
[box type=”bio”] Learning Point of the Article: [/box]
Femoral head fracture ; Hip dislocation; Safe surgical dislocation of hip; Functional outcome.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 58-61 | Atul Gupta, Sunil Barod. DOI: 10.13107/jocr.2020.v10.i02.1696
Authors: Atul Gupta[1], Sunil Barod[1]
[1]Department of Orthopaedic Surgery, Barod Hospital, Indore, Madhya Pradesh, India.
Address of Correspondence:
Dr. Atul Gupta,
Department of Orthopaedic Surgery, Barod Hospital, AH 28,29 HIG Sukhliya, MR-10, Indore – 452010, Madhya Pradesh, India.
E-mail: guptaortho.in@gmail.com
Abstract
Introduction: Femoral head fractures are a rare pathology most often arising with high-energy traumas and associated with hip dislocations, which gravely compromise the ultimate functional outcome of the hip. Femoral head fractures without dislocation or subluxation are extremely rare injuries.
Case Report: A 23-year-old male who sustained a high-energy trauma due to road traffic accident. He presented to ER with fracture of shaft femur, multi-ligament injury at the ipsilateral knee, fracture lower pole patella, ipsilateral fracture talus, and calcaneus along with comminuted fracture femoral head. He was managed by open reduction and internal fixation of the femoral head by safe surgical dislocation of the hip joint. Such injuries have been described rarely in the literature until now. The purpose of this report is to highlight the extreme rarity, possible mechanism involved, surgical management, and functional outcomes of such injuries.
Conclusion: Femoral head fracture without dislocation is a very rare entity, early diagnosis, especially in high-energy trauma scenarios to prevent the neglect and delay in the treatment which is the paramount importance of an excellent result in young patients.
Keywords: Femur head, hip dislocation, safe surgical dislocation of hip, functional outcome.
Introduction
