
[box type=”bio”] Learning Point for this Article: [/box]
After performing a total hip arthroplasty by a lateral approach this simple technique of passing sutures through bone tunnels can be used for reattachment of the capsule and abductor mechanism. This soft tissue restoration may lead to an earlier improvement in the patients gait during the post operative period.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 26-29| Sanjay Agarwala, Naeem Jagani. DOI: 10.13107/jocr.2250-0685.1034
Authors: Sanjay Agarwala[1], Naeem Jagani[2]
[1]Department of Orthopaedics and Trauma, P.D. Hinduja Hospital, Mahim – Mumbai. Maharashtra. India.
[2]Department of Arthroplasty and Trauma, P.D. Hinduja Hospital, Mahim – Mumbai. Maharashtra. India.
Address of Correspondence:
Dr. Sanjay Agarwala,
Department of Orthopaedics and Traumatology, P D Hinduja Hospital and Medical Research Centre, Mahim, Mumbai, Maharashtra. India.
E-mail: drsa2011@gmail.com
Abstract
Introduction: We describe a novel technique for approximation and reattachment of the capsule, hip abductors, and vastuslateralis muscles during closure of the arthrotomy and surgical wound, after total hip arthroplasty through a modified direct lateral approach. This anatomical restoration of soft tissues could thereby lead to early post-operative rehabilitation and recovery.
Case Report: This is a method of osteotendinous suturing that could lead to reestablishing the functional continuity of the gluteus minimus, medius muscles, and the anterior capsule through drill holes in the greater trochanter, and thereby preserve the integrity of the hip abductor musculature. This is a simple and easily reproducible technique of soft tissue approximation and reattachment that results in early mobilization and ambulation of the patient with no additional complications and have several advantages over the other methods used for closure.
Conclusion: This osteotendinous technique can be used for arthrotomy closure after both primary and revision total hip arthroplasties through the lateral approach (Hardinge and modified Hardinge) to the hip.
Keywords: Capsular repair, gluteus medius reattachment, hip abductor integrity, total hip replacement, transosseous suturing.
Introduction
In India, majority of the patients undergoing total hip arthroplasty (THA) are cases of arthritis of the hip joint secondary to osteonecrosis/avascular necrosis, seronegative arthritis, or secondary to trauma (fracture of the neck of the femur)[1]. The success of THA is dependent on several factors, which include appropriate patient and implant selection and meticulous surgical technique, one of which is closure of the arthrotomy and reestablishing soft tissue integrity. A watertight anatomical closure reduces the dead space, thereby causing a tamponade effect, thus reducing hematoma formation and also decreases the incidence of post-operative dislocations after THA [2, 3, 4]. The lateral approach involves cutting and reflecting the gluteus medius, minimus, and capsule anteriorly [5, 6, 7, 8].Various means such as metal clips or suture anchors may be used for the approximation of these structures. However, these are not cost-effective and have disadvantages such as infection and synovitis [9, 10, 11]. We describe a technique of drilling holes into the greater trochanter to prevent cut through of sutures and achieve better soft tissue approximation. Moreover, the tensor fascia lata is also closed with continuous sutures, thereby ensuring complete soft tissue restoration.
