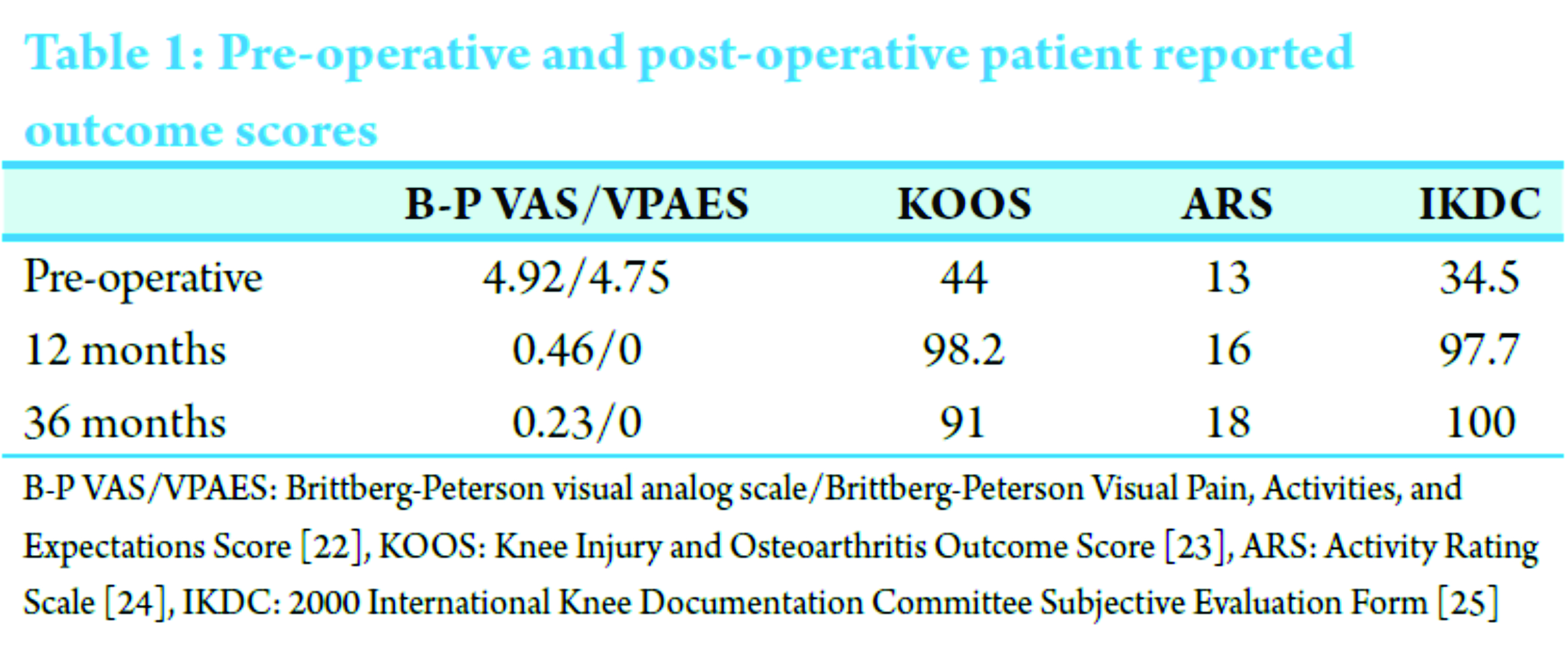
Discussion
Cartilage has limited capacity for self-repair because of its limited vascularity, which results in poor replicative capacity of chondrocytes. Because of this, full-thickness defects in articular cartilage lack the fundamental ability for complete spontaneous repair [2]. Current treatment methods for well-defined osteochondral defects include microfracture, ACI, OAT, and osteochondral allograft. However, microfracture and OAT are often ineffective or impractical for lesions >2 cm [9, 10]. Staged cell-based cartilage repair, such as ACI, remains a viable management option for large defects of the knee in young, active patients [3]. ACI is an established treatment for symptomatic focal chondral defects of the knee [3]. ACI has shown promising results in the treatment of full-thickness chondral and osteochondral defects of the knee in the short to medium term in adults and adolescents [10, 11, 12]. Recent studies have shown satisfactory outcomes in as high as 92% of patients, with long-term graft survival rates of 78% at 5 years and 51% beyond 10 years following ACI [11, 13]. The advantage of ACI is that it leads to the development of hyaline-like cartilage rather than fibrocartilage, seemingly leading to better long-term outcomes and cartilage durability [14]. Factors that favorably influence the results of ACI include a younger patient age, higher preoperative Cincinnati scores, a shorter duration of symptoms, a single osteochondral defect, and a defect located on the trochlea and/or lateral femoral condyle [11, 15]. However, lesions of the patellofemoral joint, as in our patient, have been shown to be the most difficult to treat [11, 16]. In a recent systematic review of 11 studies and 613 knees that underwent ACI for large patellar lesions, the percentage of either failed or fair/poor function ranged from 8% to 60%, demonstrating the unpredictability of ACI within the patellofemoral compartment [16]. Several studies have shown that the anatomic and biomechanical properties of the patellofemoral compartment differ significantly from those of the tibiofemoral compartment, potentially resulting in their worse outcomes [9, 17]. However, these complications were primarily related to periosteal hypertrophy, a first-generation technique that is currently less commonly performed with the increased use of collagen membranes and 3-dimensional bioscaffolds [3]. Yet, a recent study found that patients who underwent ACI of isolated patellar lesions performed as well as those with condylar lesions in the long term [18]. In addition, Mandelbaum et al., in a case series of 40 patients with symptomatic full thickness articular cartilage lesions of the trochlea, concluded with statistical significance that ACI improved function and reduced symptoms in young- to middle-aged patients [12]. Graft failures tend to occur due to grafts either partially or completely delaminating, insufficient fill, or symptomatic hypertrophy of the periosteum in first-generation ACI. Delaminations