Femoral head fractures are a rare pathology most often arising with high-energy traumas and associated with hip dislocations, which gravely compromise the ultimate functional outcome of the hip. Femoral head fractures were described for the first time by Birkett [1] in 1869,subsequent to necropsy [1]. They are a rare type of injury, but their incidence has increased proportionally with the number of high-speed trauma, which is the most frequent etiological factor. Almost all cases of such fractures are associated with dislocation of the hip. In exceptional cases, this may occur without any dislocation[2, 3, 4]. Isolated femoral head fracture without hip dislocation is an extremely rare injury. An extensive review of the literature has revealed only two cases of isolated fracture of femoral head without any dislocation of the hip. One was a neglected case of femoral head fracture in a young patient, and another was by low-energy trauma [5, 6]. This type of fracture is extremely rare and surgical management is challenging. The aim was to highlight the extreme rarity of such injury, to suggest the possible mechanism, surgical management, and functional outcomes of such injury.
Case Report
A 23-year-old male sustained injury over the right lower limb as a result of high-velocity trauma (motorcycle-motorcycle collision). The patient suffered from severe pain, a deformity at mid-thigh and knee, and functional disability of the right leg along with wound over calf and ankle region (Gustilo-Anderson 3b).
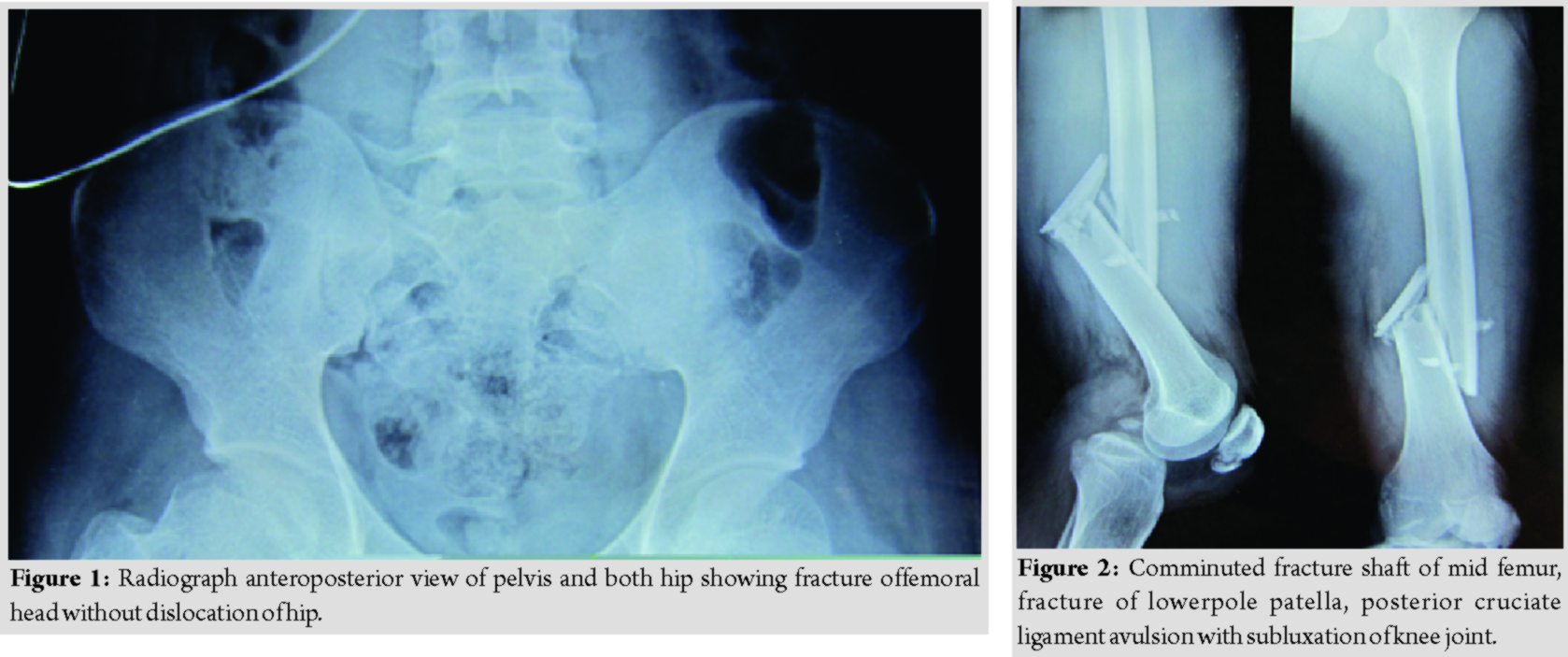
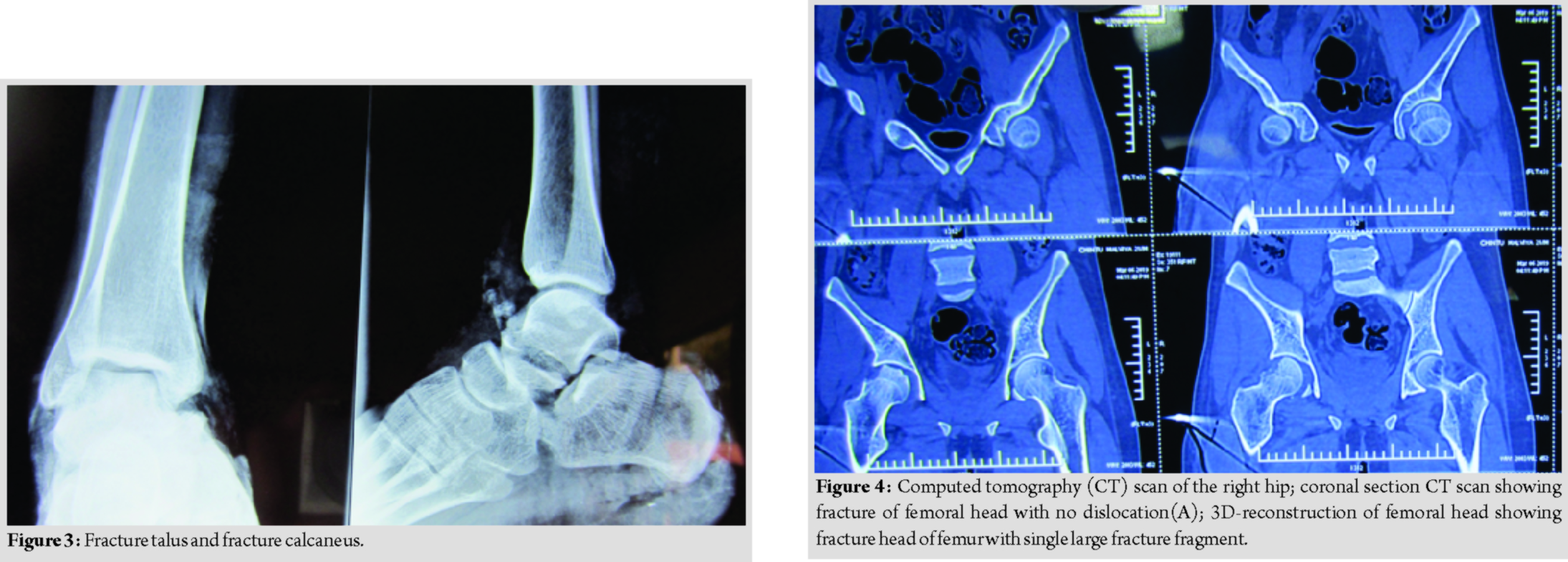
Radiographs done after primary resuscitation as per the standard protocol of advanced trauma life support. Radiographs revealed a fracture at the femoral head (Fig. 1), comminuted fracture Shaft of the mid femur, fracture of lower pole patella, posterior cruciate ligament avulsion with subluxation of the knee joint (Fig. 2), fracture talus, and fracture calcaneus (Fig. 3). There was no dislocation of the hip. Emergent ankle debridement was performed with stabilization of knee by upper tibial pin traction. A computed tomography scan of the right hip joint was done, which was suggestive of the femoral head fracture without dislocation or acetabular fracture (Fig. 4).