Case Report
The authors performed and used this technique in 160 total hip arthroplasties done in 12 months and the steps were the same in all the cases. 120 patients (48 female and 72 male) were available for a short-term review. All the included patients were Asian Indians and belonged to middle to high socioeconomic class. All patients presenting with a hip disorder warranting THA were included in our study, where this technique was used. All patients were followed up for 1 year.Suitable anesthesia was administered and the procedure was performed in the lateral position. A straight midlateral incision was used starting 5–6 cm proximal to the greater trochanter and extending approximately 7 cm distal to it on the lateral femoral shaft. A modified Hardinge type of lateral approach to the hip was used with the gluteus medius muscle being divided at the junction of its anterior one-third with its posterior two-third [8]. This was then extended distally over the lateral aspect of the greater trochanter upto the proximal part of the lateral femoral shaft, thereby dividing the proximal part of the vastuslateralis muscle. External rotation of the limb exposes the anterior capsule of the hip along with the anterior neck and calcar region. A “T”-shaped incision was made on the anterior capsule with the vertical limb of the T along the intertrochanteric line and the horizontal limb across the anterior surface of the capsule to the acetabular rim. The capsule is retained and retracted using Steinman pins[8]. After making a neck cut and extraction of the femoral head access to the acetabulum is achieved and appropriate retractors are placed. After implantation of an uncemented acetabular cup and liner, it is packed and the femoral preparation is performed. Three drill holes are made in the anterior and lateral part of the greater trochanter after marking their positions with an electrocautery (Fig. 1 and 2).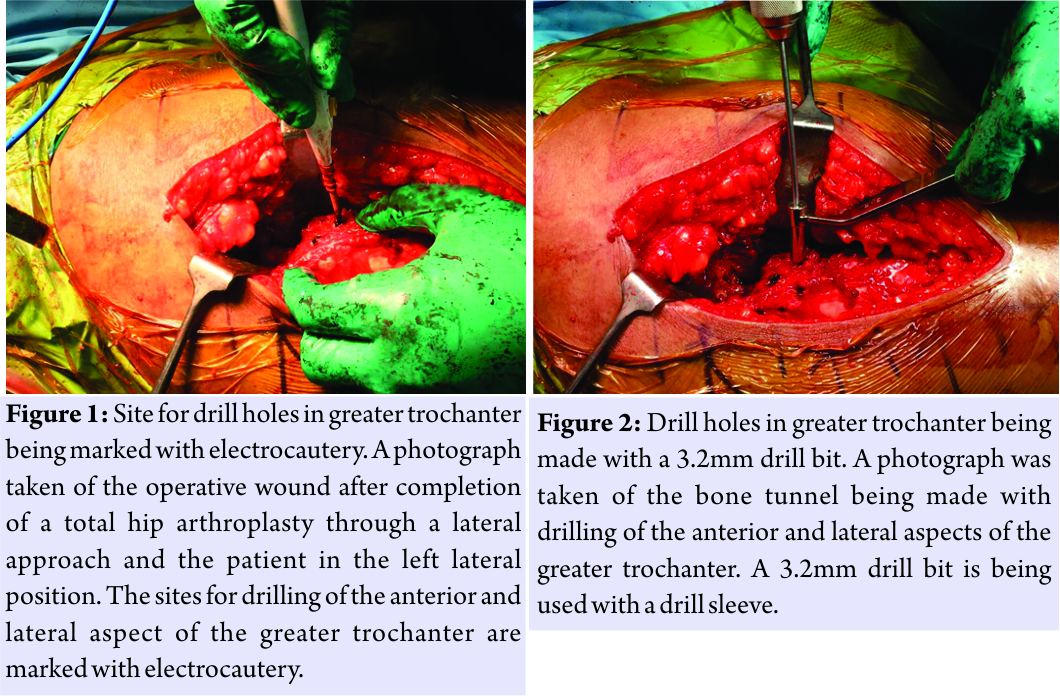 These are then connected through the curved tips of a towel clamp to form a curved tunnel for later passage of the suture needle(Fig. 3 and 7).
