
[box type=”bio”] What to Learn from this Article?[/box]
Acetabular fractures after hemiarthroplasty can be treated by conversion to a total hip arthroplasty after stabilization of the fracture by means of cerclage wires.
Case Report | Volume 7 | Issue 6 | JOCR Nov – Dec 2017 | Page 20-23| Vanlommel Jan, Vanderschot Paul. DOI: 10.13107/jocr.2250-0685.932
Authors: Vanlommel Jan [1], Vanderschot Paul [2]
[1]Orthoclinic, AZ Sint-Lucas, Brugge, Belgium.
[2]Department of Traumatology, University Hospital Leuven, Belgium.
Address of Correspondence:
Prof. Paul Vanderschot, University Hospital Leuven, Herestraat 49, Leuven, Belgium.
E-mail: paul.vanderschot@uzleuven.be
Abstract
Introduction: Hip fractures in the elderly pose an increasing problem in society. In the elderly, a bipolar hemiarthroplasty (HA) remains the treatment of choice in case of hip fractures related to osteoporosis. However, due to an ongoing osteoporosis in this age group, a periprosthetic femoral fracture and a fracture of the unresurfaced acetabulum are increasingly noticed. In the literature, no information can be found regarding the treatment options for this kind of periprosthetic acetabular fracture.
Case presentation: We present a case report of a patient suffering an acetabular fracture 6 years after a hemi-arthroplasty. A one stage surgical procedure was the treatment of choice, consisting of a stabilization the acetabulum fracture by means of cerclage wires and a conversion of the hemi-arthroplasty to a total hip arthroplasty. Four months after surgery, she regained her pre-operative functional status and a radiographic evaluation of the right hemipelvis showed good signs of the fracture healing without migration of the acetabular component.
Conclusion: This case shows a ‘one stage’ surgery solution for an acetabular fracture after hemiarthroplasty. Stabilization of the acetabulum fracture by means of cerclage wires and a conversion of the hemi-arthroplasty to a total hip arthroplasty is a viable solution for this rare and challenging problem.
Keywords: hemiarthroplasty, acetabular fracture, cerclage wires
Introduction
Hip fractures in the elderly pose an increasing problem in society. This increase can be attributed to a greater longevity of the population, associated with a high prevalence of osteoporosis and concomitant morbidities. In the elderly, a bipolar hemiarthroplasty (HA) remains the treatment of choice in case of hip fractures related to osteoporosis [1]. However, due to an ongoing osteoporosis in this age group, a periprosthetic femoral fracture [2] and a fracture of the unresurfaced acetabulum [3] are increasingly noticed. This latter complication is a rather rare but a devastating complication after a hip hemiarthroplasty. In the literature, no information can be found regarding the treatment options for this kind of periprosthetic acetabular fracture. We present a case report of a patient suffering an acetabular fracture 6 years after a hemi-arthroplasty. A one stage surgical procedure was the treatment of choice, consisting of a stabilization the acetabulum fracture by means of cerclage wires and a conversion of the hemi-arthroplasty to a total hip arthroplasty.
Case Presentation
A 90-years-old female was transferred to the hospital after sustaining a low-energy trauma, a simple fall. She experienced pain at the right hip and pelvis. Weight bearing on the affected side was no longer possible. The medical file revealed a hemiarthroplasty for a displaced femoral neck fracture at the right and left side, respectively 6 and 8 years ago. She was ambulating only short distances using a walking stick. Radiographic assessment revealed a displaced acetabular fracture with a central dislocation of the bipolar head. Impaction against the acetabular roof resulted in a displaced fracture of the greater trochanter (Fig.1a and 1b).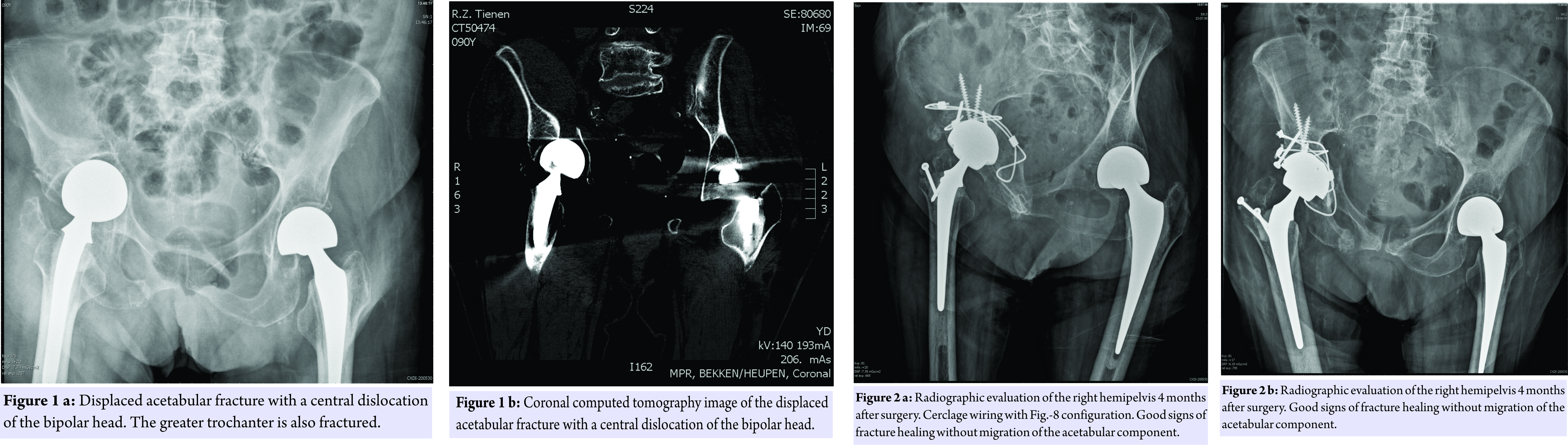
