
[box type=”bio”] Learning Point for this Article: [/box]
Osteonecrosis of the talus is a rare condition affecting fairly young people; MRI is the diagnostic method of choice, and core decompression with intraosseous stem cell injection provides a feasible treatment option for the early-stage talar osteonecrosis.
Case Report | Volume 8 | Issue 1 | JOCR Jan – Feb 2018 | Page 23-26| Mika T Nevalainen, Jussi P Repo, Maija Pesola, Jukka P Nyrhinen. DOI: 10.13107/jocr.2250-0685.982
Authors: Mika T Nevalainen[1],[3], Jussi P Repo[2], Maija Pesola[2], Jukka P Nyrhinen[2]
[1]Department of Radiology, Central Finland Central Hospital, Keskussairaalantie 19 Jyväskylä, 40620 Finland.
[2]Department of Orthopedics and Traumatology, Central Finland Central Hospital Keskussairaalantie 19, Jyväskylä, 40620 Finland.
[3]Medical Research Center, University of Oulu and Oulu University Hospital, P.O. Box 10, OYS 90029 Finland
Address of Correspondence:
Dr. Mika T Nevalainen,
Medical Research Center, University of Oulu and Oulu University Hospital, P.O. Box 10, OYS 90029 Finland.
E-mail: mika.nevalainen@oulu.fi
Abstract
Introduction: Osteonecrosis of the talus is a fairly rare condition. Many predisposing factors have been identified including previous trauma, use of corticosteroids, alcoholism, and smoking. As a gold standard, magnetic resonance imaging (MRI) is the most sensitive and specific diagnostic examination to detect osteonecrosis. While many treatment options for talar osteonecrosis exist, core decompression is suggested on young patients with good outcome results. More recently, intraosseous stem cell and platelet-rich plasma (PRP) injection has been added to the core decompression procedure.
Case Report: We report a successful treatment of early talar osteonecrosis ARCO I (Association Research Circulation Osseous) by core decompression combined with stem cell and PRP injection. On 3-month and 15-month follow-up, MRI showed complete resolution of the osteonecrotic changes together with clinical improvement.
Conclusion: This modified technique is a viable treatment option for early talar osteonecrosis. Nevertheless, future prospects should include a study comparing this combined technique with plain core decompression.
Keywords: Core decompression, magnetic resonance imaging, osteonecrosis, stem cell, talus.
Introduction
Talar osteonecrosis is a fairly uncommon entity caused by the disruption of the blood supply to the talus [1]. Talus is predisposed to osteonecrosis due to its unique anatomy, distinctive extraosseous arterial circulation, and variable intraosseous blood supply [1, 2]. Both traumatic and atraumatic causes behind the osteonecrosis of the talus have been identified. Traumatic causes constitute of 75% of the cases and involve talar fracture and dislocation of the talar neck [3]. Atraumatic causes generally include the use of corticosteroids, alcoholism, or smoking, but on some occasions also systemic lupus erythematosus, renal transplant, sickle cell anemia, and thrombophilias can lead to osteonecrosis [1]. Idiopathic cases of talar osteonecrosis have been described too. On radiographs, talar osteonecrosis can be seen as increased talar dome opacity (sclerosis) with surrounding radiolucent rim. Subsequent crescent subchondral lucency (crescent sign), deformity, and ultimately articular collapse are late manifestations of the talar osteonecrosis [1, 4, 5, 6]. Magnetic resonance imaging (MRI) is the superior imaging modality to detect osteonecrosis in early stages with sensitivity and specificity up to 99% [7]. On MRI, the typical initial findings consist of patchy bone marrow edema (increased signal on T2-weighted/fluid-sensitive sequences and decreased signal on T1-weighted images). Later, as radiographic sclerosis develops in the infarcted bone, corresponding low signal on both T1- and T2-weighted images can be detected. The reparative zone between necrotic tissue and viable granulation tissue represents the “double-line sign,” a low-signal rim in which the inner aspect becomes high signal on T2-weighted images [4, 8]. Many classification systems for osteonecrosis exist, and the Association Research Circulation Osseous (ARCO) system was selected for this case report [9]. To the orthopedic surgeon, the osteonecrosis of the talus represents a dilemma; while several treatment options exist, the outcomes have remained suboptimal [10]. Moreover, while a plethora of treatment choices is available – including restricted weight-bearing, bracing, bone grafting, core decompression, talectomy, and arthrodesis – no consensus for the ideal treatment strategy for the talar osteonecrosis exists [10]. Here, we report a successful treatment of early osteonecrosis of the talus (ARCO Stage I) using core decompression combined with intraosseous stem cell and platelet-rich plasma (PRP) injection. This technique has been introduced by Hernigou and Beaujean mainly to treat osteonecrosis of the femoral head [11]. To the best of our knowledge, no prior literature exists where this modified technique had been used to treat talar osteonecrosis.