These are then connected through the curved tips of a towel clamp to form a curved tunnel for later passage of the suture needle(Fig. 3 and 7).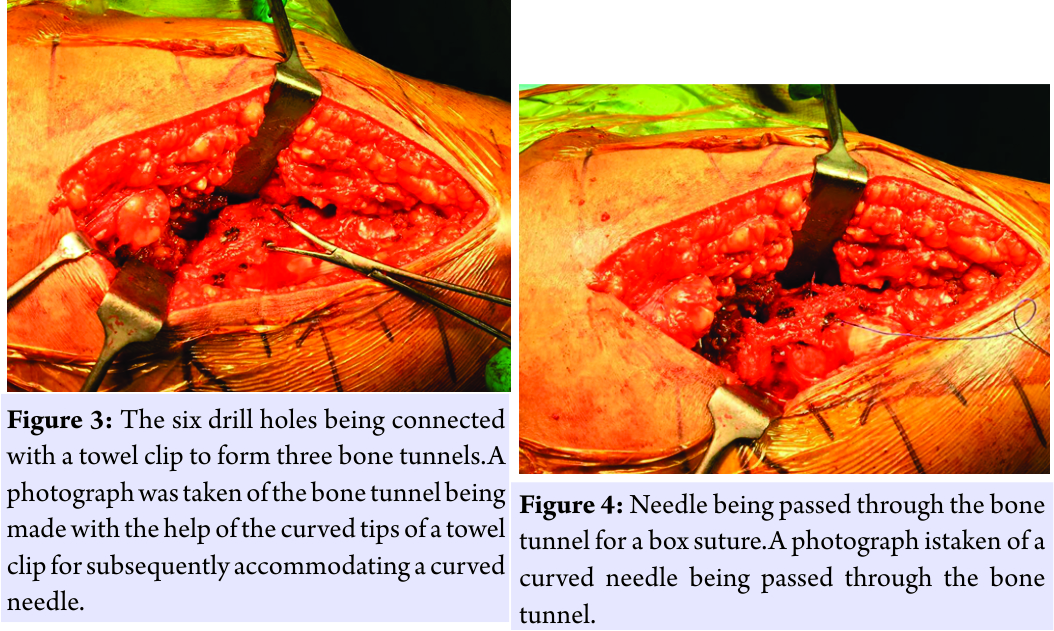 An uncemented stem is implanted followed by the implantation of the head, which is then reduced and its stability, offsets, and length are checked, a thorough wash given and closure begun in layers. Alternatively, these drill holes for the bone tunnels may be made after the final femoral stem is inserted. The closure is done with the hip in slight abduction and internal rotation in the following sequence. Two to three interrupted stiches are taken to oppose the horizontal limb of the hip joint capsule. A box suture is then taken in the greater trochanter through the proximal bone tunnel with No.1 polyglactin 910 suture on a reverse cutting needle (Fig. 4)(other suture material,namely, No. 5 polybutylate coated braided polyester fiber may also be used) [8]. The vertical limb of the distalcapsule along with theabductor muscles is reattached to the greater trochanter by this proximal box suture (Fig. 5).
An uncemented stem is implanted followed by the implantation of the head, which is then reduced and its stability, offsets, and length are checked, a thorough wash given and closure begun in layers. Alternatively, these drill holes for the bone tunnels may be made after the final femoral stem is inserted. The closure is done with the hip in slight abduction and internal rotation in the following sequence. Two to three interrupted stiches are taken to oppose the horizontal limb of the hip joint capsule. A box suture is then taken in the greater trochanter through the proximal bone tunnel with No.1 polyglactin 910 suture on a reverse cutting needle (Fig. 4)(other suture material,namely, No. 5 polybutylate coated braided polyester fiber may also be used) [8]. The vertical limb of the distalcapsule along with theabductor muscles is reattached to the greater trochanter by this proximal box suture (Fig. 5).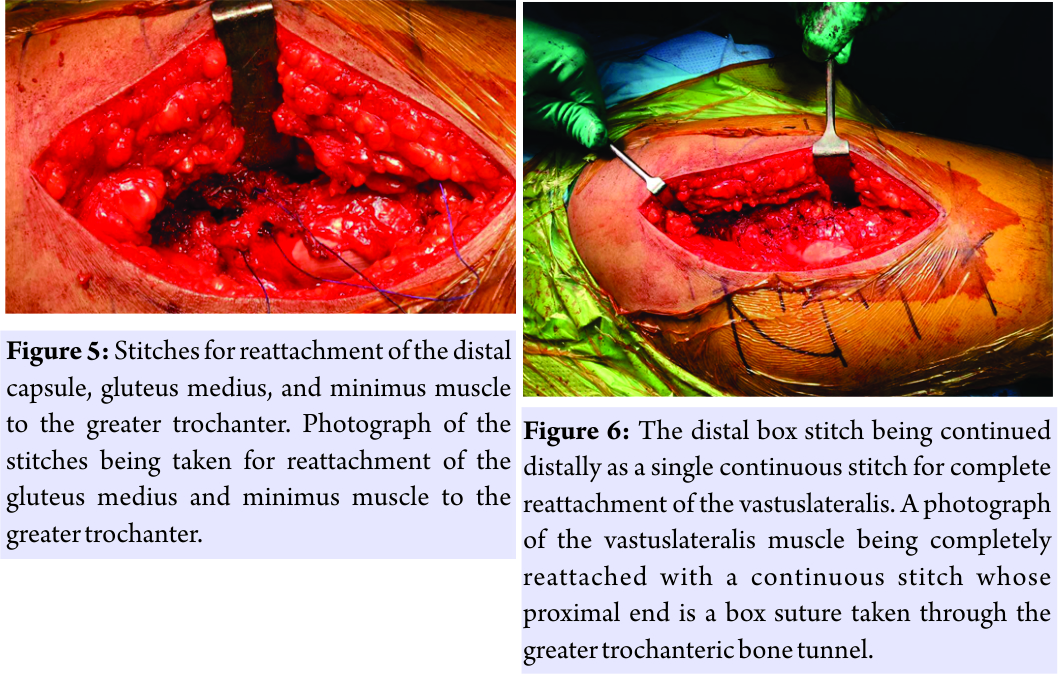 A continuous interlocking suture is then taken from this box suture till the proximal division of gluteus medius and minimus. Additional box suturesare taken at the mid and inferior drill holes in the greater trochanter with the remainder of the gluteus medius–vastuslateralis confluence. A continuous interlocking suture is then taken from the inferior-most box suture till the distal division of vastuslateralis (Fig. 6). After taking a continuous suture through the tensor fascia lata, the subcutaneous closure is done with interrupted No.1 polyglactin suture and then interrupted subcuticular sutures are taken with absorbable undyed braided 2–0 polyglactin 910 with a reverse cutting needle.
