
[box type=”bio”] Learning Point for the Article: [/box]
The article learning point is to treat patellofemoral instability in down’s children early. We showed our results with one modificated MPFL reconstruction
Case Report | Volume 8 | Issue 4 | JOCR July – August 2018 | Page 61-65| Alexandre Carneiro Bitar, Caio Oliveira D’Elia, Breno Schor, Jefferson Bertoni, Zan Mustacchi, Patricia Moreno Grangeiro. DOI: 10.13107/jocr.2250-0685.1162
Authors: Alexandre Carneiro Bitar[1], Caio Oliveira D’Elia[1], Breno Schor[1], Jefferson Bertoni[1], Zan Mustacchi[2], Patricia Moreno Grangeiro[1],[3]
[1]Instituto Vita (ou Vita Care), São Paulo, SP, Brazil.
[2]Center for Studies and Clinical Research of São Paulo (CEPEC-SP), São Paulo, SP, Brazil.
[3]Instituto de Ortopedia e Traumatologia, FMUSP, São Paulo, SP, Brazil.
Address of Correspondence:
Dr. Alexandre Carneiro Bitar,
Department of Orthopaedics, Master of Medical Sciences, Physician of the Shoulder and Knee Group at Instituto Vita, 106, Mato Grosso Street, 1 Floor, Higienópolis, 01239-010 – São Paulo – SP. Brazil.
E-mail: bitar@institutovita.com.br
Abstract
Introduction: We attended three skeletally immature patients with Down syndrome (DS) with complaints of severe patellofemoral instability and dislocated patella (preoperatively, Dugdale classification IV or V), in addition to low functional capacity, with falls during gait. The technique (lateral release, medial capsulectomy, reconstruction of the medial patellofemoral ligament (MPFL) with the patellar ligament and associated techniques, and some knees) and results in three children with DS and bilaterally dislocated patella were revealed.
Case Report: Our minimum follow-up was 27 months and maximum was 105 months (average of 64 months).All children improved gait, patellar stability, Kujala (58.13%), and subjective IDKC (40.55%) scores and improved the congruence and the trochlea groove angles.
Conclusion: The patellofemoral instability in children with DS is a challenge. We should use an arsenal of surgical techniques in this complex problem. We believe in early surgery to improve the formation of structures, especially in patients with gross instabilities and frequent falls. In all cases, we detected a weakness of medial components and lateral contracture, reconstructed the MPFL (we were the first researchers to describe this procedure for this group of patients), and performed a medial capsulectomy and lateral release. In some knees, intraoperatively, it was necessary to associate the reconstruction of the medial patellotibial ligament to improve instability. We consider fundamental analysis of the axis with panoramic radiographs and hemiepiphysiodes is in cases of asymmetric or severe valgus.
Keywords: Patellofemoral instability, dislocated patella, down syndrome.
Introduction
Down syndrome (DS) is one of the most common chromosomal abnormalities [1], and approximately 20% of patients with DS present with patellar instability [2]. Dugdale and Renshaw [3] evaluated a large number of patients with institutionalized DS(210) or not (150) for almost 30 years. Despite a retrospective study, the conservative management of patellar instabilities was recommended for years. Only in 2007 [4] and 2009 [1], researchers described specific techniques for children with DS with good results in small case series. Recent study[5] described the results in this group of patients with the Green quadricepsplasty technique associated to semitendinosus tenodesis in older patients (modified Galeazzi) in ten knees, with two cases of failure. However, none of the procedures described to treat DS patients used more recent anatomical concepts with the medial patellofemoral ligament (MPFL)[6, 7].This study presents the functional and radiographical results in three children (six knees) and describes the Camanho’s[8] reconstruction technique of MPFL with some modifications and associated procedures to treat DS patients with dislocated patella.
