
[box type=”bio”] Learning Point of the Article: [/box]
The pain and paresthesia of medial foot can be caused by a ganglion cyst of the tibial nerve and the ultrasound examination is usefull tool to visualize this pathology.
Case Report | Volume 9 | Issue 4 | JOCR July-August 2019 | Page 76-79 | Barbara Igielska-Bela, Marek Krzemiński, Ludomira Rzepecka-Wejs. DOI: 10.13107/jocr.2019.v09i04.1488
Authors: Barbara Igielska-Bela[1], Marek Krzemiński[1], Ludomira Rzepecka-Wejs[2]
[1]Department of Orthopedic, Specialist Hospital in Koscierzyna, Ul.Piechowskiego 36, 83-400 Kościerzyna,
[2]Goris-Med Sp. p., Sopot, Poland.
Address of Correspondence:
Dr. Barbara Igielska-Bela,
Department of Orthopaedic, Specialist Hospital in Koscierzyna, Ul. Piechowskiego 36, 83-400 Kościerzyna.
E-mail: 33030@gumed.edu.pl
Abstract
Introduction: The intraneural ganglion cyst of the tibial nerve is very rare, especially at the level of an ankle and a foot. There are 15 previous reports of the tibial intraneural ganglion cyst within the tarsal tunnel or the popliteal fossa. The authors present an infrequent case of the tibial intraneural ganglion at the level of the tarsal tunnel diagnosed by an ultrasound examination and provide a review of the case studies described earlier in the available literature.
Case Report: Patient, a 37-year-old Caucasian male, was admitted to the orthopedic outpatient clinic with the pain and the paresthesia of medial half of his right foot. He underwent an ultrasound examination which diagnosed the intraneural ganglion cyst of the tibial nerve. The patient was qualified for surgical treatment. The nerve was compressed to only 30% of its diameter. The nerve function returned in4 months post-operative and the patient presented no signs of the nerve disorder.
Conclusion: In almost all analyzed articles, authors suggest that pathogenesis is connected with the retrograde extension of the synovial fluid from the adjacent joints or with the trauma. In our study, there was no history of trauma and there was no connection with the joint during operation. We believed that the pathogenesis of this disorder was multifactorial.
Keywords: Intraneural ganglion cyst, tibial nerve, ultrasound
Introduction
The intraneural ganglion cyst of the peripheral nerves is rare defect which is caused by the accumulation of thick mucous fluid inside the epineurium [1, 2]. These cysts are usually found in adults and cause an intermittent compression of nerve fascicles, resulting in pain, paresthesia, weakness, muscle denervation, or even atrophy. The etiology of such cysts seems to be secondary to chronic mechanical irritation or idiopathic mucoid degeneration. Some authors believe that the cysts are the retrograde extensions of synovial fluid along the path of the intra-articular branches of a surrounding nerve [2, 3]. An intraneural hemorrhage secondary to trauma and formation of cysts after resorption of the hemorrhage has also been proposed. Several reports also described trauma as a potential pathology [1, 2, 3, 4, 5]. An ultrasound examination is a good diagnostic tool to confirm problems with peripheral nerves. This examination may give information which includes the enlargement of the diameter and the cross-sectional area of the nerve trunk, the presence of pathological structures and, in cases of the nerve compression, the hour glass narrowing on the longitudinal section; abundle echostructure disorder and hyperemia above the site of compression [6]. The authors present a rare case of an isolated extra-articular intraneural cyst of the tibial nerve and a medial plantar nerve with the illustration of the sonography appearances and intraoperative findings.