may be due to new traumatic injury or atraumatic flap formation secondary to insufficient integration to the normal surrounding peripheral cartilage or the underlying subchondral bone. The timing of hypertrophy development and its etiology are not completely understood although most authors report the presence of hypertrophy within the 1st year post-operatively [19]. Graft failures have been reported to occur around 18-24 months after ACI [20]. This confirms previous findings that subjects who have poor or even fair clinical outcomes by 2 years post-operatively eventually fail [21]. On the other hand, patients with good or excellent results tended to remain satisfied with their outcome, with 75% of subjects reporting their status as good as or better than prior years [13].
Conclusion
Although our patient is only 36 months from her multisite ACI surgery, our patient has shown that ACI implantation is not only a good option for patients with patellar or trochlear defects but also that it can be successfully used for the treatment of kissing lesions in the patellofemoral compartment.
Clinical Message
ACI remains an established treatment for isolated cartilage lesions about the knee. However, kissing lesions are much rarer, and therefore, much less is known about their treatment. This case report has demonstrated that ACI may be a suitable treatment for young active individuals with kissing cartilage lesions about the knee. Due to limitations of case reports and paucity of published literature, further investigation of treatment and outcome for kissing lesions about the knee is warranted.
References
1. Arøen A, Løken S, Heir S, Alvik E, Ekeland A, Granlund OG, et al. Articular cartilage lesions in 993 consecutive knee arthroscopies. Am J Sports Med 2004;32(1):211-215.1. Arøen A, Løken S, Heir S, Alvik E, Ekeland A, Granlund OG, et al. Articular cartilage lesions in 993 consecutive knee arthroscopies. Am J Sports Med 2004;32(1):211-215.
2. Mankin HJ. The response of articular cartilage to mechanical injury. J Bone Joint Surg Am 1982;64(3):460-466.
3. Sherman SL, Garrity J, Bauer K, Cook J, Stannard J, Bugbee W. Fresh osteochondral allograft transplantation for the knee: Current concepts. J Am Acad Orthop Surg 2014;22(2):121-133.
4. Terzidis IP, Christodoulou AG, Ploumis AL, Metsovitis SR, Koimtzis M, Givissis P. The appearance of kissing contusion in the acutely injured knee in the athletes. Br J Sports Med 2004;38(5):592-596.
5. Giuliani JR, Burns TC, Owens BD, Svoboda SJ. Knee cartilage patellofemoral injuries. Tech Orthop 2010;25(4):217-224.
6. Ossendorf C, Steinwachs MR, Kreuz PC, Osterhoff G, Lahm A, Ducommun PP, et al. Autologous chondrocyte implantation (ACI) for the treatment of large and complex cartilage lesions of the knee. Sports Med Arthrosc Rehabil Ther Technol 2011;3:11.
7. Vasiliadis HS, Lindahl A, Georgoulis AD, Peterson L. Malalignment and cartilage lesions in the patellofemoral joint treated with autologous chondrocyte implantation. Knee Surg Sports Traumatol Arthrosc 2011;19(3):452-457.