Case Report
We attended three skeletally immature patients with DS with complaints of severe patellofemoral instability and dislocated patella (preoperatively, Dugdale classification IV or V, according to Table 1), in addition to low functional capacity, with falls during gait. They were submitted to the same procedur A lateral release was performed and we conducted a capsulectomy of this exuberant tissue. Then, the associated MPFL reconstruction was performed with the medial strip of the patellar ligament (PL)[1] (Fig. 1 and2). This surgical technique was well described by Camanho et al. in 2007 [9]and it was also performed by Bitar et al. [10]. In some knees, we had to associate other techniques as follows: Elongation of the quadriceps and fixation of the new ligament with two anchors; modified Galeazzi technique with the reconstruction of the medial patellotibial ligament with the semitendinous maintained in the tibia; and the medial femoral hemiepiphysiodesis procedure. The episodes of patellar instability during follow-up (subluxation and/or dislocation),functional scores (subjective IKDC and Kujala), and radiographs which analyzed the trochlea dysplasia and patellar inclination before and after surgery were evaluated. There were performed radiographic forehead and absolute and axial profile incidences in the Merchant position with 45° of flexion. In evaluating the trochlear groove angle, we considered the trochlea to be flat when the angle was >150°. In evaluating the patellar congruence angle, we considered that lateral subluxation >11° or complete dislocation represented positive or altered values (Fig. 3)[9]. Minimum follow-up was 27 months and maximum was 105 months. Relatives of each patient were informed that data concerning the case would be submitted for publication and they agreed with this.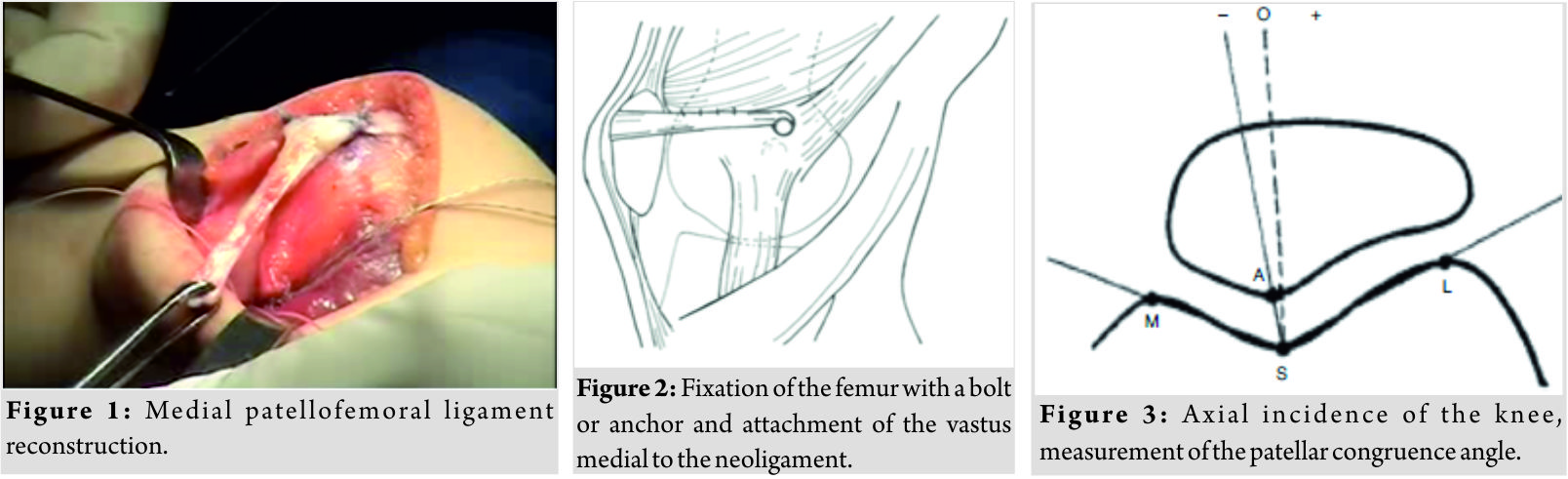
