
[box type=”bio”] Learning Point of the Article: [/box]
Complex floating knee in the presence of a previous implant creates an unusual fracture pattern which poses a unique challenge in management and subsequent rehabilitation.
Case Report | Volume 9 | Issue 3 | JOCR May-June 2019 | Page 79-83 | Gaurav Saini, R K Sen, Anoop Kalia, Sagar Kadam. DOI: 10.13107/jocr.2250-0685.1432
Authors: Gaurav Saini[1], R K Sen[1], Anoop Kalia[1], Sagar Kadam[1]
[1]Department of Orthopaedics, Max Super Speciality Hospital, Mohali, Punjab, India.
Address of Correspondence:
Dr. Anoop Kalia,
Department of Orthopaedics, Max Super Speciality Hospital, Mohali, Punjab, India.
E-mail: kaliaanoop@gmail.com
Abstract
Introduction: Complex floating knee in the presence of a previous implant creates an unusual fracture pattern which is a rare entity and poses a unique challenge in management and subsequent rehabilitation.
Case Report: A 56-year-old psychiatric patient who jumped from height had a polytrauma and a floating knee injury. Following the primary care and damage control surgery with knee-spanning fixator at some other centers, he was shifted to us on ventilator care and was directly admitted to intensive care unit for further management. On presentation, it was a floating knee injury with gross comminution of both femur and tibia with associated Hoffa with bent implant in situ. It was managed by plating of both lower end femur and tibia and at the end of 6 months, showed a satisfactory outcome.
Conclusion: Floating knee injuries further complicated by the presence of the previous implant in a polytrauma situation poses a unique challenge which requires meticulous surgical planning and prolonged rehabilitation to achieve satisfactory outcome.
Keywords: Floating knee, Hoffa, polytrauma.
Introduction
Floating knee injury is a high-velocity trauma and can be associated with systemic injuries to chest, abdomen, or head [1] or local complications in the form of injury to neurovascular structures [2], or knee ligamentous disruption [1] or there can be compounding [3]. Floating knee in a previous operated limb is a difficult situation and further, if the implant is in situ, it poses a unique challenge. This case report highlights such a scenario. The precise incidence of floating knee is not known, it is a relatively uncommon injury and the presence of associated Hoffa fracture with floating knee is a rare entity. The largest series of floating knee consists of 222 patients over an 11-year period [4]. Hoffa fractures were first described as a coronal fracture of femoral condyle by Friedrich Busch but were later named by Albert Hoffa in 1904. Hoffa fracture can involve either condyle but most commonly involve lateral condyle [5]. The exact mechanism of Hoffa fracture is not known. Lewis et al. [6] suggested that axial load applied to the knee when the knee is in 90° or more flexion produces posterior tangential fractures.
Case Report
A 56-year-old diabetic, hypertensive man on antipsychotic medications who jumped from about 30 feet height, sustained polytrauma and was admitted in a local hospital. After initial resuscitation and advanced trauma life support (ATLS) care, he was intubated and put on ventilator support. He was diagnosed with bilateral hemothorax and his right lower limb X-rays showed fracture lower one-third femur with extensive metadiaphyseal comminution and fracture ipsilateral proximal tibia extending to metaphysis. A locking distal femoral locking plate was present and had bent (Fig. 1). As per records, he had 3*2 cm wound on anterior aspect of thigh which was thoroughly washed, debrided, and sutured and damage control [7]surgery was done in the form of knee-spanning fixator (Fig. 2) and the patient was put on intravenous antibiotics. He stayed in the intensive care unit (ICU) for 7 days, after which he was shifted to our center. As a part of repeat evaluation, all his necessary X-rays were retaken (Fig. 3) which revealed resolution happening in bilateral hemothorax. The right lower limb X-rays revealed knee-spanning external fixator with fracture of lower end femur and proximal end tibia with bent implant in situ (Fig. 2).