8. Gillogly SD, Myers TH, Reinold MM. Treatment of full-thickness chondral defects in the knee with autologous chondrocyte implantation. J Orthop Sports Phys Ther 2006;36(10):751-764.
9. Gudas R, Gudaite A, Pocius A, Gudiene A, Cekanauskas E, Monastyreckiene E, et al. Ten-year follow-up of a prospective, randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint of athletes. Am J Sports Med 2012;40(11):2499-2508.
10. Knutsen G, Drogset JO, Engebretsen L, Grøntvedt T, Isaksen V, Ludvigsen TC, et al. A randomized trial comparing autologous chondrocyte implantation with microfracture. Findings at five years. J Bone Joint Surg Am 2007;89(10):2105-2112.
11. Nawaz SZ, Bentley G, Briggs TW, Carrington RW, Skinner JA, Gallagher KR, et al. Autologous chondrocyte implantation in the knee: Mid-term to long-term results. J Bone Joint Surg Am 2014;96(10):824-830.
12. Mandelbaum B, Browne JE, Fu F, Micheli LJ, Moseley JB Jr, Erggelet C, et al. Treatment outcomes of autologous chondrocyte implantation for full-thickness articular cartilage defects of the trochlea. Am J Sports Med 2007;35(6):915-921.
13. Peterson L, Vasiliadis HS, Brittberg M, Lindahl A. Autologous chondrocyte implantation: A long-term follow-up. Am J Sports Med 2010;38(6):1117-1124.
14. Gikas PD, Morris T, Carrington R, Skinner J, Bentley G, Briggs T. A correlation between the timing of biopsy after autologous chondrocyte implantation and the histological appearance. J Bone Joint Surg Br 2009;91(9):1172-1177.
15. Krishnan SP, Skinner JA, Bartlett W, Carrington RW, Flanagan AM, Briggs TW, et al. Who is the ideal candidate for autologous chondrocyte implantation? J Bone Joint Surg Br 2006;88(1):61-64.
16. Noyes FR, Barber-Westin SD. Advanced patellofemoral cartilage lesions in patients younger than 50 years of age: Is there an ideal operative option? Arthroscopy 2013;29(8):1423-1436.
17. Levy YD, Gortz S, Pulido PA, McCauley JC, Bugbee WD. Do fresh osteochondral allografts successfully treat femoral condyle lesions? Clin Orthop Relat Res 2013;471(1):231-237.
18. Biant LC, Bentley G, Vijayan S, Skinner JA, Carrington RW. Long-term results of autologous chondrocyte implantation in the knee for chronic chondral and osteochondral defects. Am J Sports Med 2014;42(9):2178-2183.
19. Henderson I, Gui J, Lavigne P. Autologous chondrocyte implantation: Natural history of postimplantation periosteal hypertrophy and effects of repair-site debridement on outcome. Arthroscopy 2006;22(12):1318-1324.e1.
20. Harris JD, Siston RA, Brophy RH, Lattermann C, Carey JL, Flanigan DC. Failures, re-operations, and complications after autologous chondrocyte implantation – A systematic review. Osteoarthritis Cartilage 2011;19(7):779-791.
21. Peterson L, Brittberg M, Kiviranta I, Akerlund EL, Lindahl A. Autologous chondrocyte transplantation. Biomechanics and long-term durability. Am J Sports Med 2002;30(1):2-12.
22. Peterson L, Minas T, Brittberg M, Nilsson A, Sjögren-Jansson E, Lindahl A. Two- to 9-year outcome after autologous chondrocyte transplantation of the knee. Clin Orthop Relat Res 2000;374:212-234.
23. Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS) – Development of a self-administered outcome measure. J Orthop Sports Phys Ther 1998;28(2):88-96.
24. Marx RG, Stump TJ, Jones EC, Wickiewicz TL, Warren RF. Development and evaluation of an activity rating scale for disorders of the knee. Am J Sports Med 2001;29(2):213-218.
25. Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 2001;29(5):600-613.
 |
 |
 |
| Dr. Taylor J Ridley | Christopher T Rud | Dr. Jeffrey A Macalena |
| How to Cite This Article: Ridley TJ, Rud CT, Macalena JA. Patellofemoral Articulating Osteochondral (Kissing) Lesion Treated with Autologous Chondrocyte Implantation: A Case Report. Journal of Orthopaedic Case Reports 2017 May-June;7(3):41-44. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


