
[box type=”bio”] Learning Point of the Article: [/box]
Nontraumatic pain in clavicle bone should be thinking in neoplastic origin.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 54-57 | David Gómez Garrido, Alfonso Prada Cañizares, Michele Bisaccia, Luigi Meccariello, Estefania Fernández Delgado. DOI: 10.13107/jocr.2020.v10.i02.1694
Authors: David Gómez Garrido[1], Alfonso Prada Cañizares[2], Michele Bisaccia[3], Luigi Meccariello[4], Estefania Fernández Delgado[5]
[1]Department of Orthopedics and Traumatology, Hospital Quiron Salud Toledo,Hospital Solimat Toledo, Spain
[2]Department of Orthopedics and Traumatology, Hospital General de Villalba, Spain,
[3]Department of Orthopedics and Traumatology, Azienda Ospedaliera “S. Maria Della Misericordia” Perugia, Italy,
[4]Department of Orthopedics and Traumatology, Vito Fazzi Hospital, Lecce, Italy,
[5]Department of Radiology, Hospital General de Villalba, Spain.
Address of Correspondence:
Dr. Luigi Meccariello,
Department of Orthopedics and Traumatology, Vito Fazzi Hospital, Via Ada Cudazzo, Block: A- Floor:V, Lecce, Italy.
E-mail: drlordmec@gmail.com
Abstract
Introduction: Pain around the shoulder is very common. The most frequent causes of shoulder pain without traumatic even are rotator cuff diseases, shoulder, and sternoclavicular arthritis, other causes are neoplastic pathology, but lung cancer metastasis has never been described.
Case Report: We describe a rare case of pathological clavicle fracture as the cause of atraumatic shoulder pain, as the first case of lung cancer, and discuss the different cause of shoulder pain.
Conclusion: Pathological clavicular fracture is a very rare disease and symptom of lung cancer but should be in the differential diagnosis in patients with focal pain without traumatic event and abnormal radiographic studies.
Keywords: Clavicle, lung, cancer, metastatic, fracture.
Introduction
Shoulder problems are common in patients around 40 years of age. Shoulder pain is a frequent reason for a medical visit; some studies have reported up to address that 30% of medical consultations to a general practitioner to be due to shoulder pain. The shoulder is a complex joint with numerous anatomical structures which can be damaged and be a source of pain. Rotator cuff disease is the most common cause for this condition in patients older than 50 years of age, and a non-traumatic fracture of the clavicle is a very rare etiology. Non-neoplastic conditions such as ¨osteitis condensing claviculii¨ sternoclavicular joint arthropathy, chronic sternoclavicular dislocation, osteoporotic fracture, chronic recurrent multifocal osteomyelitis (CRMO), or acromioclavicular osteoarthritis are the most common etiologies affecting the clavicle; and to a lesser extent, malignant lesions such as plasma cell neoplasms, Paget’s osteosarcomas, and metastatic tumors can also be present [1]. In this case report, we describe a case of atraumatic pathological clavicle fracture, as the first symptom of lung cancer.
Case Report
A 70-year-old male without significant medical history except for being a former smoker presented to our emergency service with the left shoulder pain for the past 2 weeks. The pain was located in the distal third of the clavicle, and there was no history of trauma.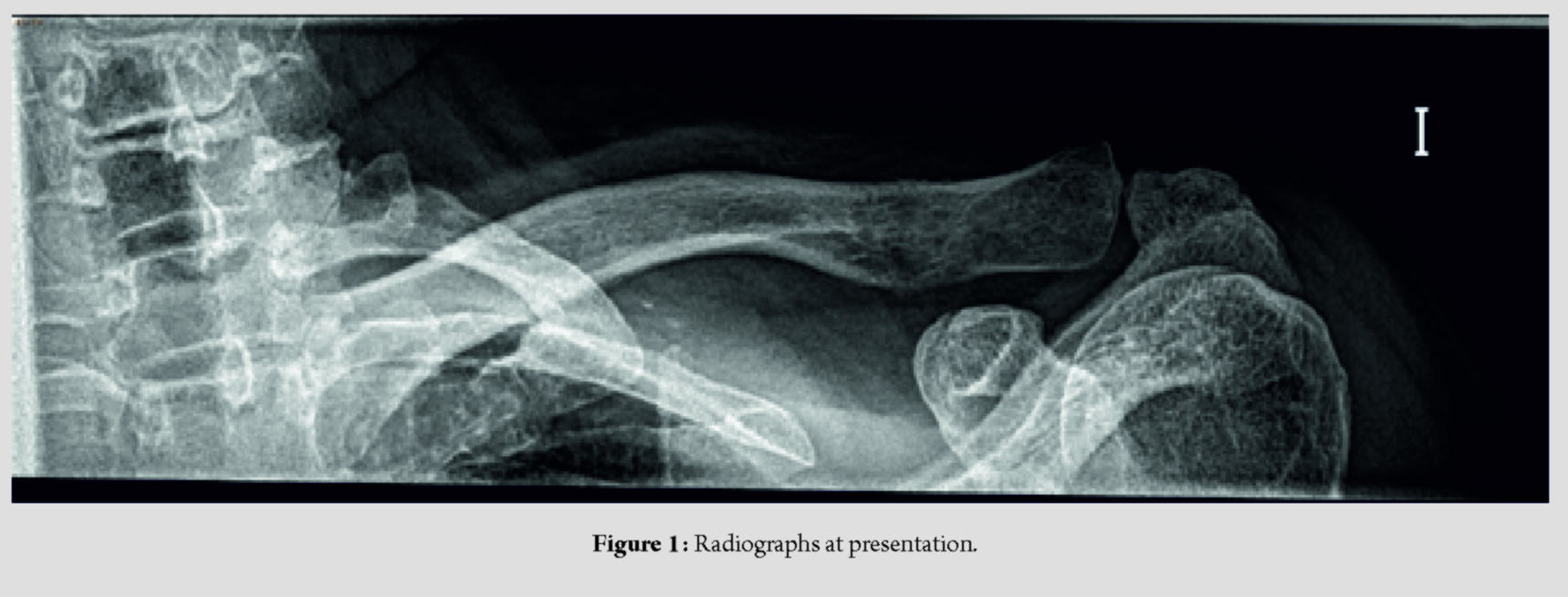