Case 1
The first patient was 8 years’ old, frequent falls, and bilateral patellofemoral instability. In the preoperative period, the patella of the right knee was dislocated and irreducible (Dugdale V) and the left knee was Dugdale IV. She was submitted to the surgical procedure in the right knee and 1year later in the left one (Fig. 4). We removed the anchors bilaterally in 2011, at the age of 12. No other procedure was necessary, and the functional results and family satisfaction were excellent.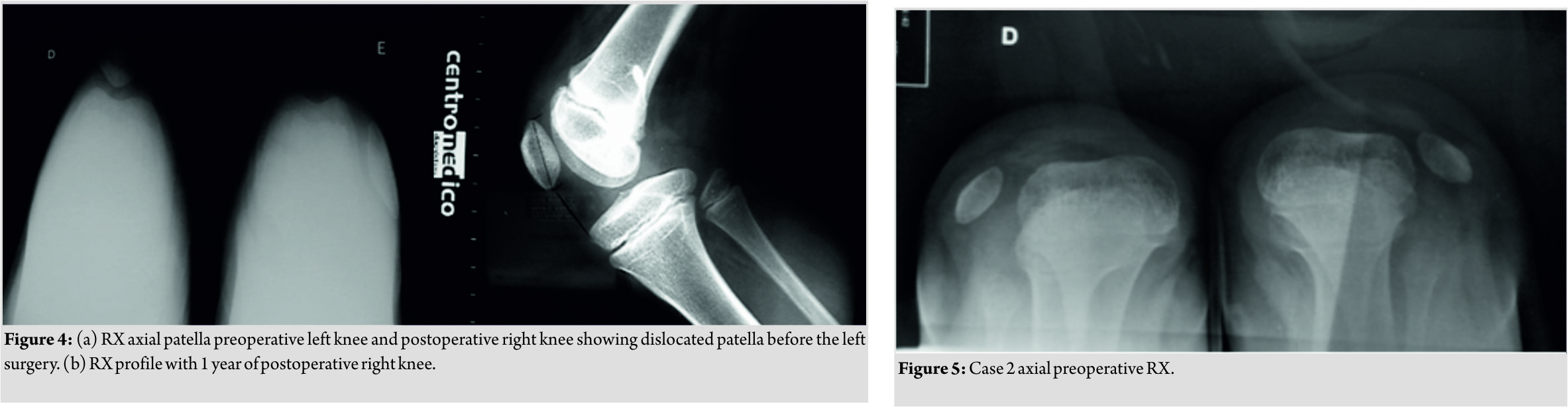
Case 2
The second child presented with a complaint of recurrent falls, bilateral valgus, bilateral significant femoral anteversion, and the two Dugdale V knees (Fig. 5). At 6 years of age, he was submitted to surgery in the right knee (2010) and in 2011 in the left. As in the right knee he still had subluxation of the patella, we performed in the left knee, an associated and modified Galeazzi procedure reconstructing the medial patellotibial ligament, leaving the semitendinosus inserted in the tibia, and setting the reconstruction with osseous points on the patella medially. After 3years, as valgus of the right knee increased and continued with dislocation in flexion, we performed bilateral medial femoral hemiepiphysiodesis procedure (Fig. 6 and 7). 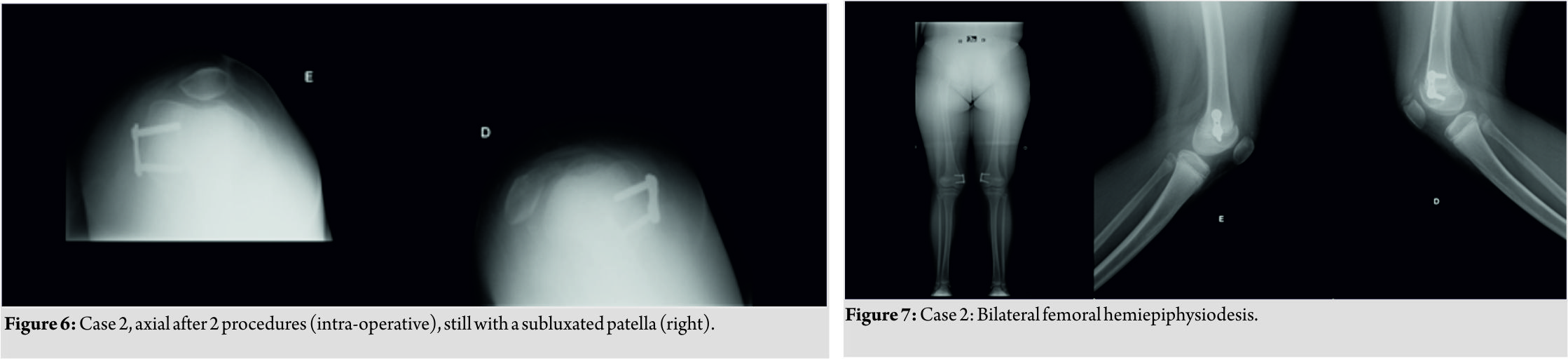 In 2015, we removed the plaque from the left knee and in 2016 from the right, with the improvement of the patella subluxation and formation of the trochlea (Fig. 8).
