
[box type=”bio”] Learning Point for the Article: [/box]
Limbus fracture must be considered as one of the differential diagnoses in an adolescent patient presenting with acute cauda equina syndrome.
Case Report | Volume 8 | Issue 4 | JOCR July – August 2018 | Page 38-40| Nigil Sadanandan Palliyil, Ravi Ranjan Rai, Kedar Deogaonkar. DOI: 10.13107/jocr.2250-0685.1150
Authors: Nigil Sadanandan Palliyil[1], Ravi Ranjan Rai[1], Kedar Deogaonkar[1]
[1]Department of Orthopaedics, P.D Hinduja National Hospital and Medical Research Centre, Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Nigil Sadanandan Palliyil,
Department of Orthopaedics,P.D Hinduja National Hospital and Medical Research Centre,Veer Savarkar Marg, Mahim, Mumbai – 400016, Maharashtra, India.
E-mail: nigilanand@hotmail.com
Abstract
Introduction: Limbus vertebral fracture is an uncommon injury described in adolescents. It refers to the separation of a bony fragment from the unfused ring apophysis of lumbar vertebral end plate. It usually presents with back pain with/without radiculopathy masquerading an acute disc prolapse. However, the presentation as acute cauda equina syndrome has seldom been reported.
Case Report: A 15-year-old male presented to the casualty with a history of acute-onset low back pain and bilateral lower limb radicular pain with weakness, after lifting of a heavy Indian musical instrument (Dholak). This was associated with urinary retention and numbness in perineal region. Examination revealed L5 and S1 weakness with absent ankle jerks bilaterally. Bulbocavernosus reflex was absent. Emergency magnetic resonance imaging imaging was done, which revealed a limbus fracture of cephalad part of L4 vertebral body with displaced fragment into the spinal canal causing compression of the cauda equina. Emergency surgery was done in the form of L3-L4 midline interlaminar microscopic decompression. The patient had complete neurological recovery including the bladder control within 1 month of surgery. The patient had no functional deficits during follow-up at 3 and6 months. Dynamic radiographs taken at the end of 6 months did not show any sign of instability.
Conclusion: When an adolescent patient with no previous history of backpain presents with acute cauda equina syndrome, a possibility of limbus fracture should also be considered. Early diagnosis and surgical decompression in such cases can bring about complete neurological recovery and excellent clinical outcome.
Keywords: Limbus fracture, cauda equina adolescent, vertebral epiphyseal separation.
Introduction