Case report
A 45-year-old man (treated from 11/2014 to 06/2016) with hypertension and hypothyroidism medications had twisted his right ankle while walking his dog. Primarily, he presented edema around the lateral malleolus, and no fracture was detected on radiographs (figure not shown); thus, conservative treatment with ankle brace was initiated. The pain in the ankle persisted for 3 months, and subsequent follow-up radiographs, and eventually MRI of the ankle was performed.
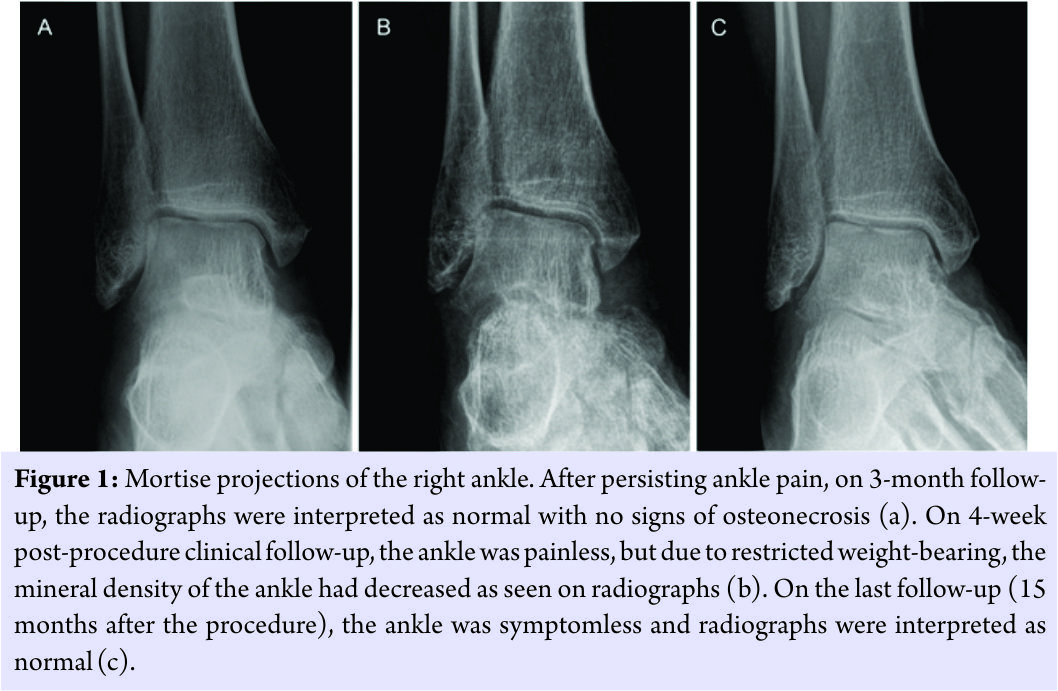
The radiographs were normal (Fig. 1a),but the MRI revealed ARCO Stage I osteonecrosis of the talus with increased signal on T2-weighted fat-saturated images and decreased signal on T1-weighted images; an additional minor crescent sign was also present (Fig. 2a and b). Due to the persisting pain and poor strain tolerance, core decompression with stem cell and PRP injection was performed using GPS® III (Gravitational Platelet Separation System; Zimmer-Biomet, Warsaw, Indiana, USA) and BioCUE BMA (Bone Marrow Aspirate [BMA] Concentration System; Zimmer-Biomet, Warsaw, Indiana, USA) systems. First, 30 ml of venous blood (including 3 ml of anticoagulant) was collected from the patient and centrifuged for 15 min. Accordingly, 3 ml of PRP was recovered from the centrifuged sample. In operating room under general anesthesia, autologous aspiration of bone marrow-derived stem cells from the right anterior iliac crest was carried out by an orthopedic surgeon. In total, 60 ml of BMA was collected and subsequently centrifuged for 15 min producing 6 ml of concentrated BMA. Finally, the PRP and BMA were mixed producing a total of 9 ml of the injectate. A stab incision on the anteroinferior edge of the medial malleolus was performed, and on fluoroscopic control, a guidance spike was directed into the talus to the region of the osteonecrosis.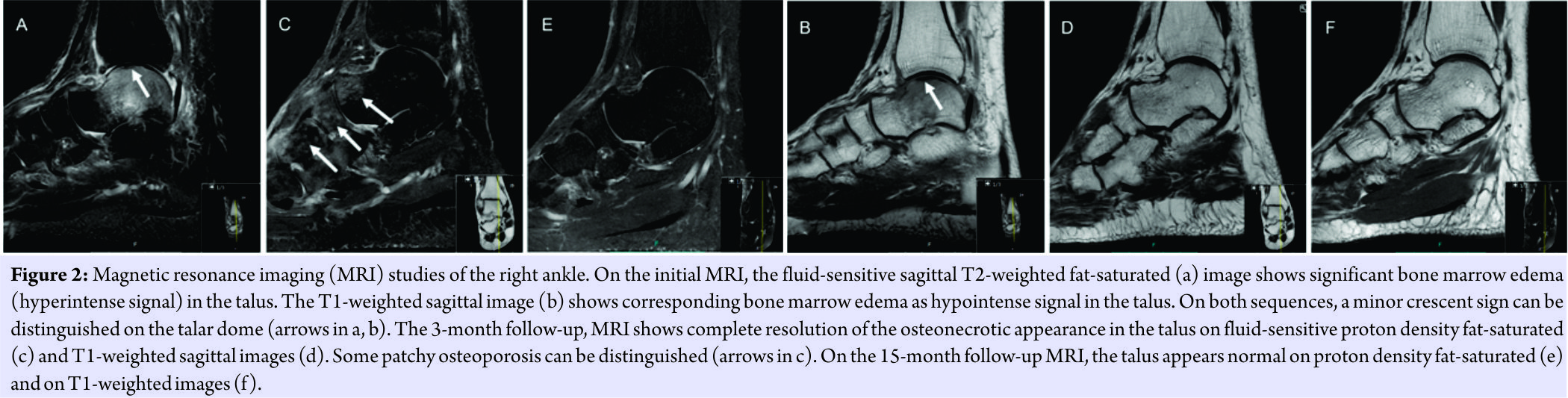 A 2.7 mm cannulated drill was used to provide core decompression. Routine histopathological specimens were not produced due to typical findings of osteonecrosis on MRI. Next, the PRP-BMA concoction was injected into the osteonecrotic region under fluoroscopic control using a 3 mm aspiration needle (Fig. 3). The incision wound was closed and full weight-bearing was restricted for 4 weeks with free mobilization