
[box type=”bio”] Learning Point for this Article: [/box]
Hydatic cysts can rarely be observed in musculoskeletal tissue and often misdiagnosed. However, clinical outcome is good after successful surgery.
Case Report | Volume 8 | Issue 2 | JOCR Mar – Apr 2018 | Page 104-106| Levent Adiyeke, Tugrul Cakir, Tahir Mutlu Duymus, Suavi Aydogmus. DOI: 10.13107/jocr.2250-0685.1072
Authors: Levent Adiyeke[1], Tugrul Cakir[2], Tahir Mutlu Duymus[1], Suavi Aydogmus[1]
[1]Department of Orthopeadic Surgery Haydarpasa Numune Training and Research Hospital, Üsküdar, İstanbul.
[2]Department of Orthopeadic Surgery Antalya Training and Research Hospital, Antalya, Turkey.
Address of Correspondence:
Dr. Levent Adıyeke,
Haydarpasa Numune Training and Research Hospital, Tıbbiye Cad. No: 23 34668, Üsküdar, İstanbul.
E-mail: leventadiyeke@gmail.com
Abstract
Introduction: Primary hydatid cyst is rarely seen in musculoskeletal system. This paper presents a case of an intramuscular hydatid cyst in gluteal region.
Case of Report: We present the case of a 36-year-old woman affected by pain and a mass in her right gluteal region. Serological tests and radiographies were inconclusive. Ultrasonography showed a 52 mm × 47 mm diameter hypoechoic intramuscular cyst with septations. Computed tomography showed a cystic lesion located between muscle groups. The mass was excised under spinal anesthesia. It was a well-demarcated cystic lesion with 5 cm diameter. Albendazole chemotherapy was prescribed postoperatively.
Conclusion: Hydatid cysts must be considered in differential diagnosis in patients with cystic masses in musculoskeletal system, especially in patients living in endemic areas.
Keywords: Echinococcosis, gluteal region, hydatid cyst, primary.
Introduction
Echinococcosis or hydatidosis is a zoonosis caused by Echinococcus granulosus. As the parasite’s eggs continue life cycle in primary host (Canidae family members such as dog, wolf, and jackal) and intermediate host (herbivores such as sheep, goat, and beef), they were taken into gastrointestinal system of human. The larvae pass from intestines to liver and lungs which are the two most common sites of disease. Larvae rarely pass the physiological barriers and cause disease in brain, kidney, pancreas, diaphragm, and tissues like muscle. Primary hydatid cyst is very rarely seen in musculoskel et al system [1, 2]. We present a case of an intramuscular hydatid cyst in gluteal region.
Case Report
A 36-year-old woman affected by pain and a mass in her right gluteal region with a 2-year history was seen in outpatient clinic. She suffered from pain growing by walking and limited hip motion. Her examination revealed a mild erythema and a small swelling in contrast to her contralateral hip in gluteal region. In history, she was misdiagnosed in another center as having an abscess diagnosis and needle aspiration was made by local clinician. No pathological findings were seen radiolographies. Her serological test results were normal. Ultrasonography (USG) revealed a 52 mm × 47 mm diameter hypoechoic intramuscular cyst with septations. Computed tomography (CT) demonstrated a cystic lesion located in posterior muscle groups and extending inferiorly without bony involvement (Fig. 1).