No other bony lesions or associated neurovascular injuries where noted. After a careful preoperative assessment, the surgical plan consisted of a stabilization of the acetabulum fracture by means of cerclage wires together with a conversion of the hemiarthroplasty to a total hip prosthesis. The patient was positioned in a lateral decubitus. A tri-radiate approach was preferred to gain a wide exposure to the hip joint. The greater trochanter was already fractured. So, no osteotomy at that level needed to be done. After removal of the bipolar head, the femoral component seemed to be fixed very well and was left in place. First of all, a 2mm braided cable (Zimmer, Inc., Warsaw, Indiana) passed around the body of the ischial bone using Statinsky aortic clamps. Thereafter, one end of the wire carefully passed along the inner pelvic surface while the other passed under beneath the sacrospinal ligament. Both ends were clamped together above the acetabulum, creating a figure-8 configuration (Fig. 2a) as described by Mears et al [4]. A second cerclage wire was used to fix the posterior column (Fig. 2a). After reduction and stabilization of the acetabular fracture, the acetabulum was progressively reamed to the appropriate size. A cementless Trabecular Metal cup (Zimmer, Inc., Warsaw, Indiana) was inserted and titanium screws were applied to provide additional stability to the construct. A highly crosslinked polyethylene liner was implanted together with a new metallic femoral head. The fracture of the greater trochanter was reduced and fixed by means of two AO screws. Finally, a reduction of the total hip prosthesis was performed which seemed to be stable without major leg length discrepancy. Postoperatively, continuous passive motion of the operated hip was started immediately. Weight bearing was not allowed during the first 6 weeks. Thereafter, ambulating using a walking device and partial weight bearing (20kg) was allowed. Four months after surgery, she regained her pre-operative functional status and a radiographic evaluation of the right hemipelvis showed good signs of the fracture healing without migration of the acetabular component (Fig. 2a and 2b).
Discussion
When dealing with an aging population, the prevalence and burden of all osteopenic fractures continue to be of great concern. The incidence of femoral fractures seems to stabilize and even to decrease. On the other hand, the incidence of acetabular fractures shows a 2.4-fold increase over the past quarter of a century. This increasing incidence can be attributed to geriatric patients with osteoporotic bone which are the fastest growing subgroup of patients with acetabular fractures [3,5,6]. Arthroplasty is a well-accepted treatment for patients with displaced femoral neck fractures, showing a decreased patient risk of operation compared with internal fixation at mid- and long-term follow-ups [7]. Regarding the type of implant, current evidence supports a thermoplastic as the treatment of choice for the low-demand elderly patient [8,9]. Since these patients are at high risk of subsequent fractures, it is not unlikely they sustain an ipsilateral acetabular fragility fracture, resulting from a low-energy trauma such as a fall from a standing height [3,10]. Few reports have been published discussing the treatment of traumatic periprosthetic acetabular fractures after total hip arthroplasty. Several treatment options were described, including conservative treatment and acute or delayed revision arthroplasty [11,12]. To our knowledge, no literature exists regarding the treatment of an acute acetabular fracture after hemiarthroplasty of the ipsilateral hip. In this case report, we preferred an acute one stage procedure: conversion to a THA with open reduction and stabilization of the acetabular fracture with two cerclage wires. Several techniques of fracture reduction and stabilization (cables, formal ORIF, or percutaneous ORIF) can be used but the goal of the treatment remains the reduction both columns in such a way that a fracture stability can be achieved for the acetabular component, which is imperative to minimize the risk of aseptic cup loosening [13]. In our case the cerclage technique as described by Mears et al. was used [4]. Good functional and radiographical results have been reported with this technique when treating acetabular fractures with acute total hip arthroplasty [4,14]. The advantage of a one stage surgical procedure is obvious: reduction of the postoperative time of bed rest and full weight bearing which can be allowed rapidly. In this way, associated complications such as decubitus and venous thrombosis can be reduced.