In 2015, we removed the plaque from the left knee and in 2016 from the right, with the improvement of the patella subluxation and formation of the trochlea (Fig. 8).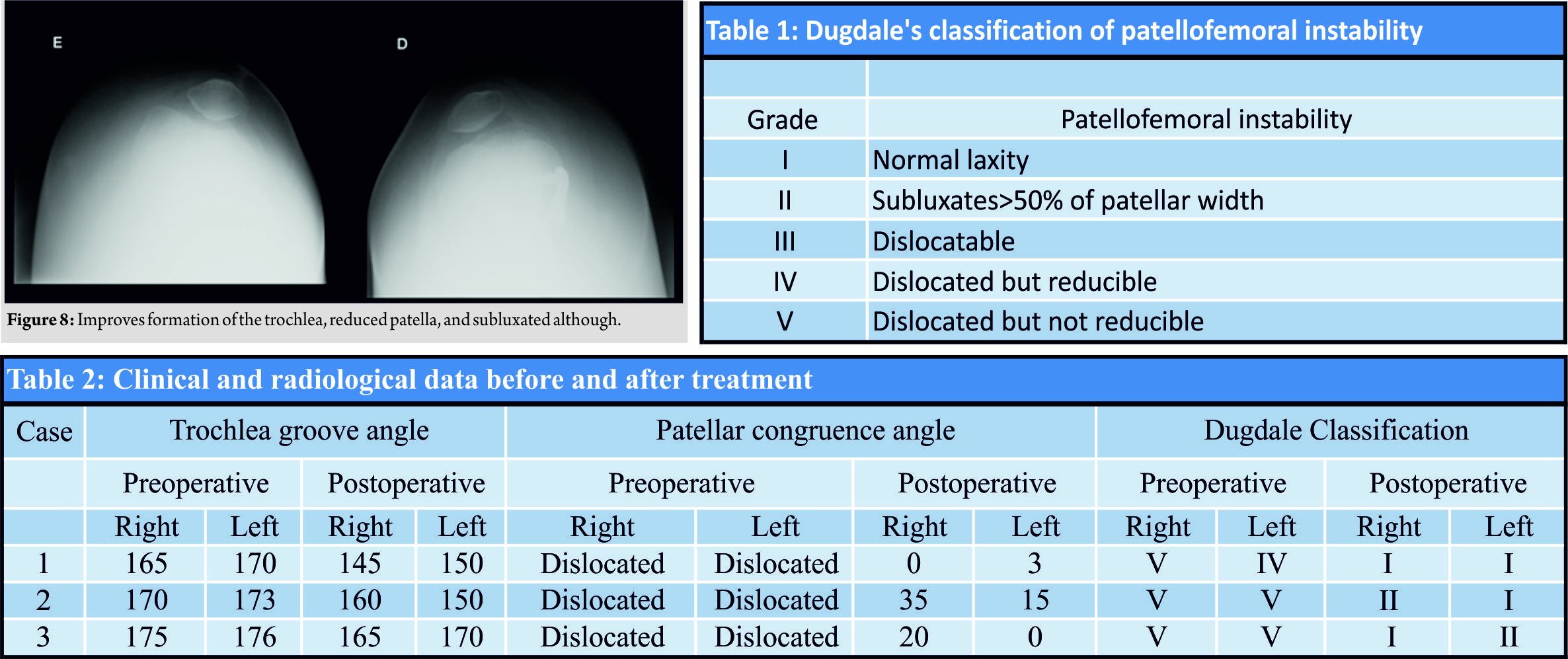
Case 3
The third patient, with a history of acute myeloid leukemia, presented both dislocated and irreducible knees (Dugdale V) and we performed a bilateral surgery. During evolution, the right knee remained centered with well-formed and clinically stable trochlea. The left knee was submitted to quadriceps stretching to center the patella intraoperatively and the trochlea still shallow. Clinically, it was possible to subluxate the patella. He was submitted to hemiepiphysiodesis of the left knee due to an asymmetric valgus. He is in follow-up and clinically better, plays soccer, and does not present falls, and he does not have more episodes of subluxation. Concerning all cases, before surgery, five of the six knees were classified as Dugdale V and one Dugdale IV. After the surgical procedure, five patients evolved with total reduction and clinical stability (Dugdale I) and one Dugdale II. All children improved gait and episodes of falls ceased. Kujala’s pre- and post-operative scores were 55.3 (the right and left knee) and 90 (right) and 85 (left), respectively. Pre- and post-operative subjective IKDC scores were 55.9 (right) and 55.5 (left); 76.6 (right) and 80.7 (left), respectively. Kujala’s scores improved 58.1% and subjective IKDC 40.6%. Minimum follow-up was 27 monthsandmaximumwas105 months (average of 64 months). The radiographic results showed an improvement in the angle of patellar congruence and the trochlear groove angle. Postoperatively, in addition to the reduced patellar angles, the mean angles of the patellar congruence were 18.3° on the right side and 6° on the left, with an overall mean of 12.16 (normal 11°). For the trochlea groove angle, the mean preoperative values were 171.5° and 156.7°, postoperatively (normal 150°), with an improvement of approximately 15°.All pre- and post-surgicalscores are shown in Table 2.