of the ankle. On 4-week clinical follow-up, the patient presented no pain in the right ankle. Radiographs were normal except for the low mineral density of the bones in general (Fig. 1b). On the 3-month follow-up, the patient had fully resumed to his daily activities and his ankle was symptomless. The MRI revealed virtually complete resolution of the talar osteonecrotic changes (Fig. 2c and d). On the subsequent 15-month follow-up, the patient presented no symptoms and the MRI scan (Fig. 2e and f) as well as the radiographs (Fig. 1c) were normal.
A 2.7 mm cannulated drill was used to provide core decompression. Routine histopathological specimens were not produced due to typical findings of osteonecrosis on MRI. Next, the PRP-BMA concoction was injected into the osteonecrotic region under fluoroscopic control using a 3 mm aspiration needle (Fig. 3). The incision wound was closed and full weight-bearing was restricted for 4 weeks with free mobilization of the ankle. On 4-week clinical follow-up, the patient presented no pain in the right ankle. Radiographs were normal except for the low mineral density of the bones in general (Fig. 1b). On the 3-month follow-up, the patient had fully resumed to his daily activities and his ankle was symptomless. The MRI revealed virtually complete resolution of the talar osteonecrotic changes (Fig. 2c and d). On the subsequent 15-month follow-up, the patient presented no symptoms and the MRI scan (Fig. 2e and f) as well as the radiographs (Fig. 1c) were normal.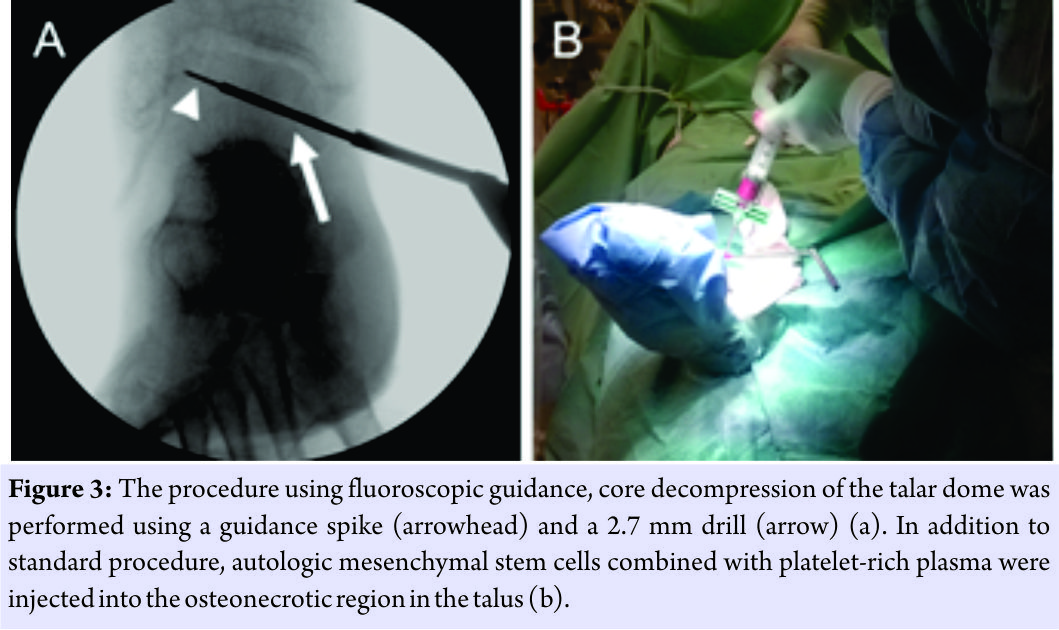
Discussion
The talus is uncommonly affected by osteonecrosis with an unknown incidence. Core decompression has been suggested as an alternative for the treatment of non-traumatic osteonecrosis of the talus without collapse by decreasing intraosseous pressure and promoting revascularization [12]. A study by Mont et al. concluded that core decompression is a feasible method of treatment for symptomatic osteonecrosis of the talus before collapse; at 7-year follow-up, 14 of the 17 ankles treated by core decompression had excellent or good result [13]. Another study also supported core decompression in symptomatic atraumatic talar osteonecrosis before collapse by reporting fair to excellent results in 29 of 32 patients [14]. A more recent study by Marulanda