
[box type=”bio”] What to Learn from this Article?[/box]
In neglected elbow dislocations, open reduction and cruciate ligament reconstruction help us in early mobilization and for better stability of elbow joint.
Case Report | Volume 7 | Issue 4 | JOCR July – August 2017 | Page 58-60| Ganesh N Pundkar, Satish B Sonar, Omkar P Kulkarni. DOI: 10.13107/jocr.2250-0685.852
Authors: Ganesh N Pundkar[1], Satish B Sonar[1], Omkar P Kulkarni[1]
[1]Department of Orthopaedics, Panjabrao Deshmukh Memorial, Medical College, Amravati. Maharashtra. India.
Address of Correspondence
Dr. Omkar P Kulkarni,
110 PG Hostel, Panjabrao Deshmukh Medical College, Panchwati, Amravati – 444 603, Maharashtra. India.
E-mail: dr.omkarkulkarni@gmail.com
Abstract
Introduction: Old neglected posterior type of elbow dislocations is not very common and generally requires open reduction. It was usually treated with open reduction and K-wire stabilization. We did a newer method in which in addition cruciate type ligament reconstruction; we have reconstructed lateral ulnar collateral ligament (LUCL) and UCL (medial collateral ligament) using semitendinosus graft. This allowed extra stability and early mobilization of the elbow joint. Authors report 3-month-old neglected posterior type of elbow dislocation without any fracture.
Case Report: A 42-year-old male presented with pain and tenderness with deformity of the left elbow joint and inability to move the elbow joint after he fell down since 3 months. There was no neurovascular deficit. Radiological examination confirmed posterior dislocation of elbow joint without any fracture. The patient is managed by open reduction and cruciate ligament reconstruction of elbow joint using autologous semitendinosus graft.
Conclusion: Open reduction with cruciate ligament reconstruction provides excellent stability for early mobilization of old neglected elbow dislocation.
Keywords: Elbow joint, posterior dislocation, cruciate ligament.
Introduction
Posterior type of dislocation of the elbow joint is common than anterior type. Anterior and posterior type of dislocation of elbow joint are decided in relation of radius and ulna with humerus, if radius and ulna dislocate posterior to humerus, it is known as posterior type and if anterior to humerus known as anterior type dislocation elbow joint [1]. Neglected elbow dislocations are common in developing countries like our India. The main reason for delayed diagnosis is due to inaccessibility to health care and consequent inadequate treatment initially. This leads to retraction of triceps muscles and collateral ligaments. The resulting nonfunctional unreduced elbow joint makes the surgical procedure quite challenging [2, 3]. In these cases require surgical treatment, the surgeon has many options to consider the surgical approach, need for triceps lengthening, and stabilization of elbow after reduction and repair of collateral ligaments.
We have reported a case of the neglected 3-month-old posterior type of dislocation of elbow joint without any neurological deficit in 42-year-old male patient.
Case Report
A 42-year-old male patient came in hospital with chief complaints of pain and swelling of the left elbow joint with deformity and inability to move the left elbow joint. There was no neurovascular deficit. He had a history of fall 3 months back followed by application of massage and manipulation by local bone setter. The patient did not take medical treatment for same at that time. Radiological examination (Fig. 1) confirmed posterior type of dislocation of elbow joint without any fracture.
Management
We planned for open reduction, and the extra stability peroperatively can be provided using two cruciate-like ligaments for the ulnohumeral and radiocapitellar joints so that postoperatively early movement is permitted safely. A patient was counseled about the treatment options, their expected results, advantages, disadvantages, and complications. A special consent was taken from the patient for harvesting semitendinosus graft.
Surgical technique
Surgical procedure started with single midline posterior skin incision followed by a medial plus lateral approach in the deeper planes (Fig. 2).