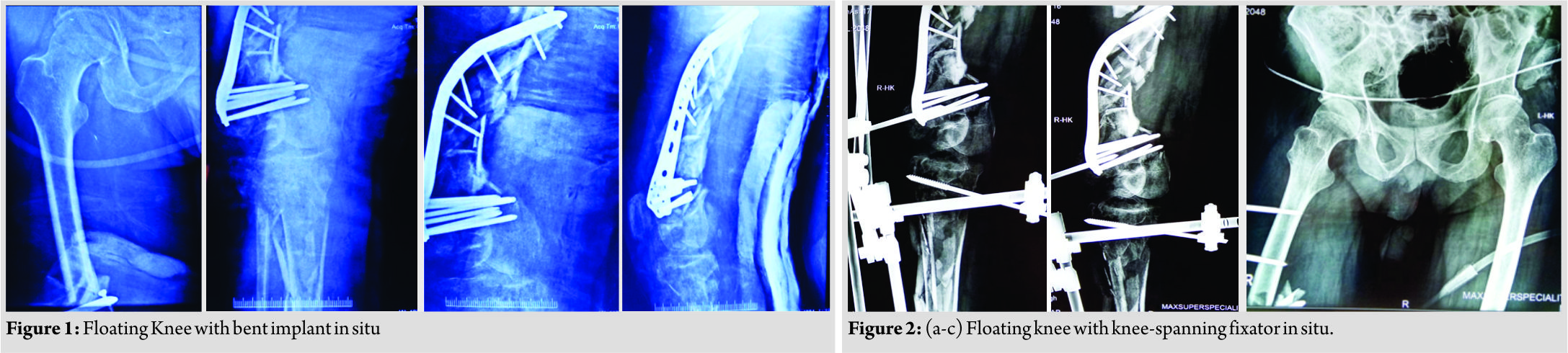 The patient was kept in the ICU till he was fit for subsequent intervention and appropriate treatment in the form of intravenous antibiotics and deep vein thrombosis prophylaxis was given. During this period, the patient had low-grade fever, but his inflammatory markers were normal and the wound over the thigh was healthy. On the 8th day, he was taken up in the operation theater with intubation on. Before removing external fixator, the wound present on anterior aspect of distal thigh was again debrided and found to be clean; then, the decision to proceed further was made and the external fixator was removed. The distal femur was opened through lateral approach using liberal skin incision (Fig. 4).
The patient was kept in the ICU till he was fit for subsequent intervention and appropriate treatment in the form of intravenous antibiotics and deep vein thrombosis prophylaxis was given. During this period, the patient had low-grade fever, but his inflammatory markers were normal and the wound over the thigh was healthy. On the 8th day, he was taken up in the operation theater with intubation on. Before removing external fixator, the wound present on anterior aspect of distal thigh was again debrided and found to be clean; then, the decision to proceed further was made and the external fixator was removed. The distal femur was opened through lateral approach using liberal skin incision (Fig. 4). After splitting the distal part of tensor fasciae latae, the distal locking screws were removed.Since the plate was bent, a bone hook was used to pull out the proximal end of plate laterally. Now, the position of the proximal screws was marked under C-arm control using an artery forceps. Each screw head was cleared causing minimal muscle damage and they were removed in a minimally invasive fashion, thus preserving the biology of zone of comminution and the plate was gently levered out. Following implant removal, we identified that there was another fracture line in coronal plane just posterior to plate application in the articular block which was identified as lateral condyle Hoffa fracture. The articular reconstruction was first done and the Hoffa fracture was fixed using single partially threaded cancellous screw. Manual linear traction was applied to the limb after reconstructing articular block and grossly comminuted fragments were seen to be aligned, so no attempt was made to open the comminuted area. The length of the limb was maintained by giving linear traction and an electrocautery was used to ensure that the center of femoral head, patella, and second toe lie in same line and checked under C-arm to maintain the correct rotation of the limb. The longest available distal femur locking plate (A.O SYNTHES) in the set was slid in a MIPPO fashion bypassing the zone of comminution after reconstructing the articular block. Same incision was extended below knee to expose proximal tibia and the longest available lateral tibia locking plate(A.O SYNTHES) was slid in a MIPPO manner bypassing the comminution. Now, after fixing both the fractures, the knee was examined for ligamentous instability and it was found to be globally unstable in both the planes. Considering the gross comminution in both femur and the tibia, and the being an open fracture, it was decided to wait for ligamentous reconstruction till bony union was achieved. Wound was sutured in layers over negative drain and a long knee brace was given to the patient since the knee was unstable in both the planes.The patient was shifted out of theater in an intubated state. Immediate post-operative X-rays revealed satisfactory alignment of both fractures, (Fig. 5). During the next 7 days, the patient remained intubated and during this period, the passive movement of joints was given, the limb was elevated and the stitch line was carefully monitored. Once the patient was extubated on the 8th day, it was found that there was an associated foot drop which was missed preoperatively since the patient was in an intubated state. The foot drop splint was applied accordingly and physiotherapy in the form of guarded ROM and muscle strengthening exercises was started. We could not ambulate the patient as he had another fracture in the wrist in the recent past, (Fig. 6).