Case Report
A 37-year-old Caucasian male was admitted to the orthopedic outpatient clinic with the pain and paresthesia of the medial half of his right foot. The general history of the patient did not reveal any systematic diseases. He did not give any history of injury of his foot and ankle in the past. The patient’s only symptom was aching at the medial aspect of his foot. This pain was aggravated during work. The symptoms started 2 months before the orthopedic consultation. The range of motion was normal.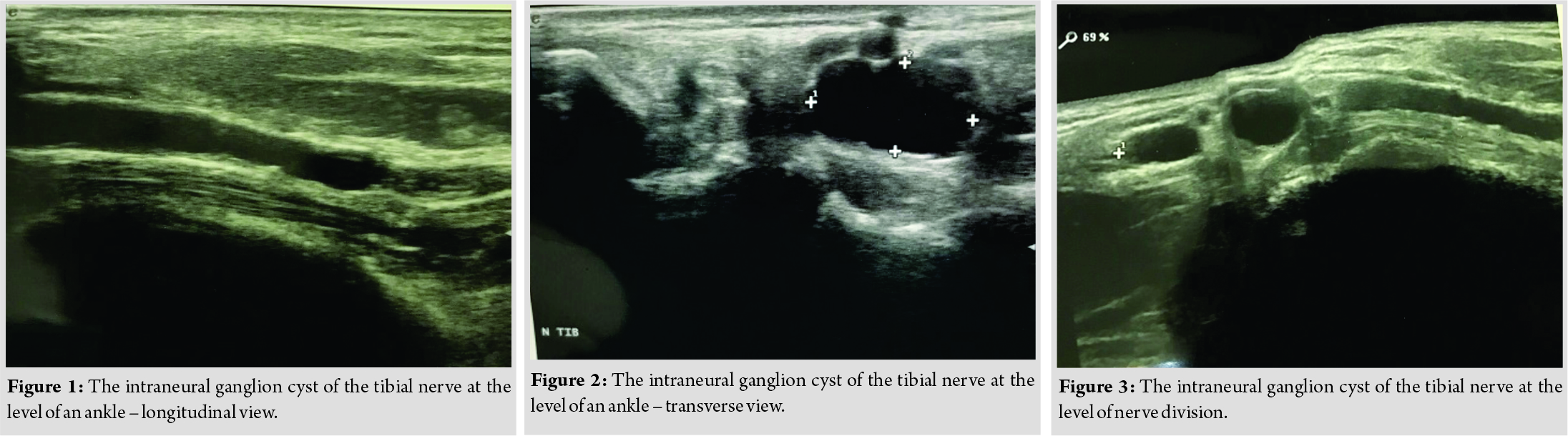
An X-ray of the foot showed no abnormalities. On an ultrasound examination of the foot, the longitudinal and transverse views were taken using a linear 14MHz probe, Esaote My lab Class C. The patient was kept in the horizontal (lying) position. The ultrasound examination showed that the patient had an intraneural ganglion cyst of the tibial nerve at the level of an ankle and the nerve division to the medial and lateral plantar nerves (Fig. 1, 2and 3).The nerve conduction study suggested a slower conduction of the tibial nerve.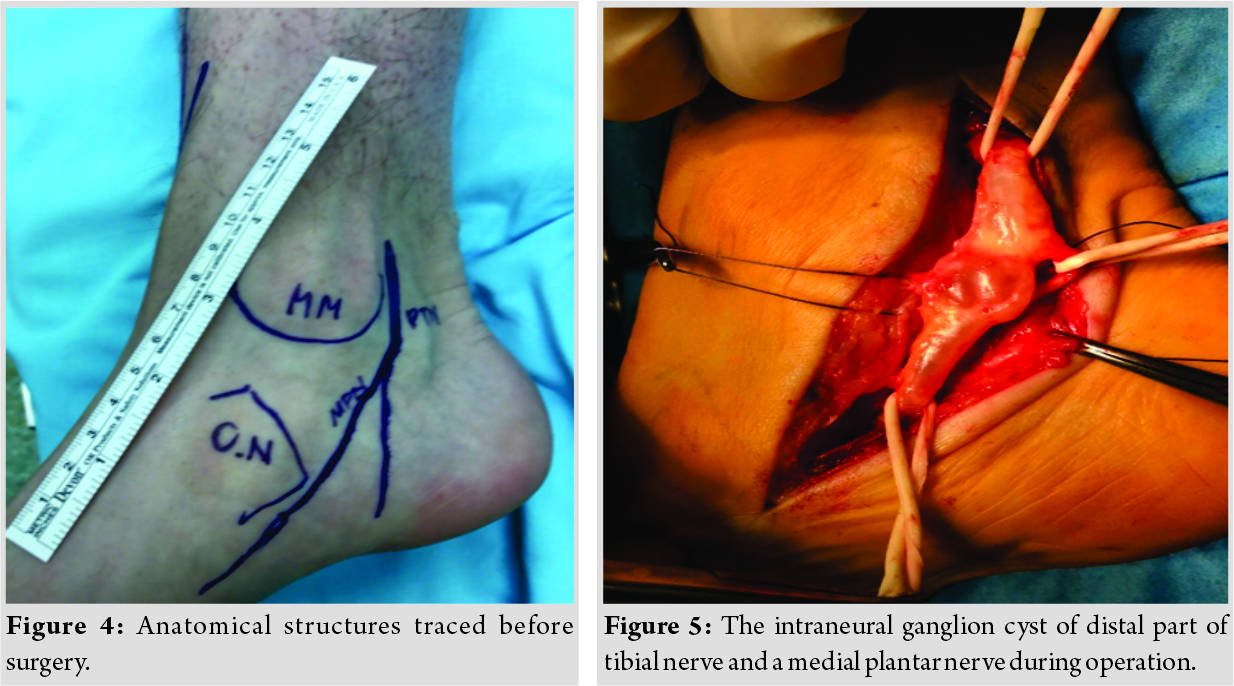
The patient was offered a choice of surgical treatment. The surgery took place 5 months after the first symptoms. The anatomical structures were traced before surgery (Fig. 4). During the operation, the intraneural ganglion cyst of the distal part of the tibial nerve and a medial plantar nerve was found (Fig. 5). In the widest place, the nerve reached the diameter of 2 cm. After cutting the epineurium, about 2–3 cm 3 of thick mucous fluid was evacuated (Fig. 6). The nerve was compressed to only 30% of its diameter. The fibrosis was removed, leaving the nerve fibers intact (Fig. 7).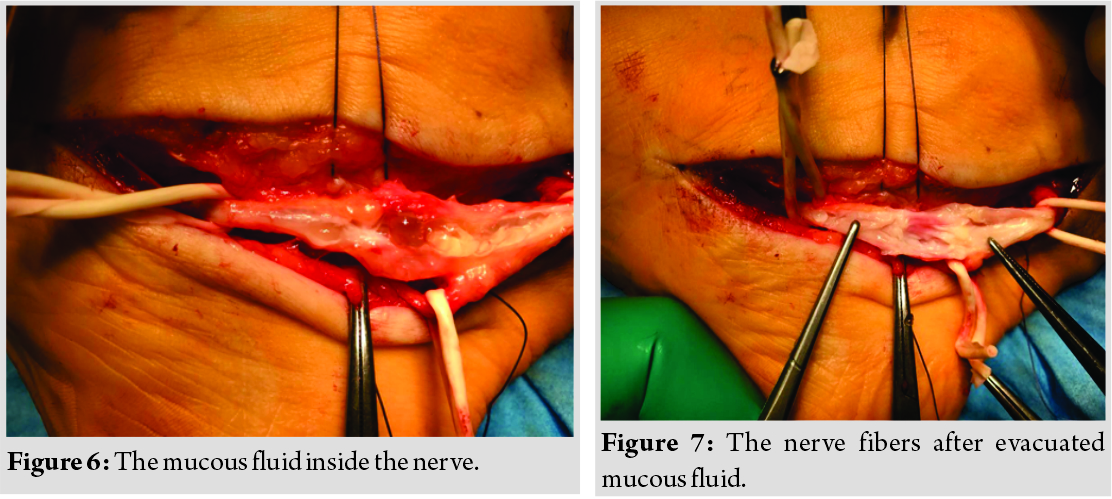
The nerve function had returned in 4 months post-operative and the patient presented no signs of the nerve disorder. The normal structure of the nerve was presented in an ultrasound examination performed in 4 months postoperatively.
Discussion