et al. depicted 44 ankles treated with core decompression, out of which 40 (91%) displayed good to excellent clinical outcomes in 4-year follow-up [15]. Overall, 28% of patients experience radiologic progression of the osteonecrosis [13, 14, 15]. Moreover, Issa et al. reported in their study that out of 85 ankles treated by core decompression only 17% demonstrated disease progression [16]. According to a fairly recent systematic review by Gross et al., the recapitulation of these results is that core decompression is an appropriate procedure in patients with early and late stage osteonecrosis secondary to atraumatic etiologies. However, further research is warranted to evaluate the role of core decompression in the treatment of traumatic talar osteonecrosis [10]. In addition to normal core decompression, Hernigou and Beaujean have introduced a method combining core decompression with intraosseous stem cell and PRP injection in the treatment of osteonecrosis of the femoral head [11]. Furthermore, two recent meta-analyses by Papakostidis et al. and Piuzzi et al. showed that on early-stage osteonecrosis of the femoral head the combined approach improves patients’ prognosis when compared to plain core decompression [17, 18]. Here, we have described a case with successful treatment of ARCO Stage I talar osteonecrosis using this combined technique. Initially, the patient presented a minor ankle sprain with persisting pain. The radiographs showed no diagnostic findings, and after definitive MRI diagnosis for early talar osteonecrosis, core decompression with stem cell and PRP injection was performed. Due to the typical MRI appearance of osteonecrosis, histopathological samples were not routinely collected. The differential diagnosis on this case might include insufficiency fracture of the talus and transient bone marrow edema, but since persisting pain and the crescent sign seen on MRI, ARCO Stage I osteonecrosis represents the most plausible diagnosis. On follow-up visits, the patient was symptomless and MRI findings of the osteonecrosis were seen to resolve.
Conclusion
We conclude that this modified technique is a viable option in the treatment of early talar osteonecrosis; however, future prospects should include a study comparing this combined technique with plain core decompression.