A continuous interlocking suture is then taken from this box suture till the proximal division of gluteus medius and minimus. Additional box suturesare taken at the mid and inferior drill holes in the greater trochanter with the remainder of the gluteus medius–vastuslateralis confluence. A continuous interlocking suture is then taken from the inferior-most box suture till the distal division of vastuslateralis (Fig. 6). After taking a continuous suture through the tensor fascia lata, the subcutaneous closure is done with interrupted No.1 polyglactin suture and then interrupted subcuticular sutures are taken with absorbable undyed braided 2–0 polyglactin 910 with a reverse cutting needle.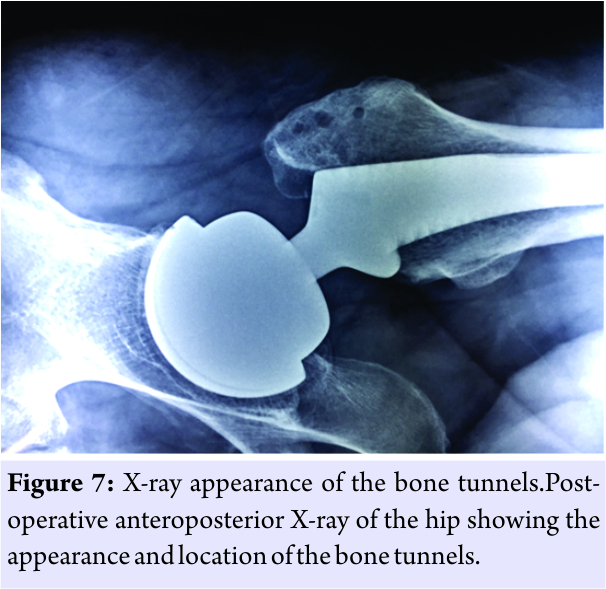
Discussion
Total hip arthroplasties are most commonly performed through the direct lateral or the posterior approaches [12]. The posterior approach is historically thought to have a higher dislocation rate which to some extent is mitigated by meticulous soft tissue repair[2, 3, 4].The direct lateral approach and its variants are associated with a higher rate of Trendelenburg gait/test in the short-term [13]. There are several types of lateral approaches to the hip such as the Ganz approach or the hemi-trochanterotomy approach; most of which involve reestablishing the abductor mechanism by reattachment of the divided greater trochanteric fragment [14, 15, 16]. Screws or cerclage wires may be used for this, and thence, these procedures are liable to being complicated by non-union of the greater trochanteric fragment [14]. These approaches are not commonly used for primary THA. The anterior approach,on the other hand, requires greater surgical expertise and has a longer learning curve compared to the lateral approach and may also require special table attachments and longer operative times [17]. We use a modification of the Hardinge approach as described by Pai [8] wherein we divide the gluteus medius at the junction of its anterior and middle-third. The salient features of this approach in contrast to the Hardinge approach are splitting gluteus medius at the junction of the anterior and middle third, and thus a large portion of the posterior 2/3 of the gluteus medius remains undisturbed at its point of insertion on the greater trochanter. The superior extension of the abductor split is only 3 cm, maintaining a safe distance from the inferior branch of superior gluteal nerve. A “T”-shaped incision is made on the anterior capsule with the vertical limb of the T along the intertrochanteric line and the horizontal limb across the anterior surface of the capsule to the acetabular rim. The capsule is retained and retracted using Steinman pins. With the posterior capsule intact and the anterior capsule repaired, this modification gives soft tissue protection against dislocation. The gluteus-vastus flap is repaired to the bone to prevent avulsion of the flap from the bone. In contrast to the Hardinge approach, the patient is placed in lateral decubitus [8]. The modified direct lateral offers predictable and easy access to the hip joint and provides