After splitting the distal part of tensor fasciae latae, the distal locking screws were removed.Since the plate was bent, a bone hook was used to pull out the proximal end of plate laterally. Now, the position of the proximal screws was marked under C-arm control using an artery forceps. Each screw head was cleared causing minimal muscle damage and they were removed in a minimally invasive fashion, thus preserving the biology of zone of comminution and the plate was gently levered out. Following implant removal, we identified that there was another fracture line in coronal plane just posterior to plate application in the articular block which was identified as lateral condyle Hoffa fracture. The articular reconstruction was first done and the Hoffa fracture was fixed using single partially threaded cancellous screw. Manual linear traction was applied to the limb after reconstructing articular block and grossly comminuted fragments were seen to be aligned, so no attempt was made to open the comminuted area. The length of the limb was maintained by giving linear traction and an electrocautery was used to ensure that the center of femoral head, patella, and second toe lie in same line and checked under C-arm to maintain the correct rotation of the limb. The longest available distal femur locking plate (A.O SYNTHES) in the set was slid in a MIPPO fashion bypassing the zone of comminution after reconstructing the articular block. Same incision was extended below knee to expose proximal tibia and the longest available lateral tibia locking plate(A.O SYNTHES) was slid in a MIPPO manner bypassing the comminution. Now, after fixing both the fractures, the knee was examined for ligamentous instability and it was found to be globally unstable in both the planes. Considering the gross comminution in both femur and the tibia, and the being an open fracture, it was decided to wait for ligamentous reconstruction till bony union was achieved. Wound was sutured in layers over negative drain and a long knee brace was given to the patient since the knee was unstable in both the planes.The patient was shifted out of theater in an intubated state. Immediate post-operative X-rays revealed satisfactory alignment of both fractures, (Fig. 5). During the next 7 days, the patient remained intubated and during this period, the passive movement of joints was given, the limb was elevated and the stitch line was carefully monitored. Once the patient was extubated on the 8th day, it was found that there was an associated foot drop which was missed preoperatively since the patient was in an intubated state. The foot drop splint was applied accordingly and physiotherapy in the form of guarded ROM and muscle strengthening exercises was started. We could not ambulate the patient as he had another fracture in the wrist in the recent past, (Fig. 6).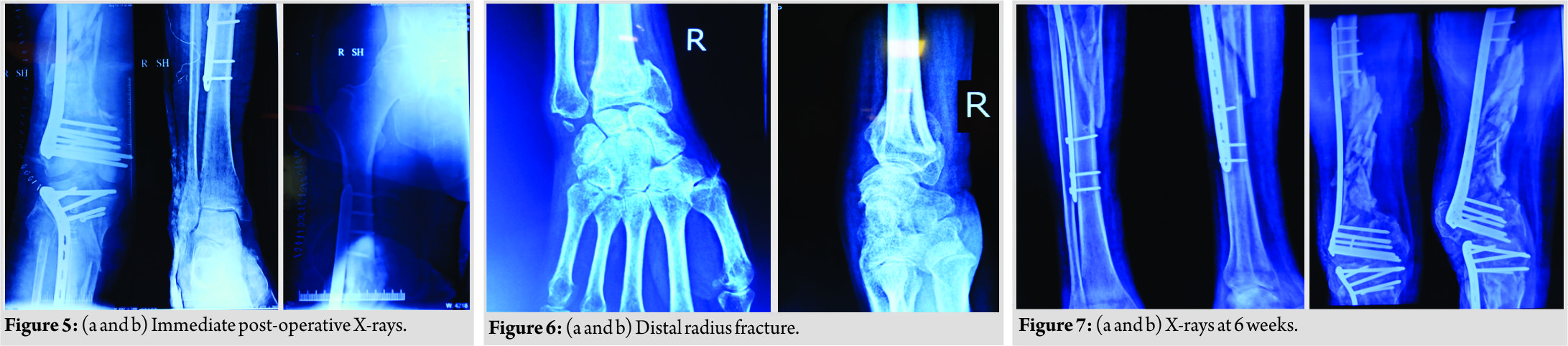 The wound healing was bit delayed but it was ultimately uneventful. An X-ray was taken at 6 weeks post-operative which revealed satisfactory alignment (Fig. 7) and toe touch weight-bearing with long knee brace was started under supervision of trained physiotherapists. The patient was further followed up at 1 month interval and during this rehabilitation period, special attention was given to his psychiatric care. At the latest follow-up of 6 months, the patient had radiological and clinical evidence of union (Fig. 8). At the last available follow-up,the ligamentous instability still persisted, and with long knee brace, he was able to stand and walk. The foot drop was also recovering and there was no extension lag and knee flexion was upto 90° (Fig. 9). At this moment, he was properly counseled and explained in detail about all the available options in the form of arthrodesis, hinged knee arthroplasty, and ligamentous reconstruction, but the patient opted for non-operative management in the form of long knee brace for the time being.