Conclusion
This case shows a ‘one stage’ surgery solution for an acetabular fracture after hemiarthroplasty. Our short term follow-up showed an adequate fixation of the acetabular component, an adequate healing of the acetabular fracture which allows a rapid mobilization of the patient. Therefore we believe this is a viable solution for this rare and challenging problem. A longer follow-up and more cases are necessary to confirm these findings.
Clinical Message
A periprosthetic fracture of the unresurfaced acetabulum after a hemiarthroplasty is a rare but severe complication. Acute stabilization of the acetabulum fracture by means of cerclage wires and a conversion of the hemi-arthroplasty to a total hip arthroplasty is a viable solution for this challenging problem.
References
1. Roberts KC, Brox WT, Jevsevar DS, Sevarino K. Management of hip fractures in the elderly. J Am Acad Orthop Surg 2015;23(2):131-7.
2. Yoon BH, Lee YK, Jo WL, Ha YC, Choi DH, Koo KH. Incidence and Risk Period of Periprosthetic Femoral Fracture After Cementless Bipolar Hemiarthroplasty in Elderly Patients. J Arthroplasty in press 2015
3. Ferguson TA, Patel R, Bhandari M, Matta JM. Fractures of the acetabulum in patients aged 60 years and older: an epidemiological and radiological study. J Bone Joint Surg Br 2010;92:250-7.
4. Mears DC, Shirahama M. Stabilization of an acetabular fracture with cables for acute total hip arthroplasty. J Arthroplasty 1998;13:104-7.
5. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA 2009;302:1573-9.
6. Butterwick D, Papp S, Gofton W, Liew A, Beaulé PE. Acetabular fractures in the elderly: evaluation and management. J Bone Joint Surg Am 2015;97:758-68.
7. Jiang J, Yang CH, Lin Q, Yun XD, Xia YY. Does Arthroplasty Provide Better Outcomes Than Internal Fixation At Mid- and Long-term Followup? A Meta-analysis. Clin Orthop Relat Res 2015;473:2672-9.
8. Grosso MG, Danoff JR, Padgett DE, Iorio R, Macaulay WB. The Cemented Unipolar Prosthesis for the Management of Displaced Femoral Neck Fractures in the Dependent Osteopenic Elderly. J Arthroplasty 2016;31:1040-6.
9. Jonas SC, Shah R, Al-Hadithy N, Norton MR, Sexton SA, Middleton RG. Displaced intracapsular neck of femur fractures in the elderly: bipolar hemiarthroplasty may be the treatment of choice; a case control study. Injury 2015;46:1988-91.
10. Johnell O, Kanis JA, Odén A, Sernbo I, Redlund-Johnell I, Petterson C, De Laet C, Jönsson B. Fracture risk following an osteoporotic fracture. Osteoporos Int 2004;153:175-9.
11. Peterson CA, Lewallen DG. Periprosthetic fracture of the acetabulum after total hip arthroplasty. J Bone Joint Surg Am 1996;788:1206-13.
11. Sánchez-Sotelo J, McGrory BJ, Berry DJ. Acute periprosthetic fracture of the acetabulum associated with osteolytic pelvic lesions: a report of 3 cases. J Arthroplasty 2000;15:126-30.
13. Mears DC, Velyvis JH. Primary total hip arthroplasty after acetabular fracture. Instr Course Lect 2001;50:335-54.
14. Mouhsine E, Garofalo R, Borens O, Blanc CH, Wettstein M, Leyvraz PF. Cable fixation and early total hip arthroplasty in the treatment of acetabular fractures in elderly patients. J Arthroplasty 2004;19:344-8.
 |
 |
| Dr. Vanlommel Jan | Dr. Vanderschot Paul |
| How to Cite This Article: Vanlommel J, Vanderschot P. Acetabular Fracture after Hip Hemiarthroplasty: One Stage Procedure to a Total Hip Arthroplasty after Stabilization of the Fracture by Means of Cerclage Wires. Journal of Orthopaedic Case Reports 2017 Nov-Dec; 7(6): 20-23. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