Limbus vertebral fracture/avulsed vertebral rim apophysis/slipped vertebral epiphysis is a rare entity found in adolescents, especially in athletes. It refers to the separation of a bony fragment from the cephalad or caudal edge of the vertebral body adjacent to the disc space where fusion between the ring apophysis and the adjacent vertebral body has not been completed. They usually present with back pain or radiculopathy masquerading an acute disc prolapse. Cauda equina syndrome secondary to this injury is extremely rare. We present a case of limbus vertebral fracture with cauda equina syndrome in a non-athlete adolescent boy.
Case Report
A 15-year-old boy presented to the casualty with a history of acute-onset low backpain and lower limb weakness after lifting of a heavy Indian musical instrument (Dholak).The patient had developed urinary retention since the time of injury. The patient had numbness, tingling sensation in both his lower limbs and was unable to stand or walk. Examination revealed Grade 0 power of bilateral ankle dorsiflexors, extensor hallucis longus, and extensor digitorum. He had Grade 3 power of ankle plantar flexors bilaterally. Ankle jerk was absent bilaterally. He had diminished sensations in L5 and sacral dermatomes. Bulbocavernosus reflex was absent. Emergency magnetic resonance imaging (MRI) imaging was done, which revealed a limbus fracture of cephalad part of L4 vertebral body with displaced fragment into the spinal canal severely compressing the cauda equina (Fig. 1 and 2). 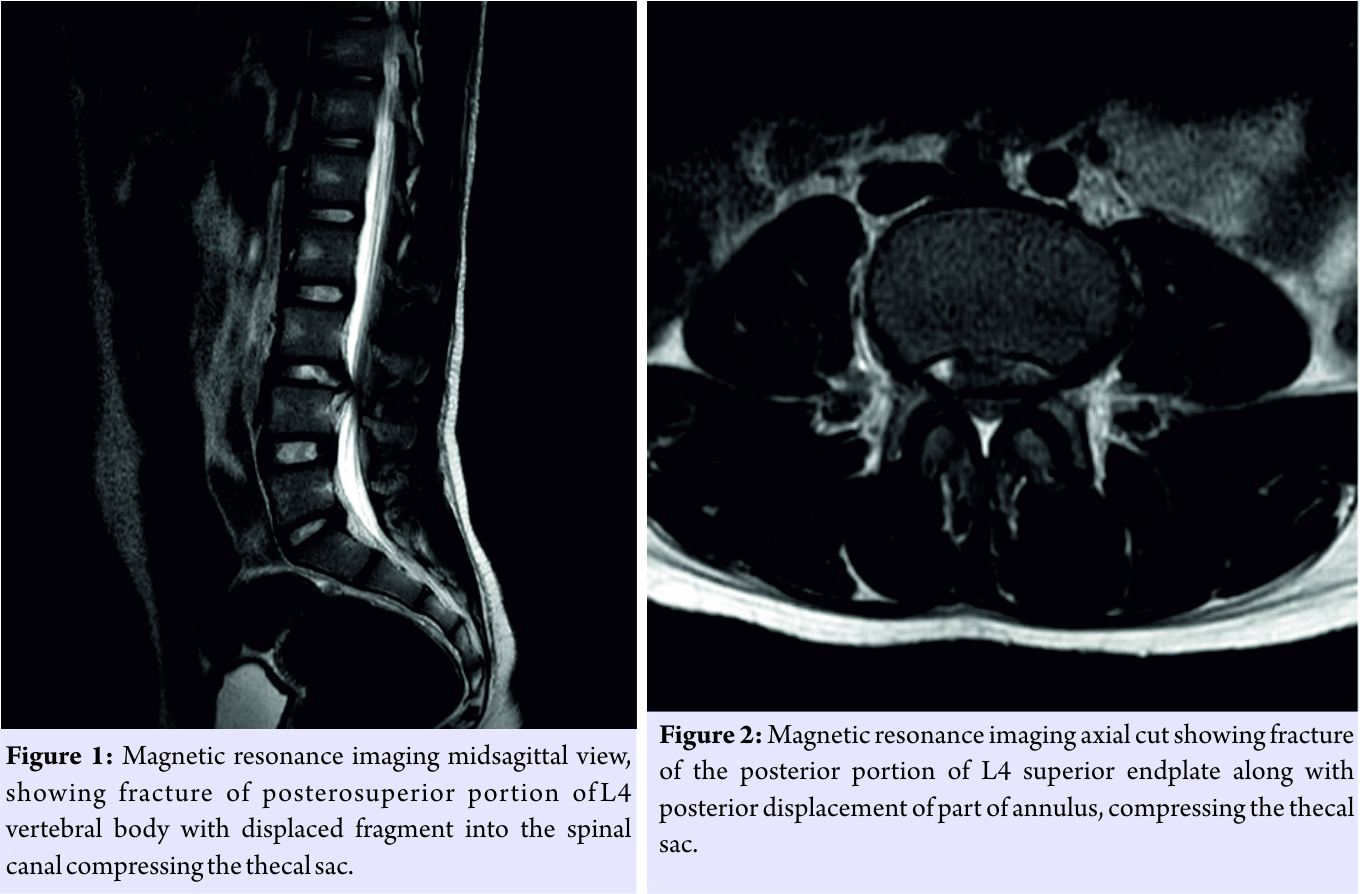 Emergency surgery was done in the form of L3-L4 midline interlaminar microscopic decompression. All loose and extruded disc fragments were removed. Bony bump was pushed back into position using a hockey stick punch. The patient showed signs of neurological recovery in the immediate post-operative period. The patient had complete neurological recovery including the bladder control within 1 month of surgery. He had no functional deficits during follow-up at 3-6 months. Dynamic radiographs taken at the end of 6 months did not show any sign of instability (Fig. 3).
Emergency surgery was done in the form of L3-L4 midline interlaminar microscopic decompression. All loose and extruded disc fragments were removed. Bony bump was pushed back into position using a hockey stick punch. The patient showed signs of neurological recovery in the immediate post-operative period. The patient had complete neurological recovery including the bladder control within 1 month of surgery. He had no functional deficits during follow-up at 3-6 months. Dynamic radiographs taken at the end of 6 months did not show any sign of instability (Fig. 3).