The wound healing was bit delayed but it was ultimately uneventful. An X-ray was taken at 6 weeks post-operative which revealed satisfactory alignment (Fig. 7) and toe touch weight-bearing with long knee brace was started under supervision of trained physiotherapists. The patient was further followed up at 1 month interval and during this rehabilitation period, special attention was given to his psychiatric care. At the latest follow-up of 6 months, the patient had radiological and clinical evidence of union (Fig. 8). At the last available follow-up,the ligamentous instability still persisted, and with long knee brace, he was able to stand and walk. The foot drop was also recovering and there was no extension lag and knee flexion was upto 90° (Fig. 9). At this moment, he was properly counseled and explained in detail about all the available options in the form of arthrodesis, hinged knee arthroplasty, and ligamentous reconstruction, but the patient opted for non-operative management in the form of long knee brace for the time being.
Discussion
Floating knee is the term used when the knee is partially or completely isolated from the rest of the extremity due to the fracture of femur and tibia. These are often associated with injuries to chest, abdomen, or head [1]. Floating knee was first classified by Fraser et al. [4]. Type 1 is the true floating knee in which neither the femoral nor the tibial fracture extends to the knee. Type 2 is a variant in which one or both the fractures involve the knee. Type 2 is further classified according to the knee injury. Type 2 a is a tibial plateau fracture associated with femoral shaft fracture while Type 2b is an articular fracture of distal femur associated with tibial shaft fracture and Type 2c is a fracture of tibial plateau and articular fracture of distal femur [8]. The present case had comminuted fracture of femur involving the articular area with comminuted fracture of proximal tibia with articular involvement. In this classification, there is no mention of any comminution of metadiaphyseal in any of the group so the nearest fracture type under which our fracture can be classified is 2c. The presence of the previous implant had further complicated the injury pattern. In addition, there was associated lateral condyle Hoffa fracture which was missed preoperatively because attention was given to more significant injuries and was seen intraoperatively after removing the previous bent implant. The floating knee is often a part of polytrauma situation and so the patients can be hemodynamically unstable, and therefore, particular attention has to be given to life-threatening injuries and ATLS protocols must be followed [9]. Floating knee is much more than a bony entity alone. Death rate on admission can be as high as 10% [10,11,12]. The present case had been accordingly given care at the index hospital and was kept in the ICU. The first intervention in majority of these patients is in the form of damage control orthopedics. In this approach, minimal intervention is done to stabilize fractures especially of long bones and this minimizes the second hit phenomenon [13]. In our case, damage control was done at the index hospital in the form of knee-spanning external fixator. Popliteal artery lesions can be seen in 7% of cases and it is often an open injury and rate as high as 69% has been reported [8]; compartment syndrome has also been reported [14]. The present case also had an open Grade 2 injury and also had neurological involvement in the form of common peroneal nerve injury which was missed preoperatively since the patient was in an intubated state and was realized only when he was extubated. Paul et al. reported 21 patients with fractures of ipsilateral femur and tibia and found that more than 50% of patients suffered ipsilateral knee injuries [2]. Szalay et al. examined 110 Australian patients with 114 femoral shaft fractures and reported ligament laxity in 27% of patients. In addition, they investigated other 33 patients with 34 ipsilateral femoral and tibial fractures. In this group, 53% of patients had knee ligament laxity, leading to the conclusion that knee ligament injury is more common in the simultaneous femoral and tibial fractures than in the single femoral fractures [15]. Pietu et al. reported that of 172 cases of floating knees, 11% had early diagnosed anterior cruciate ligament ruptures, but 15.7% presented with late severe laxity clearly indicating underestimation of associated ligamentous lesions [8]. The repair of ligament injuries can be delayed till the bony fractures have healed, although it is still a matter of debate among many researchers [15, 16]. The present case also had ligamentous injury which was missed preoperatively since the patient had knee-spanning external fixator in situ and it was diagnosed on table after fixing both femoral as well as tibial fractures. However, considering the gross comminution and open nature of the injury, it was decided to wait for ligamentous reconstruction till solid bony union was achieved. This