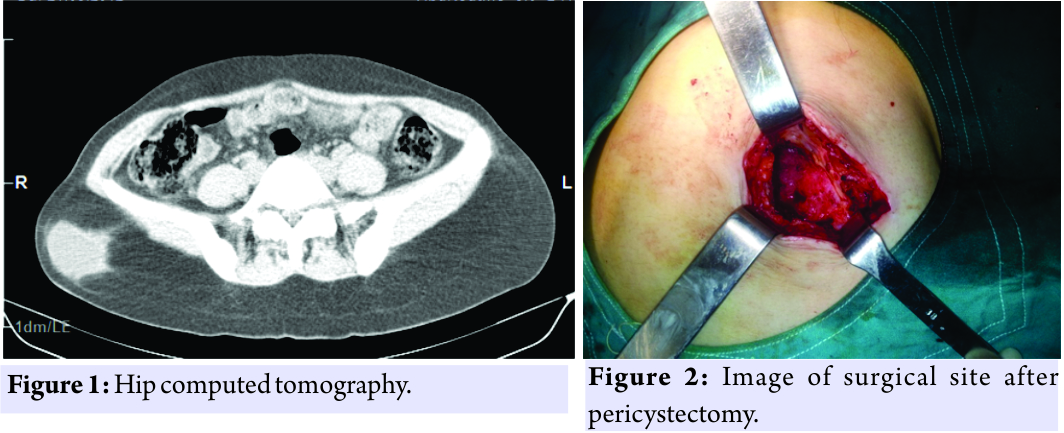 The findings were interpreted as hydatid cysts. The echinococcal indirect hemagglutination test (IHA) was found to be negative. However, this result was evaluated as false negative. Additional examinations were performed with the consideration that may be a tumor. No pathological findings were observed in abdominal USG and thoracic CT. She was operated under spinal anesthesia. A 5-cm diameter well-demarcated mass was found over the gluteal muscle tissue. Affected area was irrigated with povidone-iodine (betadine) for 5 minutes. Cyst was excised entirely. Surgical site was washed with hypertonic saline (Fig. 2). Later, the mass was intentionally ruptured, odorless, clear fluid, and daughter vesicles were observed. Biopsy was taken. Postoperatively, albendazole chemotherapy was prescribed. Biopsy was reported hydatid cyst as chitinous cuticular membrane and inflammation in the surrounding tissue (Fig. 3). She had no complaints at her latest follow-up.
The findings were interpreted as hydatid cysts. The echinococcal indirect hemagglutination test (IHA) was found to be negative. However, this result was evaluated as false negative. Additional examinations were performed with the consideration that may be a tumor. No pathological findings were observed in abdominal USG and thoracic CT. She was operated under spinal anesthesia. A 5-cm diameter well-demarcated mass was found over the gluteal muscle tissue. Affected area was irrigated with povidone-iodine (betadine) for 5 minutes. Cyst was excised entirely. Surgical site was washed with hypertonic saline (Fig. 2). Later, the mass was intentionally ruptured, odorless, clear fluid, and daughter vesicles were observed. Biopsy was taken. Postoperatively, albendazole chemotherapy was prescribed. Biopsy was reported hydatid cyst as chitinous cuticular membrane and inflammation in the surrounding tissue (Fig. 3). She had no complaints at her latest follow-up.
Discussion
Muscle tissue has a limited environment for growing of this lesion due to its contracting nature, also it has high lactic acid levels and the parasite has to cross physiological barriers of lung and liver. Hydatid cysts are rarely seen in musculoskeletal system, so hydatid cyst is less considered in differential diagnosis. Metastatic diseases, sarcoma, lipoma, giant cell tumor, malignant fibrous histiocytoma, abscess, mycotic infections, and tuberculosis must be considered in differential diagnosis of soft tissue masses [3, 4]. Hydatid cyst disease is usually diagnosed by serological and radiological studies. However, the diagnosis is challenging when the disease is primarily located in muscle tissue. Half of the primary intramuscular hydatidosis cases give a false negative [5] ın our case, IHA was negative preoperatively, we assume that antibody was not produced or diminished with time. History, clinical findings, examination, serological tests, and radiological studies should be evaluated together. Biopsy is not a primary diagnostic tool; it may cause local recurrence and anaphylaxis [6, 7]. Our patient was misdiagnosed previously and fine needle biopsy was performed, obviously, this did not harm. A lumber spinal magnetic resonance imaging (MRI) previously made reveals that the mass used to be larger 1 year before our diagnosis (Fig. 4). Treatment options for hydatid cyst are intracystic chemotherapatic injection and aspiration (puncture, aspiration, injection, and reaspiration), exclusive chemotherapy, and en bloc resection [8, 9, 10]. Recurrence is not very rare [11, 12, 13, 14]. We excised the entire cystic mass. During surgery, povidone-iodine irrigation and hypertonic saline wash were done to prevent any local recurrence. She had no symptoms at her 12-month follow-up.
