
[box type=”bio”] Learning Point of the Article: [/box]
Aneurysmal bone cyst of the clavicle though rare can occur and also be treated successfully with surgery.
Case Report | Volume 9 | Issue 6 | JOCR November – December 2019 | Page 3-5 | Asish Rajak, Amit Sethia, Amit Limbu, Rosan P S Kalawar. DOI: 10.13107/jocr.2019.v09.i06.1562
Authors: Asish Rajak[1], Amit Sethia[1], Amit Limbu[1], Rosan P S Kalawar[1]
[1]Department of Orthopaedics, B.P. Koirala Institute of Health Sciences, Dharan, Nepal.
Address of Correspondence:
Dr. Asish Rajak,
Department of Orthopaedics, B.P. Koirala Institute of Health Sciences,Dharan, Nepal.
E-mail: asishrjk@gmail.com
Abstract
Introduction: Aneurysmal bone cyst is a rare benign solitary tumor of the long tubular bones, pelvis, and vertebrae which rarely affects the clavicle. It is common in the adolescent age group and rare in old age. The characteristic radiological suggests and histopathological picture confirms its diagnosis. This case is of interest because there are only a few cases of aneurysmal bone cyst of the clavicle reported to date.
Case Report: An 11-year-old boy presented with a history of pain in the right clavicular area for 3 months associated with swelling which gradually increased in size. The radiograph showed an expansile bony mass at the lateral fourth of the right clavicle with internal septations with thinning of the cortex and no evidence of periosteal reaction. The affected part of the lateral part of the clavicle was resected leaving the thick periosteum intact. Histologically, section revealed solid and cystic areas. The cysts were separated by septa and filled with hemorrhage and beneath the surface showed osteoid bone formation and multinucleated giant cells. Stroma showed loosely arranged spindle cells which had vesicular nuclei, inconspicuous to prominent nucleoli, and moderate amount of eosinophilic cytoplasm. Prominent blood vessel proliferation was evident. Pleomorphism and mitotic figures were not seen in the specimen. The overall histological picture was that of an aneurysmal bone cyst.
Conclusion: Aneurysmal bone cyst occurring in this age group is not so common in the clavicle. This is a rare case which requires mention in literature. Our case was treated by marginal resection. On regular follow-up,the regeneration of the bone within the intact periosteum can be seen.
Keywords: Aneurysmal bone cyst, clavicle, tumor.
Introduction
Aneurysmal bone cyst is a rare [1] benign solitary tumor of the long tubular bones, pelvis, and vertebrae which rarely affects the clavicle[2]. It is common in the adolescent age group [3] and rare in old age. The characteristic radiological [3] suggests and histopathological picture [4] confirms its diagnosis. This case is of interest because there are only a few cases of aneurysmal bone cyst of the clavicle reported to date [5, 6, 7].
Case Report
An 11-year-old boy presented with a history of pain in the right clavicular area for 3 months. The pain was acute in onset associated with swelling which gradually increased in size. There was no history of recent trauma, no history of loss of weight. On local examination, there was a localized swelling over the right clavicular area which was tender. There were no skin changes — no neurovascular deficits on the ipsilateral upper limb.