The peripheral nerves may contain some various combinations of motor and sensory fibers. The sensory manifestations of neuropathy include hypoesthesia, hypoalgesia, paresthesia, hyperalgesia, and a prickling or tingling sensation. The symptoms of motor neuropathy usually include muscle spasms, clonus, fasciculations, amyotrophy, and the loss of muscle strength[1, 2]. The first case of an intraneural ganglion cyst of the tibial nerve was described in 1967 [3, 4]. In 1975, Jacobs et al. described two cases of an intraneural ganglion cyst: One of the sciatic nerves and one of the tibial nerves in the tarsal tunnel. Their examinations suggest that the lesion develops by a multicentric metaplasia of the connective tissue elements of the nerve rather than by an invasion [5]. In 1985, Godin et al., and in 2000, Spinner et al. documented the cases of a tibial intraneural ganglion, yet at the level of the knee. They suggested that a connection with the joint can participate in the development of this disorder [7, 8, 9]. The case report of the tibial intraneural ganglion was presented in 2006 by And et al. The authors conclude that the trauma might be a contributing factor to the development of intraneural ganglion cysts [10]. The consideration regarding intraneural cysts connected with the joint was taken into by Spinner et al. Their review of the same cases demonstrated radiographic evidence of the joint communications with the subtalar joints. They believed that tibial intraneural ganglia within the tarsal tunnel originate from the neighboring joints and that their connections to the joints (pedicles) are through articular branches[11]. Blitz et al. described the case report of a sural intraneural ganglion cyst. In their study, they made a retrospective reinterpretation of the patient’s pre-operative and post-operative magnetic resonance imaging (MRI) which revealed that the ligation of the articular trunk, proximal to a major branch (i.e., the anterior branch of the lateral calcaneal nerve) led to an increased intraneural cyst propagation distally. They concluded that their case report provides evidence supporting the articular theory of intraneural ganglion formation [12]. The next confirmation of the articular theory of intraneural ganglion cysts was made in 2011 by Davis and Cox; they presented two cases of tibial intraneural ganglion cyst. During the MRI, they found cysts connection to the adjacent joint through the articular branch of the nerves. This articular branch was also found at the surgery and resected [13].