excellent exposure of both acetabular and proximal femoral regions [13]. In our series, there were no cases of dislocation and post-operative limp was not a major problem. The Trendelenburg gait was absent in 62% of patients by the 6th week and 88% of patients by 12 weeks in our study. Passing sutures only through the soft tissues place a lot of stress on the tissues and the sutures tend to cut out. Hence, the technique of passing sutures through the tendon and into the bone tunnel was applied here. Suture anchors can supplant this technique. The bone tunnel and suture anchor techniques have their own advantages and disadvantages. The bone tunnel technique is the conventional method used since many years in areas like the ankle for ligament repair and for suturing external rotators in hip replacement through the posterior approach [18, 19]. This method is stronger, more secure, has remote chances of cut out of sutures without any additional increase in the cost of surgery[20]. Suture anchors are relatively expensive, with chances of pull out of anchors, anchor breakage, metal irritation, sterile inflammation, and infection [20]. Bioabsorbable anchors which are a more desirable alternative to metallic fixation are advantageous in that they reduce the complications associated with the use of metal [21]. However, bioabsorbable suture anchors are associated with serous discharge, synovitis [9, 10, 11],and cannot be visualized on radiographs. Osteotendinous closure of the abductor musculature with either absorbable No.1 polyglactin 910 suture or non-absorbable No. 5 polybutylate coated braided polyester fiber (Ethibond) [8] enhances reparation and accelerates tendon healing. This,thereby, enables early and enhanced post-operative recovery and earlier disappearance of the Trendelenburg gait.
Conclusion
We recommend this technique of closure in patients after performing a THA through a lateral approach using the Hardinge or modified Hardinge method. Prospective randomized studies are necessary to confirm the functional benefit of this procedure.
Clinical Message
Since the lateral approaches to the hip are associated with detachment of the hip abductor musculature, this method of osteotendinous suturing helps in reestablishing the soft tissue anatomy and muscular continuity and thereby helps in early ambulation and disappearance of Trendelenburg gait postoperatively.
References
1. Jain V, Dhal AK, Dhaon BK, Pradhan G. Deep vein thrombosis after total hip arthroplasty in Indian patients with and without enoxaparin. J Orthop Surg (Hong Kong) 2004;12:173-7.
2. van Stralen GM, Struben PJ, van Loon CJ. The incidence of dislocation after primary total hip arthroplasty using posterior approach with posterior soft-tissue repair. Arch Orthop Trauma Surg 2003;123:219-22.
3. Ranawat CS, Meftah M, Potter HG, Ranawat AS. The posterior approach in THR: Assuring capsular stability. Healio Orthop 2011;32:660.