Identification and preservation of ulnar nerve were first and important step (Fig. 3) followed by extensive release of fibrosis around the joint (Fig. 4). A special care was taken to preserve lateral and medial collateral ligament, or whatever was present left of them. We kept our dissection close to the bone and away from collaterals to avoid any damage. Radiohumeral horn was carefully identified and excised. This step facilitates radiocapitellar reduction. Precaution was taken to preserve articular cartilage, and nibbling of soft tissue around the articular cartilage was avoided. We performed V-Y plasty of triceps.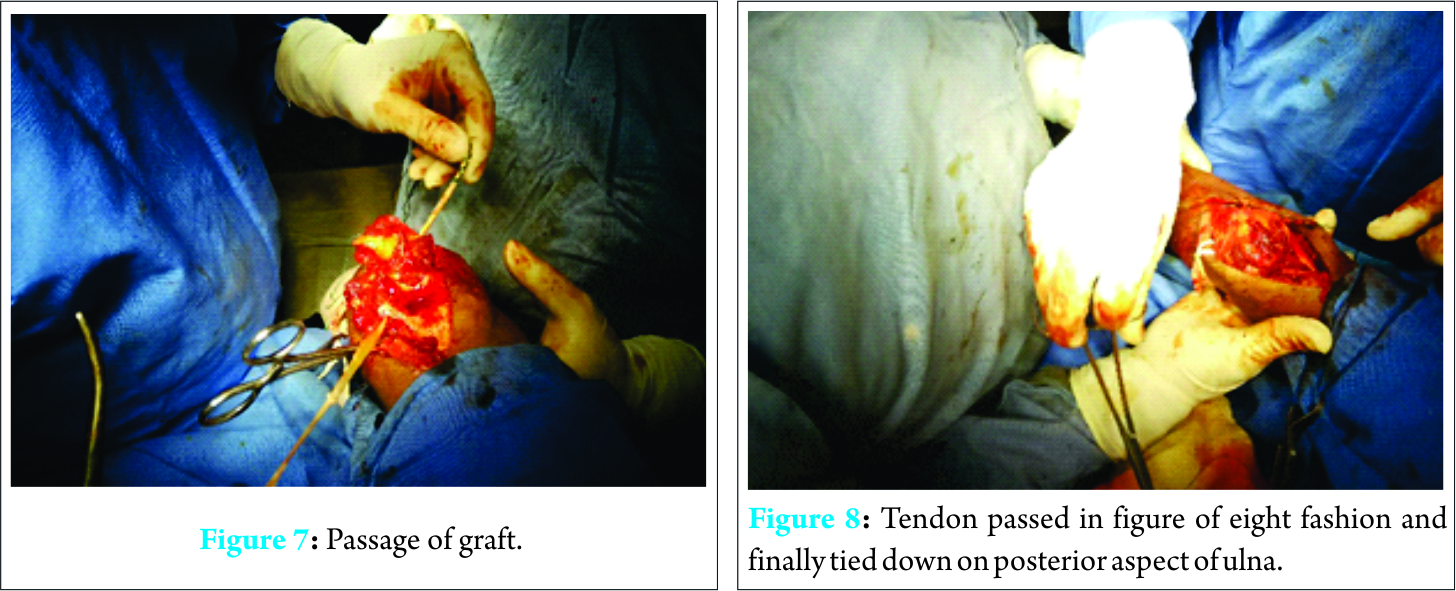
A technique originally published by Arafiles et al. [3] involved construction of an anterior-posterior cruciate ligament like structure using the palmaris longus tendon, but we harvested semitendinosus (Fig. 5) for our surgery .Total four holes are made using drill, two each in the humerus and ulna to pass the tendon through them in a figure of eight fashion (Fig. 6). The tendon passes through the articular surface of the olecranon and enters the articular surface of trochlea, winds back on the lateral condyle and passes the ulna to be finally tied down on the posterior aspect of ulna (Figs. 7 