
[box type=”bio”] Learning Points for this Article: [/box]
Though unlikely, Chance fracture at thoracic level are a possibility. Plain X-rays need to be examined very thoroughly so that a chance fracture is not missed. Visceral injuries have to be ruled out carefully.
Case Report | Volume 7 | Issue 4 | JOCR July – August 2017 | Page 62-65 | Aditya Menon, Camilla Rodrigues, Rajeev Soman, Ayesha Sunavala, Vikas M Agashe. DOI: 10.13107/jocr.2250-0685.854
Authors: Aditya Menon[1], Camilla Rodrigues[2], Rajeev Soman[3], Ayesha Sunavala[3], Vikas M Agashe[1]
[1] Department of Orthopaedics, Sancheti Institute of Orthopaedics and Rehabilitation, Pune, Maharashtra, India.
Address of Correspondence
Dr. Himanshu Gurunath Kulkarni,
Department of Orthopaedics, Sancheti Institute of Orthopaedics and Rehabilitation, Pune, Maharashtra, India.
E-mail: hgkulkarni@gmail.com
Abstract
Introduction: Chance fractures, the horizontal splitting vertebral fractures caused by flexion distraction mechanism, are inherently unstable fractures. These fractures can land up with significant visceral injuries. There are most commonly seen at thoracolumbar junction or in lumbar spine due to their high mobility. These fractures are extremely rare in the thoracic spine due to the rigidity of thoracic spine rendered by attachment of ribs. Furthermore, the level of injury makes neurological complications even graver.
Case Report: We present a case of a road traffic accident with right lower limb monoplegia. On careful examination, a thin transverse fracture line was noticed in D5 vertebral body, and magnetic resonance imaging revealed posterior ligamentous disruption extending in line with the transverse fracture line in D5 vertebral body which confirmed the diagnosis of a Chance fracture. Fracture was stabilized by pedicle screw fixation from D4 to D7 level, and decompression was done at D5 level. By the end of 7 months, patient regained Grade 4 power in the right hip and knee joints, with Grade 5 power in the right ankle and great toe.
Conclusion: Chance fractures in thoracic region are extremely rare. A clinician should have a high index of suspicion as these fractures can be notorious when it comes to presentation on plain X-ray. These being inherently unstable fractures, posterior instrumented stabilization with decompression in patients with neurodeficit gives good results.
Keywords: Chance fracture, flexion distraction injury, seat belt injury, monoplegia.
Introduction
Chance fractures are the fractures caused by the horizontal splitting of the vertebra. The mechanism of the injury is the flexion and distraction forces applied on the spine, usually over a fulcrum site. The fulcrum usually is a seat belt worn by drivers involved in car accidents or a safety harness belt used by workers who accidentally fall from height [1]. These mechanisms cause the anterior column to fail under tension along with middle and posterior columns and cause a flexion-distraction injury. Usually, these fractures occur at thoracolumbar junction or lumbar spine, due to the high mobility of these areas. Due to the rigidity of thoracic spine provided by the ribs, these injuries are extremely rare in thoracic spine [2]. Furthermore, this being an unstable fracture, the neurological deficit is present in most of the cases. Only a handful of cases of Chance fractures in the thoracic spine have been reported in the literature. We present a case of extremely rare case of upper thoracic chance fracture (D5) with monoplegia of the left lower limb.
Case Report
A 26-year-old male came to the casualty with a history of a road traffic accident of two four-wheelers, with the patient sitting on back seat. He was conscious, oriented, and had no history and symptoms suggestive of a head injury. The patient complained of severe mid back pain with inability to move his right lower limb. On examination, there was tenderness over upper and mid-thoracic spine, and he had Grade 0 power in all this right lower limb joints. Power in all left lower limb joints was Grade 5. His bladder and bowel sensations were intact, and anal tone was normal. The patient had loss of sensations of the right side of the trunk below nipple with lost sensation in the right lower limb till S2 dermatome. Reflexes were absent on affected right side with hyperreflexia on the left side. The patient also had bilateral up-going plantar reflexes (Babinski’s sign) indicating an upper motor neuron-type lesion. On first glance, X-ray of thoracic spine revealed nothing except the fracture of spinous processes of D4 and D5 vertebrae. On careful examination, a thin transverse fracture line was noticed in D5 vertebral body (Fig. 1).