was given as an option to the patient at follow-up, but he opted for conservative management in the form of long knee brace. The definitive treatment of floating knee involves surgical stabilization of both the fractures. The choice of implant, the sequence of fixation, and the surgical approach depend on numerous factors such as patients general physical condition, associated comorbidities, soft tissue injury, available resources, and last surgical proficiency. Intramedullary nailing appears to be the gold standard for Type 1 injuries which are diaphyseal while in Type 2 injuries, anatomical reconstruction of the joint takes priority and after doing so, metaphyseal-diaphyseal comminution can be stabilized in aminimally invasive fashion using locking plates [17, 18]. Rios et al. studied 43 patients with floating knee injuries and in a subgroup of 25 patients, they performed retrograde femoral nailing and antegrade tibia nailing through single incision and in another subset of 18 patients, they used traditional antegrade femoral nailing and tibia nailing. They concluded that single incision technique is an excellent option for Type 1 floating knee injuries [19]. In another study by Kao et al. [20], femoral fractures around trochanteric area were fixed using various implants in the form of cannulated screws, dynamic hipscrews, and dynamic compression screws, whereas femoral shaft fractures were fixed using intramedullary nailing either in supine position or using traction table.Tibial fractures around tibial plateau, proximal tibia, or distal tibia were fixed using compression plates or interlocking nailing depending on the fracture location. Theodratus et al. recommended intramedullary nailing as the best treatment choice except for Grade 3b and 3c open fractures [21]. The evidence for the indications and special technical considerations of the plating in floating knee injuries is sparse. Ran et al. [22] reported on outcome and management of 28 patients with floating knee injuries. In 14 cases, simultaneous plating of distal femur and proximal tibia was done. The results of plating of both fractures were excellent in 1, good in 7, acceptable in 3, and poor in 3 according to the Karlstrom and Olerud classification. In our case, considering the intra-articular nature of both distal femur and proximal tibia fractures along with the extensive metadiaphyseal comminution, the only suitable option available was plating of both the fractures. In addition, removal of the previous implant was a challenge. Hence, careful retrieval of plate and screws without disturbing the biology of smaller fragments was essential and with that due care, another implant was put. Maintaining the length and rotation of the limb were another issue. The length was maintained by manual linear traction and it was ensured that center of femoral head, patella, and second toe lie in same line by keeping electrocautery and checked under C-arm. We believe that the mechanism of injury in our case was axial force transmission along flexed knee which led to high-energy impact on the knee, leading to such a devastating injury. The presence of previous screws into anterior part of femoral condyle could be the reason for associated Hoffa fracture as shown in Fig. 2. Our case report represents an atypical case of floating knee injury and had Hoffa fracture of lateral femoral condyle along with neurological and ligamentous injury, both of which were missed preoperatively. Summarizing, the floating knee injuries are devastating injuries which produce varied results as the incidence of both systemic and local complications is high. Systemic complications could be fat embolism, renal failure, or chest or head injuries, while local complications could be pain, non-union, delayed union, infection, osteomyelitis, or in extreme conditions need to amputate the limb. Even after extensively searching the available literature, we could not find any reference of Hoffa’s fracture associated with floating knee in a previously present implant, and to the best of our knowledge, our case report is the first one to describe such an unusual pattern of injury.
Conclusion
Floating knees are a morbid group of injuries that demand careful and meticulous planning taking into account various factors such as patients general condition, associated injuries, soft tissue status, and fracture pattern to achieve the best possible outcome.
Clinical Message
Complex floating knee in the presence of a previous implant creates an unusual fracture pattern which is a rare entity and poses a unique challenge in management and subsequent rehabilitation. The choice of implant, the sequence of fixation, and the surgical approach depend on numerous factors such as patients general physical condition, associated comorbidities, soft tissue injury, available resources, and last surgical proficiency.
References
1. Rethnam U, Yesupalan RS, Nair R. The floating knee: Epidemiology, prognostic indicators and; outcome following surgical management. J Trauma Manag Outcomes 2007;1:2.