Clinical Message
Talar osteonecrosis is a fairly rare entity; however, MRI usually yields a definitive diagnosis. Since osteonecrosis is a progressive disease, treatment options should be considered with haste. Core decompression combined with intraosseous stem cell injection offers a feasible therapy option for the early talar osteonecrosis.
References
1. Pearce DH, Mongiardi CN, Fornasier VL, Daniels TR. Avascular necrosis of the talus: A pictorial essay. Radiographics 2005;25:399-410.
2. Mulfinger GL, Trueta J. The blood supply of the talus. J Bone Joint Surg Br 1970;52:160-7.
3. Adelaar RS, Madrian JR. Avascular necrosis of the talus. Orthop Clin North Am 2004;35:383-95.
4. Murphey MD, Foreman KL, Klassen-Fischer MK, Fox MG, Chung EM, Kransdorf MJ. From the radiologic pathology archives imaging of osteonecrosis: Radiologic-pathologic correlation. Radiographics 2014;34:1003-28.
5. Solomon L. Mechanisms of idiopathic osteonecrosis. Orthop Clin North Am 1985;16:655-67.
6. Resnick D, Sweet DE, Madewell JE. Osteonecrosis: Pathogenesis, diagnostic techniques, specific situations, and complications. In: Diagnosis of Bone and Joint Disorders. 4th ed. Philadelphia, PA: Saunders; 2002. p. 3599-685.
7. Lieberman JR, Berry DJ, Mont MA, Aaron RK, Callaghan JJ, Rajadhyaksha AD, et al. Osteonecrosis of the hip: Management in the 21st century. Instr Course Lect 2003;52:337-55.
8. Buchan CA, Pearce DH, Lau J, White LM. Imaging of postoperative avascular necrosis of the ankle and foot. Semin Musculoskelet Radiol 2012;16:192-204.
9. Mont MA, Marulanda GA, Jones LC, Saleh KJ, Gordon N, Hungerford DS, et al. Systematic analysis of classification systems for osteonecrosis of the femoral head. J Bone Joint Surg Am 2006;88 Suppl 3:16-26.
10. Gross CE, Haughom B, Chahal J, Holmes GB Jr. Treatments for avascular necrosis of the talus: A systematic review. Foot Ankle Spec 2014;7:387-97.
11. Hernigou P, Beaujean F. Treatment of osteonecrosis with autologous bone marrow grafting. Clin Orthop Relat Res 2002;405:14-23.
12. Léduc S, Clare MP, Laflamme GY, Walling AK. Posttraumatic avascular necrosis of the talus. Foot Ankle Clin 2008;13:753-65.
13. Mont MA, Schon LC, Hungerford MW, Hungerford DS. Avascular necrosis of the talus treated by core decompression. J Bone Joint Surg Am 1996;78:827-30.
14. Delanois RE, Mont MA, Yoon TR, Mizell M, Hungerford DS. Atraumatic osteonecrosis of the talus. J Bone Joint Surg Am 1998;80:529-36.
15. Marulanda GA, McGrath MS, Ulrich SD, Seyler TM, Delanois RE, Mont MA, et al. Percutaneous drilling for the treatment of atraumatic osteonecrosis of the ankle. J Foot Ankle Surg 2010;49:20-4.
16. Issa K, Naziri Q, Kapadia BH, Lamm BM, Jones LC, Mont MA, et al. Clinical characteristics of early-stage osteonecrosis of the ankle and treatment outcomes. J Bone Joint Surg Am 2014;96:e73.
17. Papakostidis C, Tosounidis TH, Jones E, Giannoudis PV. The role of “cell therapy” in osteonecrosis of the femoral head. A systematic review of the literature and meta-analysis of 7 studies. Acta Orthop 2016;87:72-8.
18. Piuzzi NS, Chahla J, Schrock JB, LaPrade RF, Pascual-Garrido C, Mont MA, et al. Evidence for the use of cell-based therapy for the treatment of osteonecrosis of the femoral head: A Systematic review of the literature. J Arthroplasty 2017;32:1698-708.
 |
 |
 |
 |
| Dr. Mika T Nevalainen | Dr. Jussi P Repo | Dr. Maija Pesola | Dr. Jukka P Nyrhinen |
| How to Cite This Article: Nevalainen M. T, Repo J. P, Pesola M, Nyrhinen J. P. Successful Treatment of Early Talar Osteonecrosis by Core Decompression Combined with Intraosseous Stem Cell Injection: A Case Report. Journal of Orthopaedic Case Reports 2018 Jan-Feb; 8(1): 23-26. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