and 8).We released more contracted tissue until we were achieved full range of motion. We checked for both anteroposterior and mediolateral stability during various degrees of flexion and supination pronation and adjusted our slings likewise. At the end of procedure, we succeeded in achieving good stability which was confirmed by testing ROM in all planes. Wound closed in layers and drain kept in situ (Fig. 9). Above elbow slab given postoperatively and later drain was removed after 24 h (Fig. 10 post-operative X-ray). We allowed movement on the very next day of operation. Post-operative analgesic care was taken to allow pain-free movements. Active movements and gradual strengthening exercises started over a period of 3 weeks. Light weight lifting was given after 4 weeks and full weight lifting after 3 months. Follow-up was done at 3, 6, and 12 weeks and then after 3 months. In our case, we assessed for any pain, range of movements, and stability. Radiographic evaluation was also done.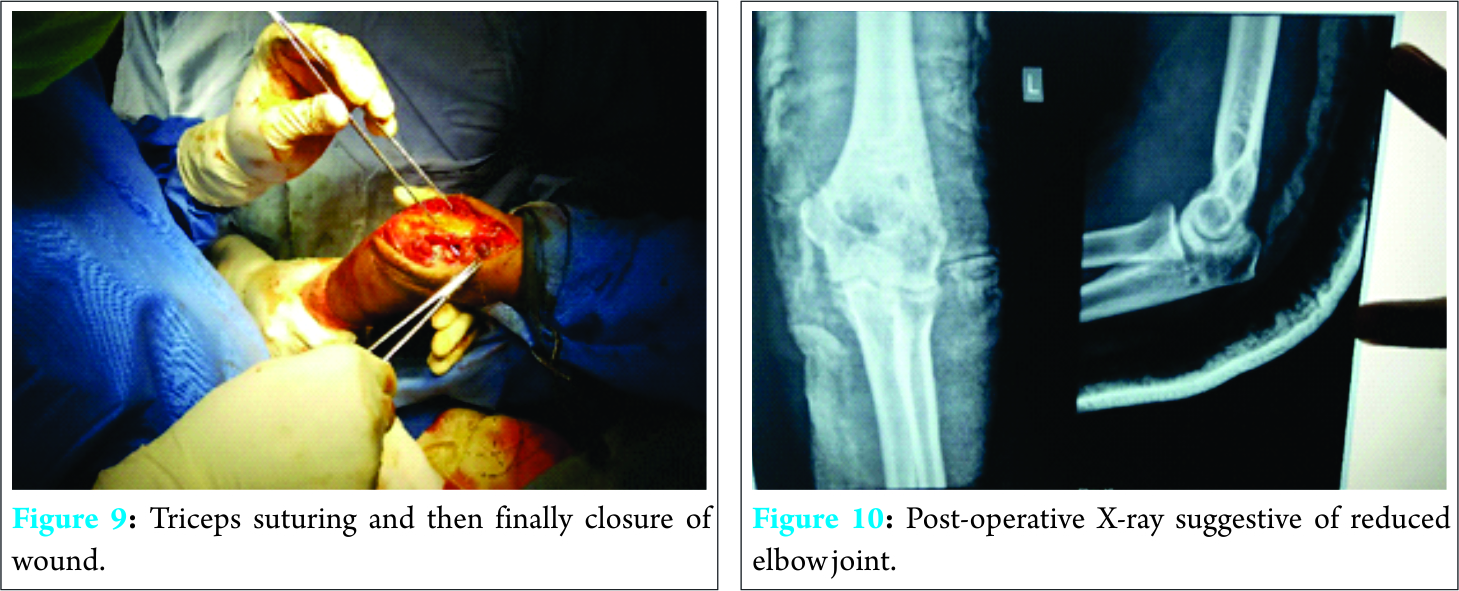
Results
We got satisfactory results in our case in terms of pain-free full range of motion along with the good stability of elbow joint. The patient is doing all his active routine physical activities without any limitations.
