
[box type=”bio”] Learning Point for this Article: [/box]
Impaled object should always be removed under direct vision in operation theatre.
Case Report | Volume 8 | Issue 1 | JOCR Jan – Feb 2018 | Page 71-74| Santosh Nagnath Banshelkikar,Binoti A Sheth, Rakesh P Dhake, Arvind B Goregaonkar DOI: 10.13107/jocr.2250-0685.1006
Authors: Santosh Nagnath Banshelkikar[1],Binoti A Sheth[1], Rakesh P Dhake[1], Arvind B Goregaonkar[1]
[1]Department of Orthopedics, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Santosh Nagnath Banshelkikar,
Flat B/502, building no 91 Deepmandir CHS, Tilak Nagar (West), Mumbai – 400 089, Maharashtra, India.
E-mail: drsantoshnb@gmail.com
Abstract
Introduction: Impalement injuries are one of the rare presentations in the emergency department and present complex surgical challengesin management.Prompt transfer to tertiary centre, pre-operative planning, and multi specialty involvement is crucial in the management of such cases.
Case Report: We report a case of 18-year-old male who sustained impalement injury to thigh with an iron rod after falling from height. After quick assessment of vital parameters and ruling out major organ injury, wound extent was examined. In collaboration with vascular and plastic surgeons, therod was successfully removed under direct vision. The patient recuperated without sequelae.
Conclusion: One should not get distracted by the appearance of the impalement injuries. After initial resuscitation, full trauma evaluation should be carried out before attending to local injury. Minimal manipulation, extraction of impaled object in operation theater under direct vision, wound debridement, and administration of antibiotics to prevent wound infection are pearls of the management of impalement injury.
Keywords: Penetrating injuries, metal rod, extremity involvement.
Introduction
Impalement injuries are one of the severe types of injuries combining effects of both penetrating and blunt trauma leading to crush injury, wound contamination, and multi organ damage [1,2,3,4,5].These types of injuries are usually a result of fall from height, vehicular accidents, and slip with strong external force [1,3,5]. These injuries are uncommon [1,2,4, 5, 6] and review of literature reveals only occasional case reports. Management of such injuries demands specific pre-hospital care, transportation, minimal handling, prevention of infection, anticipating the potential intra operative complications,and managing them effectively with appropriate surgical specialties [1,2,4,5,7].We report successful management of impalement injury to thigh,with review of literature.
Case Report
An 18-year-old male fell from a height of 15 feet at construction site over rusted iron rod which penetrated through his left upper thigh. The rod was cut with a saw to facilitate transport to hospital. On presentation, he was conscious, well oriented, and hemodynamically stable (GCS-E4M6V5). The patient didnot have any other major injury except abrasions over left forearm,elbow, and left lower back. Entry wound of the rod was through the posteromedial aspect of the left upper thigh, with an exit through anterolateral aspect of thigh(Fig. 1 and 2).
Patient’s distal pulsations were well felt. No attempts were made to remove the rod in the procedure room. PlainX-rays of thigh confirmed trajectory of rod(Fig. 3 and 4). Complete hemogram, arterial blood gas analysis, and serum electrolytes were all within normal limits. The patient was taken in the operation theaterkeeping a team of vascular and plastic surgeons stand by. General anesthesia was administered in right lateral position (Fig. 5). The exit wound of the rodwas extendedand soft tissue dissection was carried out to make the rod free from the adjacent neurovascular structures (Fig. 6). We found that rod had penetrated vastus medialis and sartorius muscle through substance, femoral and profundal vessels were just medial to it. We checked for any breach in vessel lumen and inspected nerves carefully by exploring them proximally and distally. Neurovascular structures were found to be intact. In deeper dissection, rodwas found between adductor group of muscles on one side and femoral bone on another. Once we were sure of integrity of neurovascular structures, the protruding part of the rod was gently pulled posteriorly along its length through wound track, with continuous monitoring of the distal pulsations.