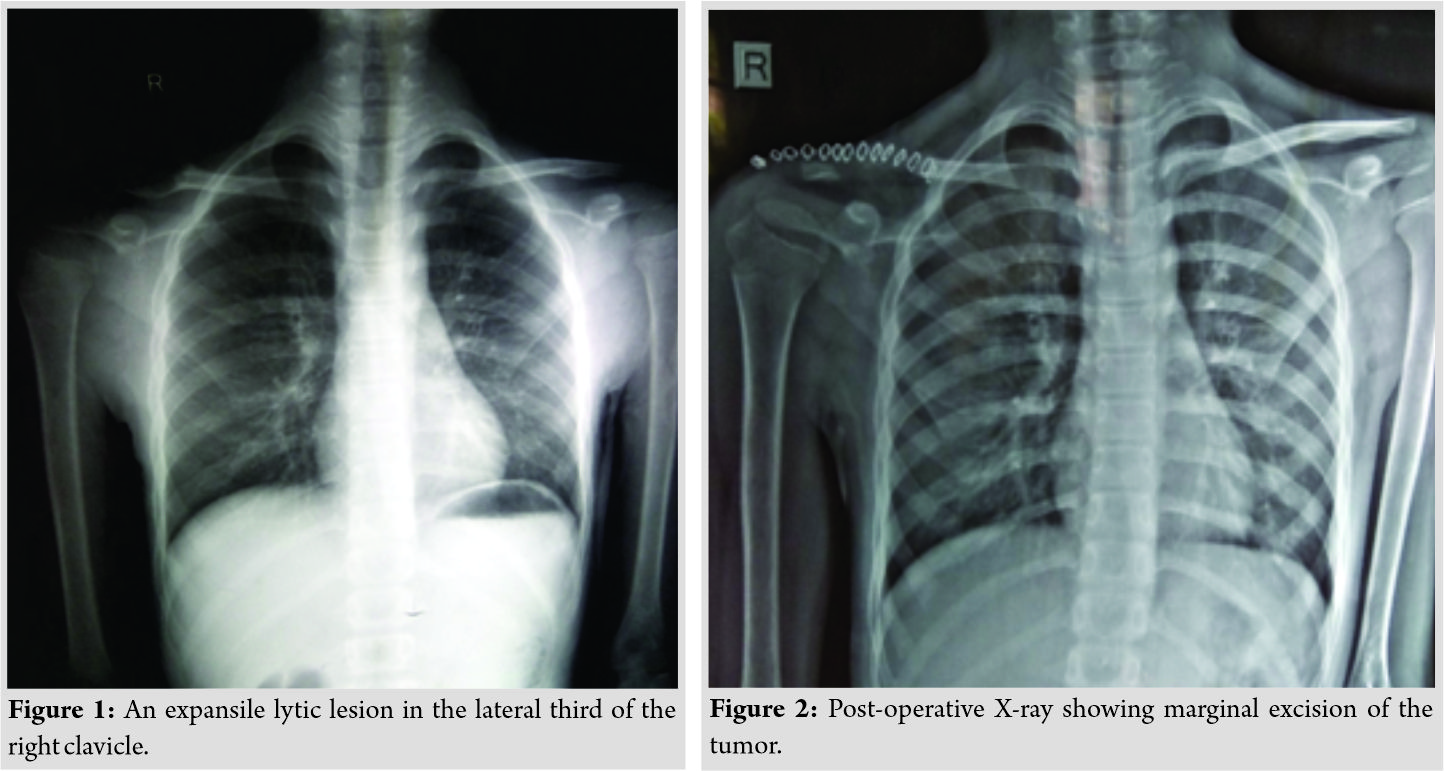
Radiograph at the time showed an expansile bony mass at the lateral fourth of the right clavicle with internal septations with thinning of the cortex and no evidence of periosteal reaction (Fig. 1).