On examination, there was a significant pain on palpation in the distal third of the clavicle and acromioclavicular joint. Limited active range of motion (abduction of 100°, anteflexion 90°, external rotation of 20°, and internal rotation up to L3), and abnormal rotator cuff strength (4 of 5).There was no vascular or neurologic deficit. Standard two-dimensional radiographs were taken (Fig. 1), with an abnormal fracture of the lateral third of clavicle without clear traumatic history. Magnetic resonance imaging showed a fracture in the lateral third of clavicle accompanied by a soft tissue mass and bone edema (Fig. 2).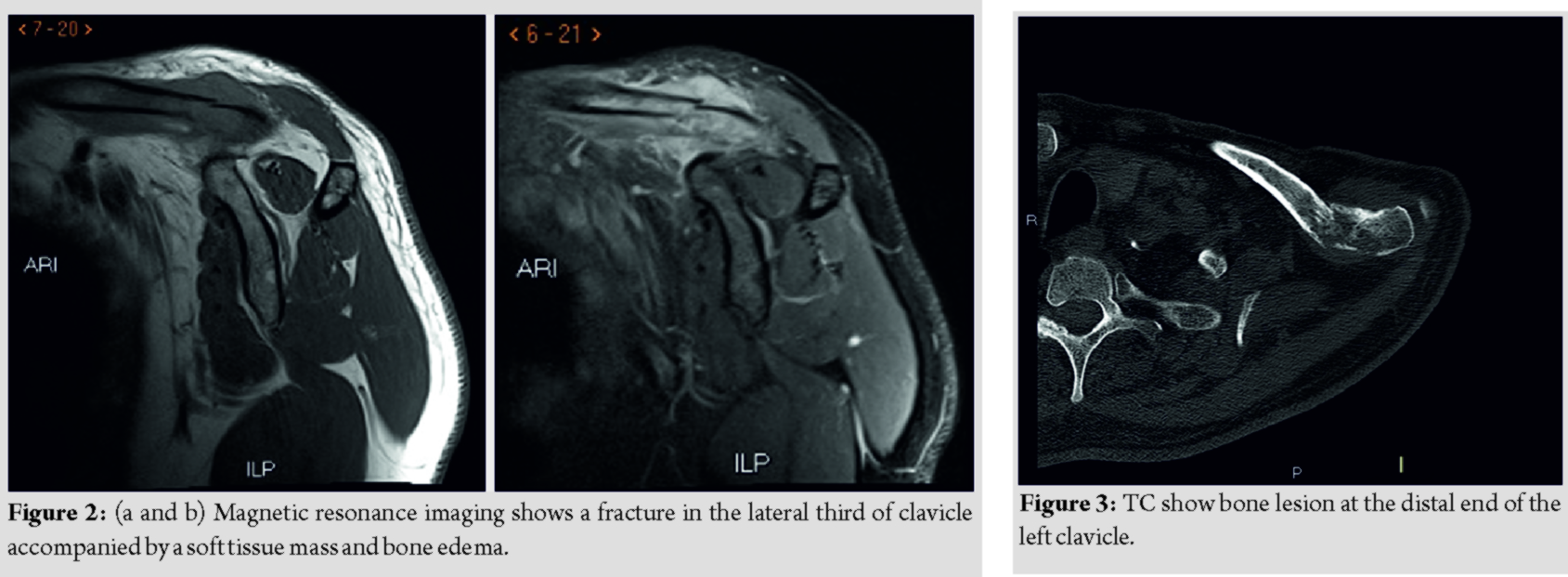
On suspicion of a pathological fracture, a positron emission tomography/computed tomography (PET-CT) scan was performed to further assess the lesion and as a staging study. It showed at the PET-CT appreciates metabolically active pulmonary mass in the left upper lobe, mediastinal and left hilar adenopathy, hepatic lesions, and a bone lesion at the distal end of the left clavicle (Fig. 3), left sternoclavicular joint, left the transverse process of the 8th vertebra, and right transverse process of the 9th vertebra. After having the staging studies, an ultrasound-guided biopsy was performed of the distal third clavicle lesion. The results of the biopsy came back compatible with a neuroendocrine carcinoma based on immunohisto chemical results (P63+, TTF1 -. CD56+ Ki67 80%). A transbronchial biopsy of the left upper lobe mass resulted in a small cell lung carcinoma. The patient was diagnosed with Stage IV advanced stage lung carcinoma and died 6 months after having with the pathological clavicle fracture.
Discussion
Shoulder pain is a very frequent medical condition, affecting patients over 40 years of age old. The origin of pain is usually multifactorial. In most of the cases, it is usually related to a rotator cuff pathology, although this is not always the case, other potential etiologies should be explored, especially within elderly population, as glenohumeral osteoarthritis and sternoclavicular osteoarthritis. The pain after a trauma can be due to different etiologies: Proximal humerus fractures, clavicle fracture, scapula fracture, traumatic rotator cuff tears, shoulder dislocation, or sternoclavicular dislocation. Proximal humerus fractures are a frequent pathology after low-energy traumas on osteoporotic bones or high-energy fractures in young people, its incidence increases in elderly people with osteoporotic bone, especially in women [2]. At present, there are many different treatment methods used, the main one is a conservative treatment through a short period of immobilization followed by physiotherapy, open reduction, and osteosynthesis with a plate or inverted shoulder arthroplasty [3]. Clavicle fractures are less frequent in elderly patients and are usually associated with direct trauma; clavicle fractures often affect young patients due to high-energy trauma. Traumatic tears of the rotator cuff are another cause of shoulder pain, the tears can be partial or total. The possibilities of surgical repair versus conservative treatment should be individualized according to the