Multiple side holes were created on a wide bore drain tube with scissor; free end of this tube was attached to the anterior end of the rod and it was passed through the exit wound following railroad technique [8]. Fig.7Wash with copious amount of normal saline was given (Fig. 7).Both the wounds were closed primarily over negative suction drain. Iron rod was 15mm in breadth (Fig. 8and 9).Broad-spectrum antibiotics were administeredalong with booster dose of tetanus and anti-tetanus serum. Wound check was clean and suture lines were dry on the 3rd and 6thpost-operative day. The patient was dischargedon the7thday postoperatively. There were no signs of wound infection even at 1-year follow-up.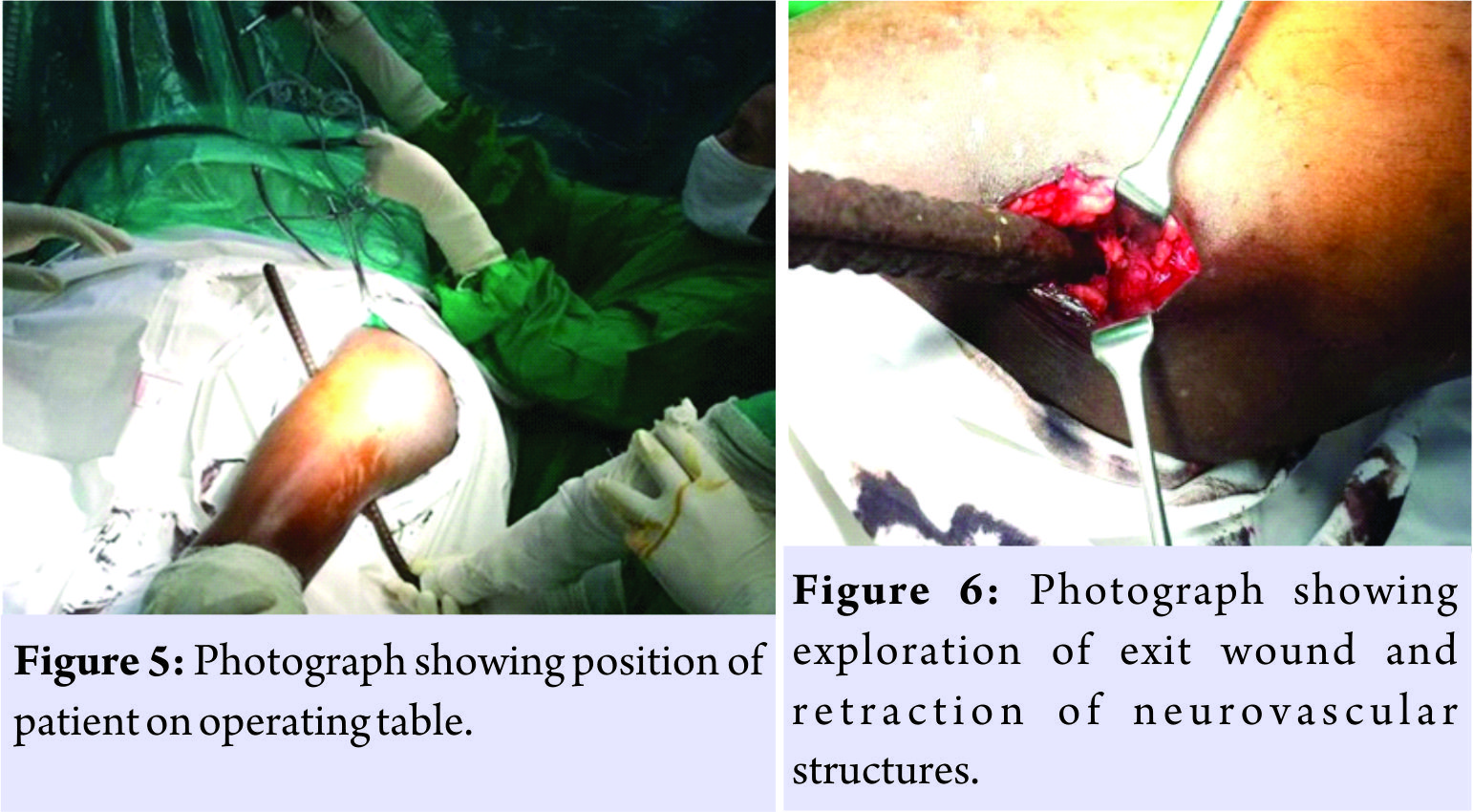
Discussion
Impalement injuries are relatively rare [1, 2, 4, 5, 6]. Ketterhagen and Wassermann [1] described two cases, one thigh impalement by tree branch and the other thoracoabdominal impalement in vehicular accident. Horowitz et al. [2] presented successful management of trunk impalement by iron rod. Bajaj et al. [6] presented a series of four cases stressing the need to individualize management in every case. Kelly et al. [7] studied a series of impalement injuries, three involving extremities and one of thoracoabdominal injury. Since then, many authors have reported individual experiences in the form of case reports discussing principles of management. Impalement injury combines the effects of both penetrating as well as blunt trauma [1, 2, 3, 4, 5]. It causes crush injury, wound contamination, underlying organ injury, as well as neurovascular damage [3]. This type of injury usually results due to fall from height or vehicular accidents [1, 3, 5]. In our case, it was caused due to fall from height of 15 feet on rusted iron rod. In impalement injury, the degree of damage depends on the organs involved. Higher mortality rates are usually seen in thoracoabdominal injuries due to the involvement of vital organs such as heart, lungs, or major blood vessels [4, 5, 6, 7]. In extremity involvement, complications are usually restricted to particular limb and are non-fatal [6, 7]. Complex impalements are injuries where impaling object traps the patient and interferes with transport. Removal of impaling object should never be attempted outside operation theater [1, 2, 3, 4, 5, 7] as it may aggravate hemorrhage due to loss of tamponade effect. In our case, the iron rod was cut with saw before transfer; minimum handling should be done while cutting. On arrival at tertiary centre, initial assessment of such injuries should be on the principles of basic life support [1, 2, 7]. After initial resuscitation and ruling out vital organ damage, impalement site should be examined to know the extent of damage. There is a uniform agreement on emergency exploration of patients who remain hemodynamically unstable even after initial fluid resuscitation, without wasting time for radiological investigations [4, 9]. In stable patients, it is prudent to proceed with selective radiological investigations to know the extent of injury and trajectory of impaling object [2]. Patient position on operating table is dictated by impaling object dimensions and trajectory [1, 2, 7]. This is particularly relevant with respect to type of anesthesia to be given. Furthermore, since organs at more than one anatomic site are involved, surgical approach under the guidance of multispecialty surgical team [2, 7] is essential. In our case, due to rod position in thigh, supine, and sitting positions were ruled out. Hence, general anesthesia was administered in right lateral