Magnetic resonance imaging (MRI) revealed posterior ligamentous disruption extending in line with the transverse fracture line in D5 vertebral body, cord contusion with minimal edema at D5-6 level (Fig. 2). Computed tomography showed fractures of transverse processes of D4 and D5, with no retropulsion of fragment at D5 level (Figs. 3 and 4). The diagnosis of D5 Chance fracture was confirmed. Fracture was classified to be AO type B2-N3 (distraction injury with osseoligamentous disruption and incomplete cord injury). On calculation, thoracolumbar injury classification and severity (TLICS) score was found to be 10 (distraction injury-4, posterior ligamentous complex [PLC] injured-3 incomplete spinal cord injury-3). Keeping the unstable nature of fracture, neurodeficit, and TLICS score >4 in mind, decision was taken to carry out operative procedure. Midline incision was taken, and dissection was done. Thorough decompression was done in D5 level. Undercutting of D4 and D6 was done. Pedicle screw fixation was done from D4 to D7 level (Fig. 5). Screws were passed in fractured D5 for better stability. Closure was done over drain. Post-operative physiotherapy was started from 2nd post-operative day. On 16th post-operative day, the patient regained Grade 1 power in hip flexors. By the end of 7 months, the patient regained Grade 4 power in all movements of the right hip and knee joints, with Grade 5 power in the right ankle and great toe.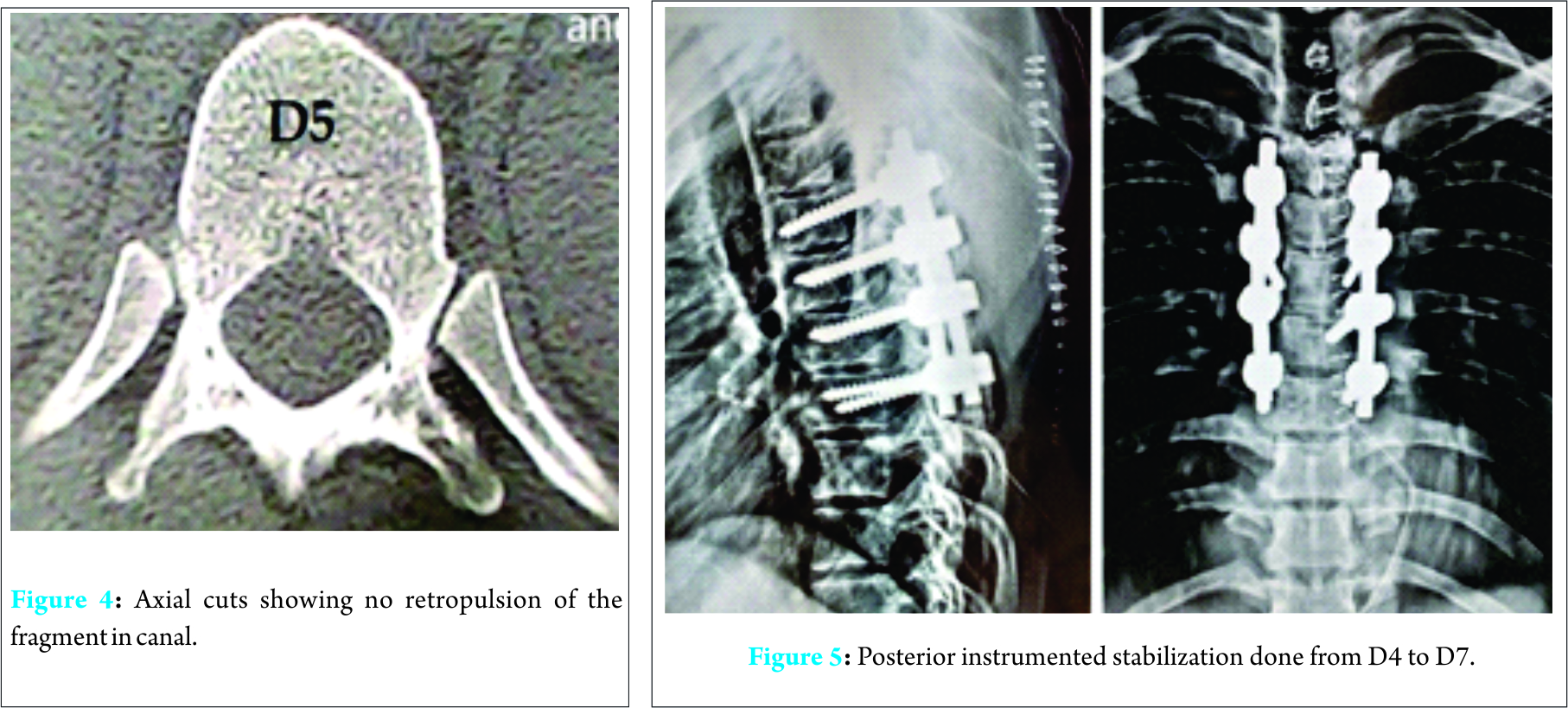
Discussion
In 1948, Chance fracture was first described by Chance, a British radiologist [3]. The term Chance’s fracture was coined by Nicoll [4]. The agreed mechanism of injury is one of flexion distraction against an anterior fulcrum, most commonly a seat belt. The accepted mechanism of injury is of flexion-distraction with all 3 columns failing in tension after sudden deceleration. The point of motion in the body impacting against this fulcrum is normally the spine itself. When hyperflexion of the spine occurs over a fulcrum, the force is displaced anteriorly and lies at the point of contact between the fulcrum and the abdominal wall. This subjects all of the components of the spine to tension stress. The result is a disruption of the ligaments and posterior elements of the spine and a transverse fracture of the posterior elements and body of the spine. Hence, in this fracture, simultaneous posterior ligament injury should be taken into consideration, since it renders the fracture its inherent instability and necessitates the fixation [5]. Anatomy plays a major role in presentations of Chance fractures. In the thoracic spine, there is a great restraint to motion due to attachments of the ribs. This makes Chance fracture a very unlikely variant in the thoracic spine. Furthermore, in most of the cases, it is the seat belt which acts as a fulcrum, so the injury is below that region, which is below the thoracic region. In children, the head-body weight ratio is higher because of children’s higher center of gravity and subsequent greater lever arm. Hence, it produces greater tensile forces surrounding the axis of rotation and makes the chance fractures more common in children than in adults [6]. In the thoracolumbar region, more mobility leads to more common incidence of chance fracture. Hence, the region of L1 to L3 has been labeled to most prone area for the occurrence of typical chance fractures [7]. Chance fractures are also associated with their share of associated comorbidities. Various