Conclusion
In almost all analyzed articles, the authors suggest that the pathogenesis is connected to a retrograde extension of the synovial fluid from the adjacent joints or with the trauma. The authors suggest to use ultrasound examination or the MRI to diagnose these disorders. Our patient also had an ultrasound examination of his foot performed, which confirmed the diagnosis. In our study, there was no history of any trauma and there was no connection with a joint during the operation. We believe that the pathogenesis of this disorder is multifactorial.
Clinical Message
The pain of the medial aspect of the foot can be caused by intraneural ganglion cyst of the tibial nerve. Ultrasound examination can help put early right diagnosis. To avoid the tibial nerve damage, surgery is indicated. It is also important to remember that the pathogenesis of this disorder is multifactorial.
References
1. Silveira CR, Vieira CG, Pereira BM, Pinto Neto LH, Chhabra A. Cystic degeneration of the tibial nerve: Magnetic resonance neurography and sonography appearances of an intraneural ganglion cyst. Skeletal Radiol2017;46:1763-7.
2. Isaacs AM, Midha R, Desy NM, Amrami KK, Spinner RJ. The mechanism underlying combined medial and lateral plantar and tibial intraneural ganglia in the tarsal tunnel. Acta Neurochir (Wien) 2016;158:2225-9.
3. Prasad NK, Desy NM, Howe BM, Amrami KK, Spinner RJ. Subparaneurial ganglion cysts of the fibular and tibial nerves: A new variant of intraneural ganglion cysts. Clin Anat2016;29:530-7.
4. Friedlander HL. Intraneural ganglion of the tibial nerve. A case report. J Bone Joint Surg Am 1967;49:519-22.
5. Jacobs R, Maxwell JA, Kepes J. Ganglia of the nerve. Presentation of two unusual cases, a review of the literature, and a discussion of pathogenesis. Clin OrthopRelat Res1975;113:135-44.
6. Godin V, Huaux JP, Knoops P, Noel H, Rombouts JJ: Une cause rare de paralysie des muscles releveurs du pied; le kyste synovial intraneural du SPE. Louv Med 1985;104:281-6.
7. Kowalska B, Sudoł-Szopińska I. Ultrasound assessment of selected peripheral nerve pathologies. Part II: Lower limb compression neuropathy.J Ultrasound 2012;12:463-71.
8. Godin V, Huaux JP, Knoops P. A rare case of anterior tibial nerve palsy: The intra neural ganglion of the lateral popliteal nerve. Neurochirurgie1987;33:412-3.
9. Spinner RJ, Atkinson JL, Harper CM Jr., Wenger DE. Recurrent intraneural ganglion cyst of the tibial nerve. Case report. J Neurosurg2000;92:334-7.
10. Adn M, Hamlat A, Morandi X, Guegan Y. Intraneural ganglion cyst of the tibial nerve. Acta Neurochir (Wien) 2006;148:885-9.
11. Spinner RJ, Dellon AL, Rosson GD, Anderson SR, Amrami KK. Tibial intraneural ganglia in the tarsal tunnel: Is there a joint connection? J Foot Ankle Surg 2007;46:27-31.
12. Blitz NM, Prestridge J, Amrami KK, Spinner RJ. A posttraumatic, joint-connected sural intraneural ganglion cyst-with a new mechanism of intraneural recurrence: A case report. J Foot Ankle Surg 2008;47:199-205.
13. Davis GA, Cox IH. Tibial intraneural ganglia at the ankle and knee: Incorporating the unified (articular) theory in adults and children. J Neurosurg2011;114:236-9.
 |
 |
 |
| Dr. Barbara Igielska-Bela | Dr. Marek Krzemiński | Dr. Ludomira Rzepecka-Wejs |
| How to Cite This Article: Igielska-Bela B, Krzemiński M, Rzepecka-Wejs L. The Intraneural Ganglion Cyst of the Tibial Nerve: A Case Report and Review of Literature. Journal of Orthopaedic Case Reports 2019 Jul-Aug; 9(4): 76-79. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