Discussion
Cauda equina syndrome is an uncommon diagnosis in adolescents. Etiology of cauda equina syndrome in this age group includes neoplasm, trauma, infection,and spinal dysraphism. Limbus fracture has rarely been reported as a cause of cauda equina syndrome[1]. It occurs more frequently in males(2.85:1) [2]. This could be explained by the greater degree of physical activity in males. It usually affects adolescent population and young adults as the fusion process between ring apophysis and vertebral end plate is not completed until the ages of 18–25 years [2]. Trauma, weightlifting, and gymnastics were the cause of fractures in more than half of patients in the study by Epstein and Epstein [3]. Different mechanisms have been described regarding the pathogenesis of this fracture: Hyperextension according to Keller[4] and and hyperflexion according to Nishijima et al. [5]. Most frequently affected vertebrae include L4, L5 and S1 [6]. The most common form of presentation is low back pain with/without radiculopathy. The presence of neurological deficits is quite rare [2]. The cause of neurological deficits could be related to the posterior displacement of the osseous fragment or because of the compressive effect of epidural hematoma [6]. Lateral radiograph may show a bony defect at the posterosuperior corner of the vertebral body. MRI sagittal view classically shows a hypointense signal in a “comma” or “7” shape indicating an avulsed bony fragment [6]. MRI also helps to rule out other causes including infection or tumor. Computed tomography (CT) scan is the best modality in identifying the bony fragments and is also helpful in classifying the fracture. Takata et al. have proposed a classification based on CT scan findings [7]. Type I is a simple separation of the posterior rim of the vertebra without osseous defect in the posterior part of the vertebral body. Type II is an avulsion fracture of the posterior rim of the vertebral body, including the overlying cartilage of the anulus fibrosus. Type III is a small fracture, posterior to an irregularity in the cartilage of the endplate. In this type of fracture, there is a round defect in the bone adjoining the fracture site. Epstein and Epstein described Type IV with a complete split and displacement of the posterior wall of the vertebral body [3]. As this fracture has quite rarely been reported in literature, there is lack of an agreed treatment plan [2]. Emergency surgical management is advocated in cases presenting with neurological deficits. There are controversies in the available literature on the surgical strategies including the choice of decompressive modalities, whether removal of apophyseal fragments or/and disc and the necessity of additional spinal fusion. Liquois et al. suggested that diskectomy is not to be performed in children in the absence of degenerative disc disease [8]. According to Takata et al., spinal fusion is only justified in Type II, where the bone fragment is largely attached to the posterior vertebral ligament and in cases where discectomy is also done along with laminectomy leading to spinal instability [7]. Decision regarding diskectomy and fusion is taken after considering the age, MRI finding, and type of bone lesions [6]. Most of the adolescent patients who were surgically treated for limbus fracture showed good to excellent results [2].
Conclusion
Limbus fracture, although rare, can present as acute cauda equina syndrome masquerading an acute disc prolapse in adolescents. Prompt recognition of the injury and timely surgical decompression can bring about complete neurological recovery and excellent clinical outcome.
Clinical Message
Limbus fracture, though uncommon, must be considered as one of the differential diagnoses in an adolescent patient presenting with acute cauda equina syndrome. Timely surgical intervention can bring about excellent neurological recovery.
References
1. Akhaddar A, Belfquih H, Oukabli M, Boucetta M. Posterior ring apophysis separation combined with lumbar disc herniation in adults: A 10-year experience in the surgical management of 87 cases. J Neurosurg Spine 2011;14:475-83. web link http://thejns.org/doi/abs/10.3171/2010.11.SPINE10392
2. Wu X, Ma W, Du H, Gurung K. A review of current treatment of lumbar posterior ring apophysis fracture with lumbar disc herniation. Eur Spine J 2013;22:475-88.
3. Epstein NE, Epstein JA. Limbus lumbar vertebral fractures in 27 adolescents and adults. Spine (Phila Pa 1976) 1991;16:962-6.
4. Keller RH. Traumatic displacement of the cartilaginous vertebral rim: A signof intervertebral disc prolapse. Radiology 1974;110:21-4. https://doi.org/10.1148/110.1.21
5. Nishijima M, Tatezaki S, Yamada H. Lumbar disc herniation with atraumatic fracture-dislocation of the end plate. Report of two cases. OrthopTrauma Surg1984;27:129-33.
6. Molina V, Court C, Dagher G, Pourjamasb B, Nordin JY. Fracture of the posterior margin of the lumbar spine: Case report after an acute, unique, and severe trauma. Spine (Phila Pa 1976) 2004;29:E565-7.
7. Takata K, Inoue S, Takahashi K. Fracture of the posterior margin of alumbar vertebral body. J Bone Joint Surg Am 1988;70:589-94. PMID – 3356726
8. Liquois F, Demay P, Filipe G. Sciatica caused by avulsion of the vertebral limbus in children. Rev ChirOrthopReparatriceAppar Mot 1997;83:210-6.
 |
 |
 |
| Dr. Nigil Sadanandan Palliyil | Dr. Ravi Ranjan Rai | Dr. Kedar Deogaonkar |
| How to Cite This Article: Palliyil N S, Rai R R, Deogaonkar K. Limbus Vertebral Fracture Presenting as Cauda Equina Syndrome Masquerading An Acute Disc Prolapse – A Rare Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2018 Jul-Aug; 8(4): 38-40 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