2. Paul GR, Sawka MW, Whitelaw GP. Fractures of the ipsilateral femur and tibia: Emphasis on intra-articular and soft tissue injury. J Orthop Trauma 1990;4:309-14.
3. Kumar R. The floating knee injury. J Clin Orthop Trauma 2011;2:69-76.
4. Fraser RD, Hunter GA, Waddell JP. Ipsilateral fracture of the femur and tibia. J Bone Joint Surg Br 1978;60-B:510-5.
5. Heuschen UA, Göhring U, Meeder PJ. Bilateral hoffa fracturea rarity. Aktuelle Traumatol 1994;24:83-6.
6. Lewis SL, Pozo JL, Muirhead-Allwood WF. Coronal fractures of the lateral femoral condyle. J Bone Joint Surg Br 1989;71:118-20.
7. D’Alleyrand JC, O’Toole RV. The evolution of damage control orthopedics: Current evidence and practical applications of early appropriate care. Orthop Clin North Am 2013;44:499-507.
8. Piétu G, Jacquot F, Féron JM, et les membres du GETRAUM. The floating knee: A retrospective analysis of 172 cases. Rev Chir Orthop Reparatrice Appar Mot 2007;93:627-34.
9. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: Retrospective and prospective analyses. J Bone Joint Surg Am 1976;58:453-8.
10. Dwyer AJ, Paul R, Mam MK, Kumar A, Gosselin RA. Floating knee injuries: Long-term results of four treatment methods. Int Orthop 2005;29:314-8.
11. Anastopoulos G, Assimakopoulos A, Exarchou E, Pantazopoulos T. Ipsilateral fractures of the femur and tibia. Injury 1992;23:439-41.
12. Gregory P, DiCicco J, Karpik K, DiPasquale T, Herscovici D, Sanders R, et al. Ipsilateral fractures of the femur and tibia: Treatment with retrograde femoral nailing and unreamed tibial nailing. J Orthop Trauma 1996;10:309-16.
13. Lichte P, Kobbe P, Dombroski D, Pape HC. Damage control orthopedics: Current evidence. Curr Opin Crit Care 2012;18:647-50.
14. Adamson GJ, Wiss DA, Lowery GL, Peters CL. Type II floating knee: Ipsilateral femoral and tibial fractures with intraarticular extension into the knee joint. J Orthop Trauma 1992;6:333-9.
15. Szalay MJ, Hosking OR, Annear P. Injury of knee ligament associated with ipsilateral femoral shaft fractures and with ipsilateral femoral and tibial shaft fractures. Injury 1990;21:398-400.
16. Walling AK, Seradge H, Spiegel PG. Injuries to the knee ligaments with fractures of the femur. J Bone Joint Surg Am 1982;64:1324-7.
17. Hung SH, Chen TB, Cheng YM, Cheng NJ, Lin SY. Concomitant fractures of the ipsilateral femur and tibia with intra-articular extension into the knee joint. J Trauma 2000;48:547-51.
18. Jain A, Aggarwal P, Pankaj A. Concomitant ipsilateral proximal tibia and femoral hoffa fractures. Acta Orthop Traumatol Turc 2014;48:383-7.
19. Ríos JA, Ho-Fung V, Ramírez N, Hernández RA. Floating knee injuries treated with single-incision technique versus traditional antegrade femur fixation: A comparative study. Am J Orthop (Belle Mead NJ) 2004;33:468-72.
20. Kao FC, Tu YK, Hsu KY, Su JY, Yen CY, Chou MC, et al. Floating knee injuries: A high complication rate. Orthopedics 2010;33:14.
21. Theodoratos G, Papanikolaou A, Apergis E, Maris J. Simultaneous ipsilateral diaphyseal fractures of the femur and tibia: Treatment and complications. Injury 2001;32:313-5.
22. Ran T, Hua X, Zhenyu Z, Yue L, Youhua W, Yi C, et al. Floating knee: A modified Fraser’s classification and the results of a series of 28 cases. Injury 2013;44:1033-42.
 |
 |
 |
 |
| Dr. Gaurav Saini | Dr. R K Sen | Dr. Anoop Kalia | Dr. Sagar Kadam |
| How to Cite This Article: Saini G, Sen R K, Kalia A, Kadam S. Implant-associated Hoffa’s Fracture in a Floating Knee: A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2019 May-June; 9(3): 79-83. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