position with injured limb up. Surgical approach should take into account entry and exit wound [1, 2, 5] so as to allow the removal of object under direct vision [1, 2, 4, 7]. Ketterhagen and Wassermann [1] recommended a fistulotomy type of incision connecting entry and exit points carried down to the object. According to Bajaj et al. [6], it is not necessary to lay open the tract taken by impaling object in every case; irrigating the wound with normal saline by introducing a catheter in the tract is sufficient. The wound should be thoroughly debrided to remove all devitalized tissue and optimum wash with normal saline should be given [1, 2, 5, 7]. This is a very important measure to prevent wound infection. Early administration of broad-spectrum antibiotics covering both aerobic and anaerobic organisms is also essential [1, 2, 5]. Most of the times impalement injuries are field injuries and impaling objects are metal rods (iron) with soil contamination like our case; tetanus immunization should also be carried out as per guidelines [10] based on patient’s immunization status. Regular follow-up is needed to detect post-operative infections. Horowitz et al. [2] cautioned against the development of infections by unusual pathogens found in soil. In our patient, operative wound healed by primary intention and patient was asymptomatic at 1-year follow-up.
Conclusion
Impalement injuries require multidisciplinary approach. The management of each case has to be individualized. Extensive wound exposure, extraction under direct vision, adequate debridement, and antibiotic coverage are pearls of management.
Clinical Message
In impalement injury to extremity, the neurovascular examination is of primary importance. Wide exploration of wounds, extraction of impaling object under direct vision, thorough wound wash, and prevention of post-operative wound infection are effective steps of management of such injuries.
References
1. Ketterhagen JP, Wassermann DH. Impalement injuries: The preferred approach. J Trauma 1983;23:258-9.
2. Horowitz MD, Dove DB, Eismont FJ, Green BA. Impalement injuries. J Trauma 1985;25:914-6.
3. Oya S, Miyata K, Yuasa N, Takeuchi E, Goto Y, Miyake H, et al. Impalement injury to the left buttock with massive bleeding: A case report. Nagoya J Med Sci 2013;75:147-52.
4. Shikata H, Tsuchishima S, Sakamoto S, Nagayoshi Y, Shono S, Nishizawa H, et al. Recovery of an impalement and transfixion chest injury by a reinforced steel bar. Ann Thorac Cardiovasc Surg 2001;7:304-6.
5. Naito K, Obayashi O, Mogami A, Han C, Kaneko K. Impalement injury of the pelvis due to car brake pedal. Injury Extra 2008;39:11-3.
6. Bajaj HN, Rao PS, Kumar B. Impalement injuries. Arch Orthop Trauma Surg 1989;108:58-9.
7. Kelly IP, Attwood SE, Quilan W, Fox MJ. The management of impalement injury. Injury 1995;26:191-3.
8. Ullah S, Khan M. Modifications in rail road technique for rupture of male Urethra. J Post Grad Med Inst 1999;13:12-6.
9. Malla G, Basnet B, Vohra R, Herrforth C, Adhikari S, Bhandari A, et al. Thoraco-abdominal impalement injury: A case report. BMC Emerg Med 2014;14:7.
10. Center for Disease Control and Prevention Guidelines. Available from: https://www.cdc.gov/disasters/disease/tetanus.html.
 |
 |
 |
 |
| Dr. Santosh Banshelkikar | Dr. Binoti Sheth | Dr. Rakesh P. Dhake | Dr. Arvind Goregaonkar |
| How to Cite This Article: Banshelkikar SN, Sheth BA, Dhake RP, Goregaonkar AB. Impalement Injury to Thigh: A Case Report with Review of Literature. Journal of Orthopaedic Case Reports 2018 Jan-Feb; 8(1):.71-74 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