age, characteristics, and expectations of the patient [4]. Acromioclavicular dislocations and proximal biceps rupture are less frequent causes of post-traumatic shoulder pain in elderly patients, usually with self-limited pain. Pain without previous trauma is more frequent in elderly patient, with different causes responsible for this pain. Adhesive capsulitis is a cause of chronic and atraumatic pain, its cause is unknown although it is associated with diabetes mellitus. It is frequent in patients between 40 and 60 years of old, although independent insulin patients, it can debut at an earlier age. It consists of a painful and progressive limitation of the mobility of the shoulder and self-limiting in time [5]. Primary glenohumeral osteoarthritis is rare. The clinic of primary glenohumeral osteoarthritis is difficult to distinguish from cuff arthropathy, with night pain being less pronounced [6]. There are other causes of shoulder pain in the elderly that are much less frequent, such as cervical disc disease, fibromyalgia, CRMO, or both primary and secondary bone tumors. Bone metastases infrequently settle in the periscapular waist. Pathological clavicle fractures in elderly population are rare and when present should raise the possibility of underlying pathology [1]. Bone metastasis to the periscapular area isuncommon, and symptomatology related to them as an initial presentation of an oncological process is very unlikely with only few cases published [8, 9, 10, 11], in which metastatic renal cell carcinoma, as well as hepatocellular carcinoma, was commonly reported with no lung carcinomas present [8]. Atraumatic fractures in elderly patients are rare and should make us suspect an underlying pathology [1]. In patients with reverse total shoulder replacement, we can think of stress fractures, although it is a rare complication of reverse arthroplasty, it is more common in patients with rheumatic diseases, advanced osteoporosis, and high tension in the deltoid [7]. The pathological fracture of the clavicle as an initial symptom of an oncological process is very rare, few cases have been published, among them, there were primary renal carcinomas, hepatocellular carcinomas, and no lung carcinoma [8]. Focal, isolated, and non-traumatic clavicle lesions are rare as reported, the study by Suresh and Saifuddin[1]in which shows that four of 18of these lesions were metastases and none of them caused a pathological fracture [1]. For this reason, clavicle fractures are a less frequent cause of pain, and in elderly population, most likely is related to a pathological process as opposed to the younger population, in which high-energytrauma is usually the cause [3]. Bone metastases are relatively frequent in lung cancers, they are found in approximately 20–40% of cases, of which 80% appear at the time of diagnosis, although they can be detected at any stage of the disease [10]. The presence of bone metastases in patients with lung cancer is associated with a worse prognosis [11, 12, 13]. Even though, in approximately 20–40% of lung carcinomas, there is a metastatic bone disease which in up to 80% of the cases is found at the time of diagnosis, clavicular location as a pathological fracture has not been previously reported.