4. Suh KT, Park BG, Choi YJ. A posterior approach to primary total hip arthroplasty with soft tissue repair. Clin Orthop Relat Res 2004;418:162-7.
5. Mulliken BD, Rorabeck CH, Bourne RB, Nayak N. A modified direct lateral approach in total hip arthroplasty: A comprehensive review. J Arthroplasty 1998;13:737-47.
6. Hungerford DS. Surgical approach in THA: The direct lateral approach is more practical and appealing. J Arthroplasty 2000;15:867-70.
7. Hardinge K. The direct lateral approach to the hip. J Bone Joint Surg Br 1982;64:17-9.
8. Pai VS. A modified direct lateral approach in total hip arthroplasty. J Orthop Surg 2002;10:35-9.
9. Agarwala S, Sharoff L, Chaudhari S. Osteotendinous suturing for anchorage of medial arthrotomy in total knee arthroplasty. Open J Orthop 2016;6:357-62.
10. Nho SJ, Provencher MT, Seroyer ST, Romeo AA. Bioabsorbable anchors in glenohumeral shoulder surgery. Arthroscopy 2009;25:788-93.
11. Freehill MQ, Harms DJ, Huber SM, Atlihan D, Buss DD. Poly-L-lactic acid tack synovitis after arthroscopic stabilization of the shoulder. Am J Sports Med 2003;31:643-7.
12. Byström S, Espehaug B, Furnes O, Havelin LI, Norwegian Arthroplasty Register. Femoral head size is a risk factor for total hip luxation: A study of 42,987 primary hip arthroplasties from the Norwegian arthroplasty register. Acta Orthop Scand 2003;74:514-24.
13. Witzleb WC, Stephan L, Krummenauer F, Neuke A, Günther KP. Short-term outcome after posterior versus lateral surgical approach for total hip arthroplasty-A randomized clinical trial. Eur J Med Res 2009;14:256-63.
14. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U, et al. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-24.
15. Dall D. Exposure of the hip by anterior osteotomy of the greater trochanter. A modified anterolateral approach. J Bone Joint Surg Br 1986;68:382-6.
16. Steffann F, Prudhon JL, Puch JM, Ferreira A, Descamps L, Verdier R, et al. Trans trochanteric approach with coronal osteotomy of the great trochanter: A new technique for extra-capsular trochanteric fracture patients treated by total hip arthroplasty (THA) in elderly. SICOT J 2015;1:7.
17. Yue C, Kang P, Pei F. Comparison of direct anterior and lateral approaches in total hip arthroplasty: A Systematic review and meta-analysis (PRISMA). Medicine (Baltimore) 2015;94:e2126.
18. Li X, Killie H, Guerrero P, Busconi BD. Anatomical reconstruction for chronic lateral ankle instability in the high-demand athlete: Functional outcomes after the modified brostrom repair using suture anchors. Am J Sports Med 2009;37:488-94.
19. Sioen W, Simon JP, Labey L, Van Audekercke R. Posterior transosseous capsulotendinous repair in total hip arthroplasty: A cadaver study. J Bone Joint Surg Am 2002;84-A:1793-8.
20. Hu CY, Lee KB, Song EK, Kim MS, Park KS. Comparison of bone tunnel and suture anchor techniques in the modified broström procedure for chronic lateral ankle instability. Am J Sports Med 2013;41:1877-84.
21. Kim MK, Na SI, Lee JM, Park JY. Comparison of bioabsorbable suture anchor fixation on the tibial side for anterior cruciate ligament reconstruction using free soft tissue graft: Experimental laboratory study on porcine bone. Yonsei Med J 2014;55:760-5.
 |
 |
| Dr. Sanjay Agarwala | Dr. Naeem Jagani |
| How to Cite This Article: Agarwala S, Jagani N. Osteotendinous Suturing for Anchorage of Hip Abductor Mechanism in Total Hip Arthroplasty through a Lateral Approach: A Technical Note. Journal of Orthopaedic Case Reports 2018. Mar- Apr; 8(2): 26-29. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