Discussion
In remote areas due to poor access to proper medical facilities and due to lack of awareness old unreduced elbow dislocations are common. Such patients are often neglected and maltreated before being seen by a specialist. Most surgeons recommend closed reduction for elbow dislocation up to 3 weeks post injury. After 3 weeks development of soft tissue contracture and osteoporosis makes closed reduction dangerous as manipulation may lead to fracture of the bone or damage the articular surface [4, 5, 6] most of surgeons advise open reduction for elbow dislocation up to 3 months; total elbow arthroplasty; excisional arthroplasty, or arthrodesis is advised thereafter. Speed (1925) introduced the method of triceps lengthening using V-Y plasty to reduce old dislocations of elbow [7]. The same method has been followed by many authors all throughout the century such as Billet [8], Naidoo [6], and Fowles et al. [9]. The technique essentially consists of extensive release, V-Y plasty and K-wire fixation for 2-4 weeks post-operative followed by aggressive physiotherapy. However, all of them use K-wire or plaster of Paris cast immobilization postoperatively for a varied amount of time. The only exception being Arafiles et al. [3], who have tried to create an intra-articular cruciate ligament-like structure using palmaris longus of the patient to provide immediate anteroposterior stability to the patient. This could avoid a K-wire fixation and give early movement to the patients. We have used semitendinosus tendon instead of palmaris longus for our patient. Proper dissection techniques avoided injury to collaterals ligaments and articular cartilage. Important purpose of cruciate ligament reconstruction is early mobilization. We started mobilization on next day only with our physiotherapy department. Good post-operative analgesia and proper motivational support helped to start active movements early. We got satisfactory results.
Conclusion
Open reduction with cruciate ligament reconstruction helps in the early mobilization of old neglected elbow dislocations and also gets satisfactory results.
Clinical Message
Posterior elbow dislocation can be treated by simple closed reduction. But in a neglected cases it become an issue not only of reducing it but also maintaining that reduction and stability. Only open reduction and temporary stabilization can cause post-operative instability or stiffness as it needed to be protected for a longer period. But in open reduction and cruciate ligament reconstruction along with our technique of adding lateral ulnar collateral ligament and medial collateral ligament components to the reconstruction, helps us to mobilize the elbow joint immediately and achieve good to excellent stability and functions. It is one of the better methods to treat neglected elbow dislocation in anatomical way.
References
1. Wilkins KE. Fracture and dislocations of elbow region. In: Rockwood CA, Wilkins KE, King RE, editors. Fractures in Children. 4th ed., Vol. 3. Philadelphia, PA: Lippincott-Raven; 1996. p. 653-887.1. Wilkins KE. Fracture and dislocations of elbow region. In: Rockwood CA, Wilkins KE, King RE, editors. Fractures in Children. 4th ed., Vol. 3. Philadelphia, PA: Lippincott-Raven; 1996. p. 653-887.
2. Martini M, Benselma R, Daoud A. Les luxations négligées du coude 25 repositions sanglantes. Rev Chir Orthop 1984;70:305-312.
3. Arafiles RP. Neglected posterior dislocation of the elbow. A reconstruction operation. J Bone Joint Surg Br 1987;69(2):199-202.
4. Freeman BL 3rd. Old unreduced dislocations. In: Crenshaw AH, editor. Campbell’s Operative Orthopedics. 9th ed., Vol. 1. St Louis: Mosby; 1998. p. 2673-4.
5. Rockwood CA, editor. Treatment of old unreduced posterior dislocation of elbow. In: Rockwood and Green’s Fracture in Adults. 4th ed., Vol. 1. Philadelphia, PA: Lippincot-Raven; 1996. p. 975-6.
6. Naidoo KS. Unreduced posterior dislocations of the elbow. J Bone Joint Surg Br 1982;64(5):603-606.
7. Speed JS. An operation for unreduced post dislocation of elbow. S Med J 1925;18:193.
8. Billett DM. Unreduced posterior dislocation of the elbow. J Trauma 1979;19(3):186-188.
9. Fowles JV, Kassab MT, Douik M. Untreated posterior dislocation of the elbow in children. J Bone Joint Surg Am 1984;66(6):921-926.
 |
 |
 |
| Dr. Ganesh N Pundkar | Dr. Satish B Sonar | Dr. Omkar P Kulkarni |
| How to Cite This Article: Pundkar GN, Sonar SB, Kulkarni OP. A Case of 3-month-old Neglected Elbow Dislocation Managed by Open Reduction and Cruciate Ligament Reconstruction Using Tendon Graft. Journal of Orthopaedic Case Reports. 2017 Jul-Aug;7(4):58-60. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