Conclusion
Clavicle focal pain without previous trauma is not very common, although different causes responsible for this pain and pathological fracture of the clavicle are very rare, we always have to think in pathological fracture of the clavicle in the differential diagnosis in patients with focal pain without traumatic event.
Clinical Message
We always have to investigate patients with focal pain without traumatic event around shoulder, although bone metastasis to the periscapular area is uncommon, we always have to include pathological fracture in the differential diagnosis.
References
1. SureshS, SaifuddinA. Unveiling the ‘unique bone’: A study of the distribution of focal clavicular lesions.Skeletal Radiol2008;37:749-56.
2. KannusP, PalvanenM, NiemiS, SievänenH, ParkkariJ. Rate of proximal humeral fractures in older Finnish women between 1970 and 2007.Bone2009;44:656-9.
3. FjalestadT, HoleMØ. Displaced proximal humeral fractures: Operative versus non-operative treatment–a 2-year extension of a randomized controlled trial.Eur J Orthop Surg Traumatol2014;24:1067-73.
4. PegreffiF, PaladiniP, CampiF, PorcelliniG. Conservative management of rotator cuff tear.Sports Med Arthrosc Rev2011;19:348-53.
5. GreenbergDL. Evaluation and treatment of shoulder pain.Med Clin North Am2014;98:487-504.
6. SinghJA, SperlingJ, BuchbinderR, McMakenK. Surgery for shoulder osteoarthritis.Cochrane Database Syst Rev2010;10:CD008089.
7. AnakwenzeOA, PiferMA, SinghA. Clavicle stress fracture after reverse shoulder arthroplasty.J Shoulder Elbow Surg2014;23:e170-2.
8. KongY, WangJ, LiH, GuoP, XuJF, FengHL. Pathological clavicular fracture as first presentation of renal cell carcinoma: A case report and literature review.Cancer Biol Med2015;12:409-12.
9. SmithJ, YuppaF, WatsonRC. Primary tumors and tumor-like lesions of the clavicle.Skeletal Radiol1988;17:235-46.
10. ThaiDM, KitagawaY, ChoongPF. Outcome of surgical management of bony metastases to the humerus and shoulder girdle: A retrospective analysis of 93 patients.Int Semin Surg Oncol2006;3:5.
11. KuchukM, AddisonCL, ClemonsM, KuchukI, Wheatley-PriceP. Incidence and consequences of bone metastases in lung cancer patients.J Bone Oncol2013;2:22-9.
12. CharpidouA, TsagouliS, GkiozosI, GrapsaD, MoutsosM, KiagiaM, et al. Bone metastases in patients with small cell lung carcinoma: Rate of development, early versus late onset, modality of treatment, and their impact on survival. A single-institution retrospective cohort study.Clin Exp Metastasis2016;33:453-60.
13. SagmanU, MakiE, EvansWK, WarrD, ShepherdFA, SculierJP, et al. Small-cell carcinoma of the lung: Derivation of a prognostic staging system.J Clin Oncol1991;9:1639-49.
14. NakazawaK, KurishimaK, TamuraT, KagohashiK, IshikawaH, SatohH, et al. Specific organ metastases and survival in small cell lung cancer.Oncol Lett2012;4:617-20.
 |
 |
 |
 |
 |
| Dr. David Gómez Garrido | Dr. Alfonso Prada Cañizares | Dr. Michele Bisaccia | Dr. Luigi Meccariello | Dr. Estefania Fernández Delgado |
| How to Cite This Article: Gómez Garrido D, Prada Cañizares, BisacciaM, Meccariello L, Fernándezz Delgado E. Pathological Clavicle Fracture as the First Symptom of Lung Cancer. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 54-57. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