Discussion
In relation to the number of surgical cases and the techniques used, in general, the literature presents series with few patients and varied techniques. Dugdale and Renshaw[3] operated on five patients (eight knees), but only six knees used techniques to correct knee instability, with only 50% of good results. Mendez [11] presented 14 surgeries in ten patients through lateral release and imbrication of the medial capsule. In more severe cases, the release advanced proximally until the insertion of the vastus lateralis. In 11 knees, the transfer of the patellar tendon insertion was performed additionally without any bone correction surgery for valgus or correcting rotational components. Joo et al. [4], in 2007, presented a four-in-one procedure result in five patients (six knees) and not all with DS. Bettuzzi et al.[1], in 2009, performed the Roux-Goldthwait-Campbell technique in six children (10 knees), and finally, Kocon performed quadricepsplasty in eight patients (10 knees)using the technique modified by Green. In the study of Dugdale and Renshaw[3], patients had an average age of 12.5 years, ranging from 4 to 19 years, and in the study of Mendez[11], patients had a mean of 13.6 years (ranging 27 months to 17.5 years), much older than our series on the procedure date (mean 6.3 years, ranging from four to nine years). Our follow-up time was 27–105 months (average of 64 months), while Mendez [11] presented 67.2 months (ranging from 20 to 169) and Joo et al. [4] 54.5 months (31–66 months). In relation tobilaterality, our three patients presented Dugdale IV or V in both knees, unlike the other studies (30–50% bilateral variation in surgical cases), different from other studies[1,3, 4, 5, 11] in which Dugdale III cases were mixed. Although studies have shown that not all patients with severe patellar instability exhibit symptoms of falling, pain, or functional disability, it was evident that our patients benefited from the surgeries according to reports and scores filled by their relatives. The medial patellar patellofemoral ligament (MPFL) is the main lateral restrictor of the patella[12, 13, 14]. Although some studies show good results with MPFL reconstruction techniques in children and mainly adults, this is the first work that uses the updated concept of MPFL in children with DS. We used a technique that is a variation on the original technique of Camanho et al.[8], which we believed that it is possible to treat both patients with acute lesions[15] and those with chronic instability. Another point for discussion about the variety of procedures is to associate the reconstruction of the medial patellotibial ligament described by Philipot et al.[9]. We used this in one knee of one patient and are waiting for the evolution of another to indicate this technique. We believe that, similar to the concepts of hip dysplasia, the reduction of the patella is an important factor in the formation of the trochlea and surgeries should be performed as early as possible in those who walk and have symptoms of instability and falls, in addition to radiographic changes of patellar instability. The youngest patient was 3.9-year-old at the time of surgery. All of them improved the radiographic parameters after the procedures. Preoperative panoramic radiography should be evaluated to associate hemiepiphysiodesis or not (three knees in this study) and in some cases (only one case in our series) to associate to medial patellotibial ligament reconstruction. The weaknesses of this study are the non-evaluation of osteoarthritis in the long term, a small number of cases and the association of techniques in some cases, and different associated procedures in some knees.