Conclusion
In endemic areas like Turkey, hydatid cyst should be suspected when a cystic lesion is found in soft tissue. Fine needle biopsy must not be performed until serological tests, USG, and MRI exclude hydatid cyst.
Clinical Message
In endemic areas, hydatid cyst should be suspected when a cystic lesion is found in soft tissue.
References
1. Gougoulias NE, Varitimidis SE, Bargiotas KA, Dovas TN, Karydakis G, Dailiana ZH. Skeletal muscle hydatid cysts presenting as soft tissue masses. Hippokratia 2010;14:126-30.
2. Bouraoui IH, Essid O, Boughammoura H, Arifa N, Frikha R, Jemni H, et al. Forearm hydatid cyst: An unusual presentation. EMHJ 2011;17:994-5.
3. Parola P, Mathieu D, Panuel M. Hydatid bone disease. Clin Infect Dis 2000;31:543-4.
4. Eryılmaz MA, Eroğlu C, Karabağlı P, Çobankara OE. Gluteal hydatid cyst: Case report. Turkiye Klinikleri J Med Sci 2010;30:1380-3.
5. Durakbasa CU, Tireli GA, Sehiralti V, Sander S, Tosyali AN, Mutus M. An audit on pediatric hydatid disease of uncommon localization: İncidence, diagnosis, surgical approach, and outcome. J Pediatr Surg 2006;41:1457-63.
6. Bensghir M, Fjouji S, Bouhabba N, Ahtil R, Traore A, Azendour H. Anaphylactic shock during hydatid cyst surgery. Saudi J Anaesth 2012;6:161-4.
7. Park K, Jung S, Jang HC, Shin J. First successful puncture, aspiration, ınjection, and re-aspiration of hydatid cyst in the liver presenting with anaphylactic shock in Korea. Yonsei Med J 2009;50:717-20.
8. Bilgic S, Kose O, Sehirlioglu A, Safaz I, Ozkan H. Primary paraspinal hydatid cyst treated with puncture,aspiration, injection and re-aspiration (PAIR) technique: A case report. Eur Spine J 2009;18:S165-7.
9. Ormeci N, İdilman R, Akyar S, Palabiyikoglu M, Coban S, Erdem H. Hydatid cysts in muscle: A modified percutaneous treatment approach. Int J Infect Dis 2007;1:204-8.
10. Karahan N, Bülbül M, Sert S, Başpınar Ş, Kapucu N. Primary hydatid cyst located in gluteal muscle: A case report. Med J Kocatepe 2006;7:13-5.
11. Drimousis PG, Stamou KM, Koutras A, Tsekouras DK, Zografos D. Unusual site of recurrent musculoskeletal hydatid cyst: Case report and brief review of the literature. World J Gastroenterol 2006;12:5577-8.
12. La Greca G, Pulvirenti E, Gagliardo S, Sofia M, Russello D. Muscle-sparing approach for recurrent hydatidosis of the thigh and psoas: Report of a rare case. PLoS Negl Trop Dis 2011;5:840.
13. Demirbaş S, Sinan H, Kurt Y, Aydın Y, Yıldız M, Çelenk T. Primary ıntramuscular hydatid disease localized ın a lower extremity: A case report. Turkiye Klinikleri J Med Sci 2005;25:593-6.
14. Charalambous GK, Katergiannakis VA, Manouras AJ. Three cases of primary hydatidosis of the gluteus muscle: Our experience in clinical, diagnostic and treatment aspects. Chirurgia (Bucur) 2014;109:555-8.
 |
 |
 |
 |
| Dr. Levent Adiyeke | Dr. Tugrul Cakir | Dr. Tahir Mutlu Duymus | Dr. Suavi Aydogmus |
| How to Cite This Article: Adıyeke L, Cakır T, Duymus T M, Aydogmus S. Unexpected Diagnosis in Gluteal Region – A Primary Intramuscular Hydatid Cyst: A Case Report. Journal of Orthopaedic Case Reports 2018. Mar-Apr ; 8(2): 104-106. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