The affected part of the lateral part of the clavicle was resected leaving the thick periosteum intact (Fig. 2). The surgical specimen measuring 4 × 2 × 1 cm showed a multiloculated cyst of about 1.7 cm along with solid areas measuring 1.5 cm. The cyst wall showed focal blackish areas. Histologically, section revealed solid and cystic areas. The cysts were separated by septa and filled with hemorrhage and beneath the surface showed osteoid bone formation and multinucleated giant cells. Stroma showed loosely arranged spindle cells which had vesicular nuclei, inconspicuous to prominent nucleoli, and moderate amount of eosinophilic cytoplasm. Prominent blood vessel proliferation was evident. Pleomorphism and mitotic figures were not seen in the specimen. The overall histological picture was that of an aneurysmal bone cyst.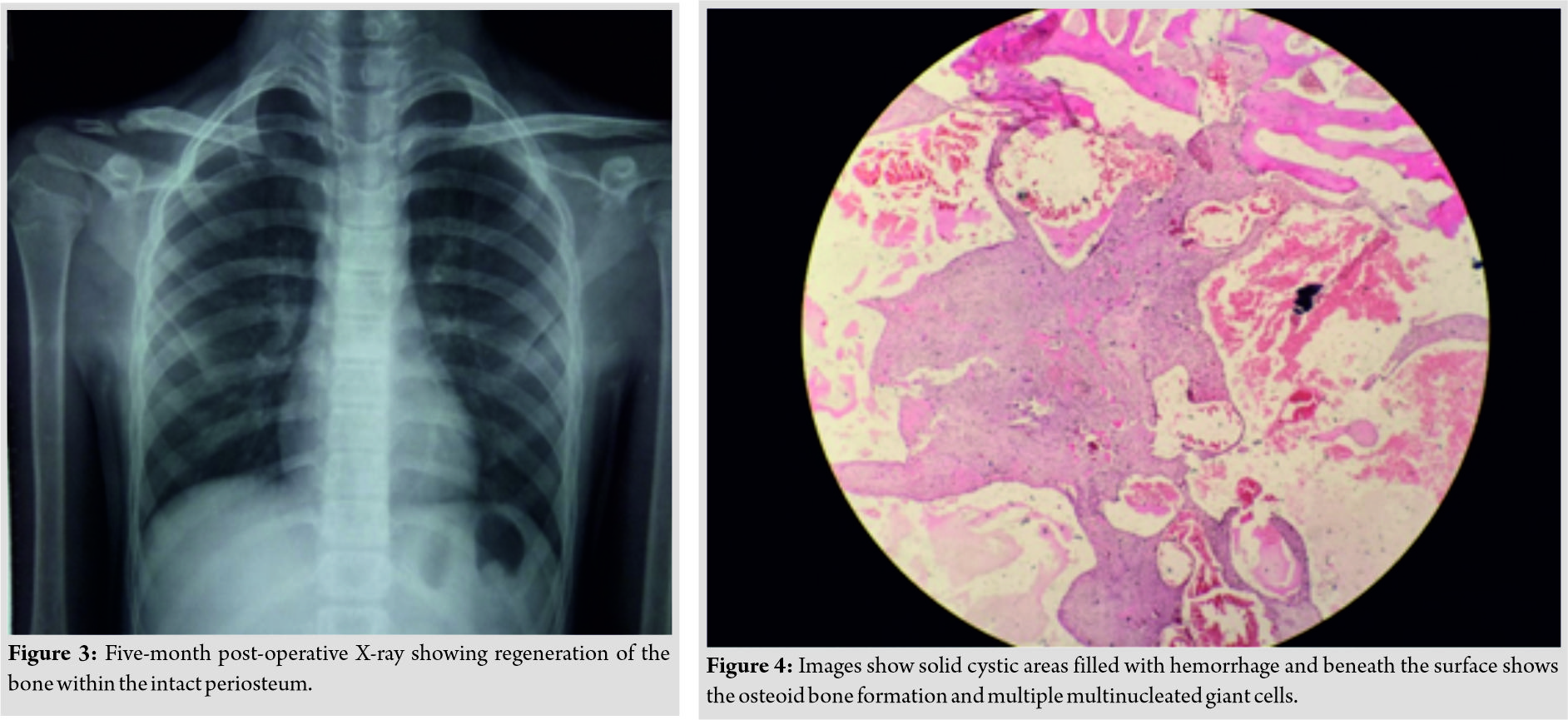
Discussion
The term aneurysmal bone cyst was first given by Jaffe and Lichtenstein while describing its radiological features in 1942 [8]. Aneurysmal bone cyst occurring in this age group is common but not so much in the clavicle [2]. Rarer are the occurrences of this tumor in the rib, skull, and mandible. The occurrence of the lesion seems to be rarer in the medial third which has been reported [9]. Aneurysmal bone cyst can also be found in association with other lesions such as giant cell tumor, chondroblastoma, osteoblastoma, fibrous dysplasia, nonossifying fibroma, and chondromyxoid fibroma [10, 11, 12]. Patients usually present with pain, swelling around the lesion, and sometimes coinciding history of trauma. These tumors can be treated by extended curettage, marginal resection, arterial embolization, and rarely low dose radiation [10]. Furthermore, cases have been treated with bisphosphonates in areas where it is unresectable or for recurrences [13, 14]. Our case was treated by marginal resection. On regular follow-up,the regeneration of the bone within the intact periosteum can be seen (Fig. 3).