studies have stated that there is a very high chance of copresence of abdominal injuries with Chance fractures. Some studies have reported associated abdominal injuries in as high as up to 67% cases [8, 9, 10]. Abdominal wall contusions, bowel perforations, and liver lacerations are a few among the reported serious comorbidities. Complete paraplegia has also been a reported complication, but the patient, in our case, was fortunate enough to have only monoplegia of the right lower limb with intact bowel and bladder sensations. In children, due to underdevelopment of the rib cage and pelvis, associated injuries in this seat belt fracture tend to be more severe [6]. Coexisting injuries in thoracic Chance fractures can be different than the usual thoracolumbar fractures, due to thoracic anatomy and the close proximity of vital vascular structures.
Conclusion
Hence, chance fractures in thoracic region are extremely rare. Furthermore, monoplegia is very unusual presentation in these fractures which are known to cause paraplegia. A clinician should have a high index of suspicion as these fractures can be notorious when it comes to presentation on plain skiagrams. MRI should be done to evaluate the injury to PLC and neural compromise. Careful screening of associated comorbidities is also necessary. These being inherently unstable fractures, posterior instrumented stabilization with decompression in patients with neurodeficit gives good results.
Clinical Message
Diagnosing Chance fractures can be challenging. A high index of suspicion is necessary for diagnosis when the patient comes with a peculiar mechanism of injury. Injuries to other organs should be carefully ruled out.
References
1. Todkar M. Case report: Unusual mechanism of chance fracture in an adult male. MedGenMed 2005;7(2):26.1. Todkar M. Case report: Unusual mechanism of chance fracture in an adult male. MedGenMed 2005;7(2):26.
2. Unal M, Turan AC, Akçali O. Isolated upper thoracic chance fracture with neurological deficit, without bone injury, Case Report. Austin J Orthop Rheumatol 2014;1(2):2.
3. Chance GQ. Note on a type of flexion fracture of the spine. Br J Radiol 1948;21(249):452.
4. Nicoll EA. Fractures of the dorso-lumbar spine. J Bone Joint Surg Br 1949;31B(3):376-394.
5. Davis JM, Beall DP, Lastine C, Sweet C, Wolff J, Wu D. Chance fracture of the upper thoracic spine. AJR Am J Roentgenol 2004;183(5):1475-1478.
6. Agran PF, Dunkle DE, Winn DG. Injuries to a sample of seatbelted children evaluated and treated in a hospital emergency room. J Trauma 1987;27(1):58-64.
7. Smith WS, Kaufer H. Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51(2):239-254.
8. Reid AB, Letts RM, Black GB. Pediatric chance fractures: Association with intra-abdominal injuries and seatbelt use. J Trauma 1990;30(4):384-391.
9. Gallagher DJ, Heinrich SD. Pediatric chance fracture. J Orthop Trauma 1990;4(2):183-187.
10. Voss L, Cole PA, D’Amato C. Pediatric chance fractures from lapbelts: Unique case report of three in one accident. J Orthop Trauma 1996;10(6):421-428.
 |
 |
 |
 |
 |
 |
| Dr. Ketan Shripad Khurjeka | Dr. Himanshu Kulkarni | Dr. Shailesh Hadgaonkar | Dr. Ajay Kothari | Dr. Ashok Shyam | Dr. Parag Sancheti |
| How to Cite This Article: Khurjeka KS, Kulkarni HG, Hadgaonkar S, Kothari A, Shyam A, Sancheti P. A Case Report: Upper Thoracic Chance Fracture with Monoplegia… An Unusual Presentation! Journal of Orthopaedic Case Reports 2017 Jul-Aug;7(4):65-67. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