Femoral head fixation was performed after the fixation of fracture shaft femur by safe surgical dislocation of the hip approach. Intraoperative comminuted fracture of the femoral head(modified Pipkins type A-V) with avulsion of cartilage was found [5] (Fig. 5). The femoral head was approached by the method of safe surgical dislocation of the hip and fixation done with Herbert screws (Fig. 6).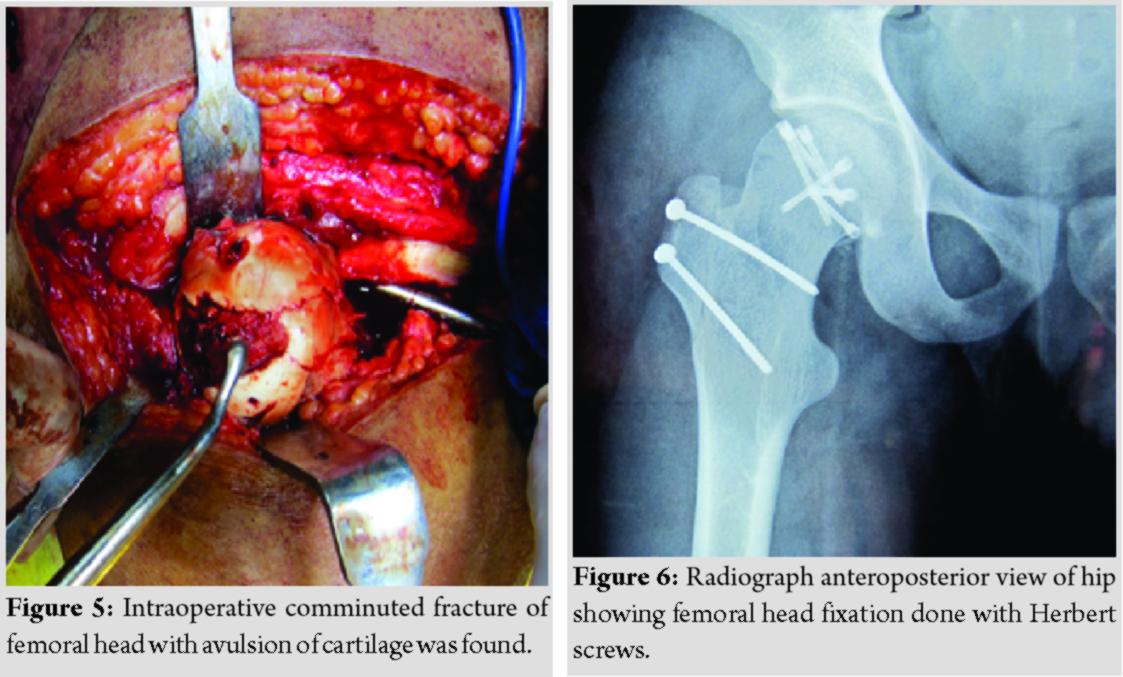
Discussion
Traumatic injuries of the hip joint are increasing in number due to road traffic accidents [7]. They are hip dislocations, dislocation with fractures, and fractures without dislocation. The lesions depend on the speed and direction of the injuries forces but also to the position of the hip at the time of impact. The position of the hip, such as adduction or abduction, flexion, and rotation, determines if the hip dislocates with or without fractures. The fractures can concern femoral neck, femoral head, greater trochanter, or posterior wall of the acetabulum. Hip dislocations associated with fractures have been described by many authors [2, 8, 9, 10]. Low-energy trauma in old age group or osteoporotic bones results in pertrochanteric femoral fractures, while low-energy trauma in young people with normal bones may fail to break the neck or trochanter of femur, instead of transmitting the injuring force to the femoral head. This would result in the fracture of the femoral head instead of the neck without dislocation of the hip. Femoral head fractures are relatively uncommon injuries, which occur in 5–15% of all hip dislocations [8]. Femoral head fractures are usually associated with hip dislocations. An extensive review of the literature has revealed only few cases of the femoral head fracture without hip dislocation published untildate [11, 12]. All these cases were associated with either fracture of the neck of the femur or fracture of the acetabulum. Kim et al. documented two cases of the femoral head fracture without dislocation of the hip. In case, one femoral head fracture was associated with fracture of the neck and intertrochanteric femur, while the other one was associated with fracture of the neck of femur. Mody and Wainwright reported two cases of the femoral head fracture without hip dislocation [13]. Both patients had low-energy trauma. Fabre et al. reported a case of comminuted fracture of the femoral head and neck and acetabulum without dislocation of the hip following a high-energy trauma [12]. Aggarwal documented a 1-year-old neglected case of the femoral head fracture without dislocation of the hip in young male following high-energy trauma [5]. Among all the previous cases were managed by either total hip replacement or conservative management. In our case, femoral head fracture without dislocation might have occurred probably due to high-energy impact on the femoral head with force acting along with the long axis of the fractured femoral shaft. We managed the femoral head fracture by safe surgical dislocation of hip technique and fixed with multiple Herbert