There is also a chance of recurrence in our case which is overall 10–20% and more so in the age group which in literature is considered to be due to insufficient curettage [4, 12].
Conclusion
Aneurysmal bone cyst occurring in this age group in the clavicle is a rare presentation which requires mention in literature. Our case was treated by marginal resection. On regular follow-up,the regeneration of the bone within the intact periosteum can be seen (Fig. 4).
Clinical Message
Aneurysmal bone cyst of the clavicle though rare should be a consideration in tumors of the clavicle. It is a challenging diagnosisand since it is a curable tumor with minimal recurrence, our aim should be curative.
References
1. Boubbou M, Atarraf K, Chater L, Afifi A, Tizniti S. Aneurysmal bone cyst primaryabout eight pediatric cases: Radiological aspects and review of the literature. Pan Afr Med J 2013;15:111.
2. Smith J. Aneurysmal bone cyst of clavicle. Indian J Surg Oncol 2014;5:158-60.
3. Sherman RS, Soong KY. Aneurysmal bone cyst: Its roentgen diagnosis. Radiology 1957;68:54-64.
4. Ruiter DJ, van Rijssel TG, van der Velde EA. Aneurysmal bone cysts: A clinicopathological study of 105 cases. Cancer 1977;39:2231-9.
5. Pointu J, Kehr P, Sejourné P, Mathevon H, Destrée G, Lang G, et al. Aneurysmal cyst of the clavicle : An uncommon lesion and a difficult diagnosis (author’s transl). Sem Hop 1982;58:1141-3.
6. Yashavntha KC, Nalini KB, Menon J, Patro DK. Aneurysmal bone cyst of medial end of clavicle in a child, a rare case report. Indian J Surg Oncol 2014;5:158-60.
7. Bakkaly AE, Hanine MD, Amrani A, Dendane A, El Alami SZ, Madhi TE, et al. Aneurysmal bone cyst of the clavicle: About a case. Pan Afr Med J 2017;27:115.
8. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst: With emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg 1942;44:1004-25.
9. Parashari UC, Khanduri S, Upadhyay D, Bhadury S, Singhal S. Radiologic and pathologic correlation of aneurysmal bone cysts at unusual sites. J Cancer Res Ther2012;8:103-5.
10. Canale ST, Beaty JH. Campbell’s Operative Orthopaedics.Philadelphia, PA: Elsevier Health Sciences; 2012.
11. Martinez V, Sissons HA. Aneurysmal bone cyst. A review of 123 cases including primary lesions and those secondary to other bone pathology. Cancer 1988;61:2291-304.
12. Sasaki H, Nagano S, Shimada H, Yokouchi M, Setoguchi T, Ishidou Y, et al. Diagnosing and discriminating between primary and secondary aneurysmal bone cysts. Oncol Lett 2017;13:2290-6.
13. Sivendran S, Harvey H, Lipton A, Drabick J. Treatment of langerhans cell histiocytosis bone lesions with zoledronic acid: A case series. Int J Hematol2011;93:782-6.
14. Cornelis F, Truchetet ME, Amoretti N, Verdier D, Fournier C, Pillet O, et al. Bisphosphonate therapy for unresectable symptomatic benign bone tumors: A long-term prospective study of tolerance and efficacy. Bone 2014;58:11-6.
 |
 |
 |
 |
| Dr. Asish Rajak | Dr. Amit Sethia | Dr. Amit Limbu | Dr. Rosan P S Kalawar |
| How to Cite This Article: Rajak A, Sethia A, Limbu A, Kalawar R P S. Aneurysmal Bone Cyst of the Clavicle: A Case Report. Journal of Orthopaedic Case Reports 2019 Nov-Dec;9(6): 3-5. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