Conclusion
The patellofemoral instability in children with DS is a challenge. We should use an arsenal of surgical techniques in this complex problem. We believe in early surgery to improve the formation of structures, especially in patients with gross instabilities and frequent falls. In all cases, we detected a weakness of medial components and lateral contracture, reconstructed the MPFL (we were the first researchers to describe this procedure for this group of patients), and performed a medial capsulectomy and lateral release. In some knees, intraoperatively, it was necessary to associate reconstruction of the medial patellotibial ligament to improve instability. We consider fundamental analysis of the axis with panoramic radiographs and hemiepiphysiodesis in cases of asymmetric or severe valgus.
Clinical Message
We use a early MPFL reconstruction (Camanho’s modified technique) with lateral release and medial capsulectomy in all children with patellar instability and DS. We associated techniques (MPFL and medial femoral hemiepiphysiodesis) in some cases. The clinical and radiological results are good. The precoce procedure and analysis of the axis are very important to achieve these results.
References
1. Bettuzzi C, Lampasi M, Magnani M, Donzelli O. Surgical treatment of patellar dislocation in children with Down syndrome: A 3- to 11-year follow-up study. Knee Surg Sports TraumatolArthrosc2009;17:334-40.
2. Mik G, Gholve PA, Scher DM, Widmann RF, Green DW. Down syndrome: Orthopedic issues. CurrOpinPediatr2008;20:30-6.
3. Dugdale TW, Renshaw TS. Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-13.
4. Joo SY, Park KB, Kim BR, Park HW, Kim HW. The ‘four-in-one’ procedure for habitual dislocation of the patella in children: Early results in patients with severe generalised ligamentous laxity and aplasis of the trochlear groove. J Bone Joint Surg Br 2007;89:1645-9.
5. Kocon H, Kabacyj M, Zgoda M. The results of the operative treatment of patellar instability in children with Down’ syndrome. J PediatrOrthop B 2012;21:407-10.
6. Steiner TM, Torga-Spak R, Teitge RA. Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia. Am J Sports Med 2006;34:1254-61.
7. Deie M, Ochi M, Sumen Y, Yasumoto M, Kobayashi K, Kimura H, et al. Reconstruction of the medial patellofemoral ligament for the treatment of habitual or recurrent dislocation of the patella in children. J Bone Joint Surg Br 2003;85:887-90.
8. Camanho GL, Bitar AC, Hernandez AJ, Olivi R. Medial patellofemoral ligament reconstruction: A novel technique using the patellar ligament. Arthroscopy 2007;23:108.e1-4.
9. Moreira TA, Demange MK, Gobbi RG, Mustacchi Z, Pécora JR, Lírico LE, et al. Trochlea dysplasia and patellar instability in patients with Down’s syndrome. Rev Bras Ortop2015;50:159-63.
10. Philipot R, Boyer B, Testa R, Farizon F, Moyen B. The role of medial ligamentous structures on patellar tracking during knee flexion. Knee Surg Sports TraumatolArthrosc2012;20:331-6.
11. Mendez AA, Keret D, MacEwen GD. Treatment of patellofemoral instability in Down’s syndrome. Clin OrthopRelat Res 1988;234:148-58.
12. Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65.
13. Tuxøe JI, Teir M, Winge S, Nielsen PL. The medial patellofemoral ligament: A dissection study. Knee Surg Sports TraumatolArthrosc2002;10:138-40.
14. Sandmeier RH, Burks RT, Bachus KN, Billings A. The effect of reconstruction of the medial patellofemoral ligament on patellar tracking. Am J Sports Med 2000;28:345-9.
15. Bitar AC, Demange MK, D’Elia CO, Camanho GL. Traumatic patelar dislocation: Nonoperative treatment compared with MPFL reconstruction using Patellar tendon. Am J Sports Med 2012;40:114-22.
 |
 |
 |
 |
 |
 |
| Dr. Alexandre Carneiro Bitar | Dr. Caio Oliveira D’Elia | Dr. Breno Schor | Dr. Jefferson Bertoni | Dr. Zan Mustacchi | Dr. Patricia Moreno Grangeiro |
| How to Cite This Article: Bitar AC, D’Elia CO, Schor B, Bertoni J, Mustacchi Z, Grangeiro PM. Clinical and Radiologic Outcomes of the Surgical Treatment of Patellofemoral Instability in Children with Down Syndrome and Dislocated Patella: Case Series. Journal of Orthopaedic Case Reports 2018 Jul-Aug; 8(4):61-65 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