screws. The possibility of fracture of the femoral head should be kept in mind, especially in high energy trauma, polytrauma patients to prevent the neglect, and delay in treatment. The purpose of this case study is early diagnosis of fracture of the femoral head in high-energy trauma without dislocation of the hip joint. We emphasize that traumatic hip fracture without dislocation is rare entities, early diagnosis and prompt management are the key determinant of an excellent result.
Conclusion
Femoral head fracture without dislocation is a very rare entity, most among them are either associated with pertrochanteric femur fracture or are neglected. Fracture of femoral head should be evaluated early, especially in high-energy trauma scenario, to prevent the neglect and delay in the treatment which is the paramount importance for an excellent result in young patients.
Clinical Message
Traumatic hip fracture without dislocation is rare entities, early diagnosis and prompt management are the key determinants of an excellent result.
References
1. Birkett J. Description of a dislocation of the head of the femur, complicated with its fracture; with remarks. Med Chir Trans 1869;52:133-8.
2. Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. In: The Hip Society, editor. Proceeding of the Hip Society. St. Louis: Mosby; 1986. p. 181-206.
3. Lafosse JM, Besombes C, Chiron P, Tricoire JL. Luxation et fracture de la tête fémorale. Hip 2002;???:67-80.
4. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39-A:1027-42.
5. Aggarwal AK, Soni A, Singh D. Femoral head fracture without hip dislocation. Chin J Traumatol 2013;16:304-7.
6. Yoon PW, Jeong HS, Yoo JJ, Hoo KH, Yoon KS, Kim HJ. Femoral head fracture without dislocation by low-energy trauma in a young adult. ClinOrthopSurg 2011;3:336-41.
7. Bauer GJ, Sarkar MR. Injury classification and surgical approach in hip dislocationsand fractures. Orthopade 1997;26:304-16.
8. Hougaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg Am 1988;70:233-9.
9. Roeder LF, Delee JC. Femoral head fractures associated with posterior hip dislocation. ClinOrthopRelat Res 1980;147:121-30.
10. Elmrini A, Daoudl A, Agoumi O, Boutayeb F, Mahfoud M. Isolated fracture of the femoral head. J Orthopaedics 2006;3:???.
11. Kim KI, Koo KH, Sharma R, Park HB, Hwang SC. Concomitant fractures of the femoral head and neck without hip dislocation. ClinOrthopRelat Res 2001;391:247-50.
12. Fabre A, Bures C, Levadoux M, Leguilloux P, Rigal S. A comminuted femoral head fracture without hip dislocation. Eur J OrthopSurgTraumatol 2003;13:166-8.
13. Mody BS, Wainwright AM. Fracture of the femoral head without associated hip dislocation following low-energy trauma. A report of two cases. Arch Orthop Trauma Surg 1996;115:300-2.
 |
 |
| Dr. Atul Gupta | Dr. Sunil Barod |
| How to Cite This Article: Gupta A, Barod S. Femoral Head Fracture without Dislocation of Hip in a Young Adult: A Case Report. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 58-61. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


